1.22: Thyroglossal Duct Cyst
- Page ID
- 17640

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
THYROGLOSSAL DUCT REMNANTS
Johan Fagan
The surgical management of thyroglossal duct remnants (TGDRs) requires an understanding of the embryology of the thyroid gland, as failure to include the embryological course of the thyroid gland in the surgical resection increases the probability of recurrence.
Relevant Embryology
The thyroid gland originates in the base of the tongue at the foramen caecum. In early embryonic life the base of the tongue is adjacent to the pericardial sac. As the embryo unfolds, TGDRs may remain anywhere between the pericardial sac and the foramen caecum. A persistent thyroglossal duct courses through the base of the tongue from the foramen caecum. It then passes inferiorly, anterior to, and rarely through, the hyoid body, and often has a diverticulum that hooks below and behind the hyoid, before it courses towards a thyroglossal duct cyst or the thyroid gland (Figure 1).
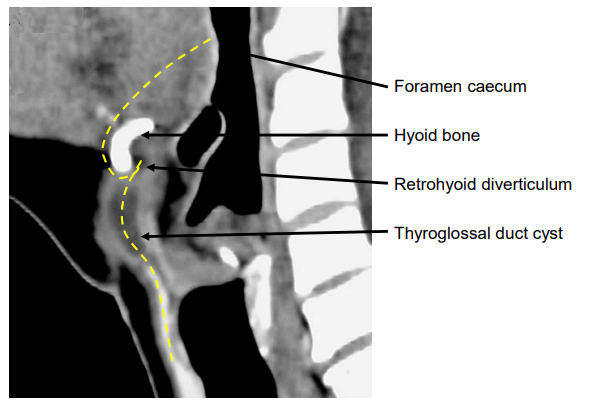
Figure 1: Typical course of thyroglossal duct remnants (yellow line)
The suprahyoid ductal segment may have a branching pattern like the tips of a broom (Figure 2). These multiple ductules communicate with secretory glands in the base of the tongue and might drain directly into the mouth.1
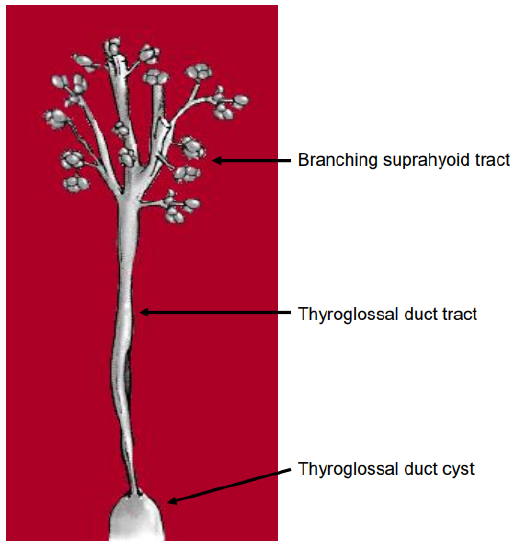
Figure 2: Schematic representation of the suprahyoid duct branching within the muscle of the base of tongue
Clinical presentation
TGDRs may present at any age as a cyst (Figure 3, 4), abscess, sinus, fistula or tumor, anywhere along the embryological course of the thyroid gland.
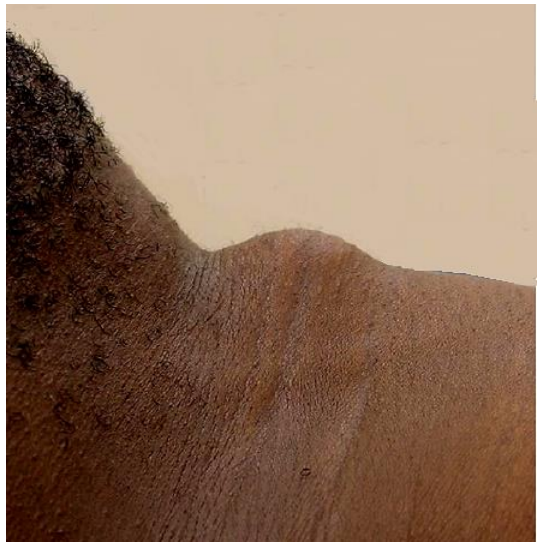
Figure 3: Thyroglossal duct cyst in thyrohyoid region
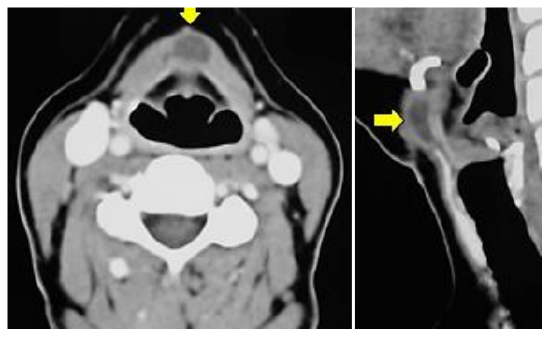
Figure 4: Thyroglossal duct cyst in thyrohyoid region
Patients classically present with a mobile, painless mass in the midline of the neck in proximity of the hyoid bone. Occasionally a cyst may be off the midline (Figures 5, 10).
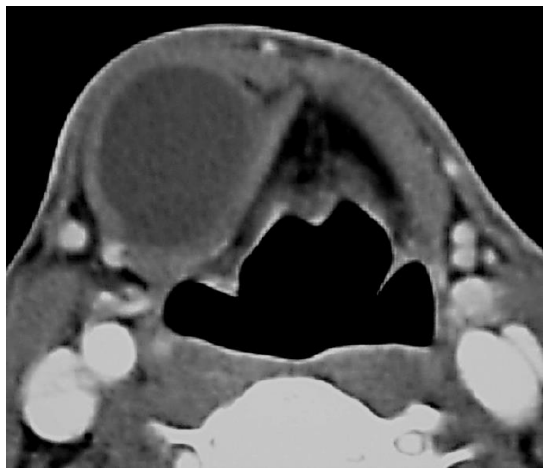
Figure 5: Thyroglossal duct cyst to left of midline overlying lamina of thyroid cartilage
Figure 6 illustrates the distribution of thyroglossal duct cysts.1
A cyst generally moves upward during deglutition or protrusion of the tongue because of its close anatomical relation to the hyoid bone. This is considered a reliable diagnostic sign as it distinguishes it from other midline neck masses such as a lymph node or a dermoid cyst (Figure 7).
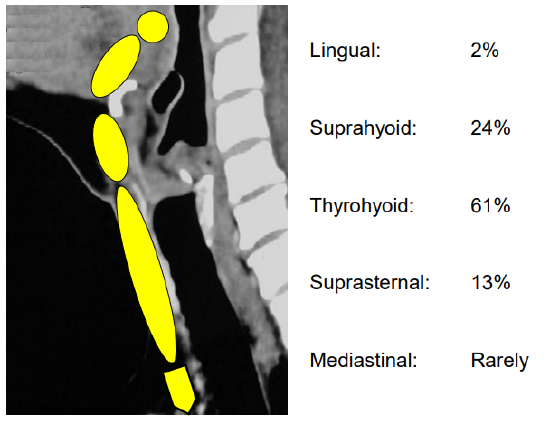
Figure 6: Distribution of thyroglossal duct cysts
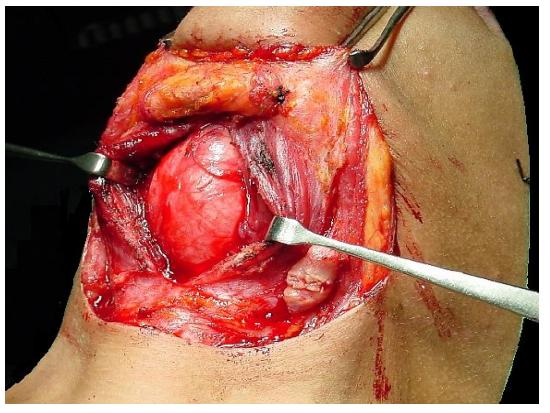
Figure 7: Dermoid cyst
A lingual thyroid usually presents as a mass in the base of the tongue (Figures 8, 9); this may be the patient’s only thyroid tissue in the majority of cases.
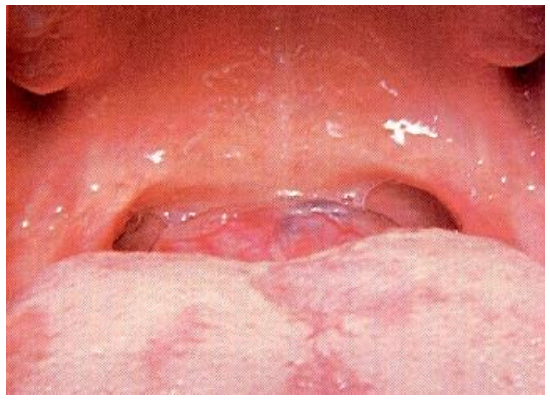
Figure 8: Lingual thyroid
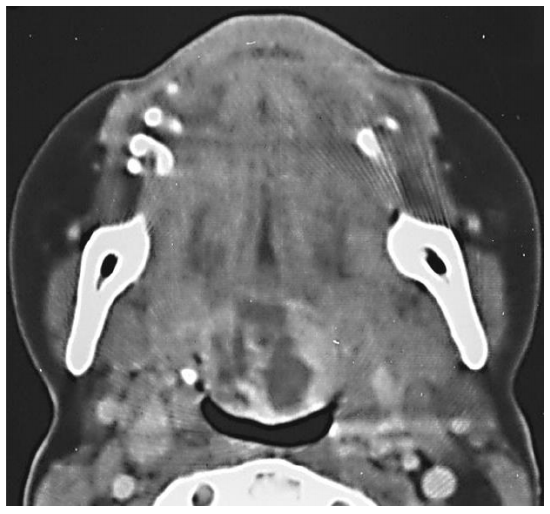
Figure 9: CT scan of lingual thyroid
Preoperative evaluation
The principal issues to determine prior to surgery are:
Is it a TGDR? Unlike other midline masses, only TGDRs are treated with a Sistrunk operation. Therefore, it is important to exclude other causes of midline masses prior to surgery such as dermoid cysts and lymph nodes.
Is it the patient’s only thyroid tissue? Occasionally a TGDR comprises the only functioning thyroid tissue, and its removal results in hypothyroidism. Ultrasound examination to establish the presence of normal thyroid tissue is a simple investigation. Should imaging not be possible, the surgeon should explore the neck to determine the presence of a normal thyroid gland.
Is the patient hypothyroid? The majority of patients with lingual thyroids are hypothyroid. Therefore patients with lingual thyroids should have a TSH level determined prior to surgery.
Does the TGDR contain thyroid cancer? Thyroid cancer occurs in only about 1% of operated TGDRs. A solid component and/ or calcification on ultrasound examination should raise the possibility of carcinoma, most commonly papillary. However, even if the diagnosis of thyroid cancer is suspected it does not alter the type of surgery (Sistrunk operation).
Surgical principles
- It is imperative to achieve a complete resection of the TGDR and its embryonic tract to avoid symptomatic recurrence
- A thyroglossal cyst abscess should initially be aspirated and treated with antibiotics, not incised and drained, to facilitate complete resection once the infection has settled
Sistrunk operation
The Sistrunk operation is the standard of care for TGDRs. It includes resection of entire embryological tract i.e. the thyroglossal duct cyst, the central portion of the body of the hyoid bone, and a broad (>1 cm) core of suprahyoid muscle extending up to / close to the foramen caecum.
The following description is for a cyst in the thyrohyoid region:
- Make an incision in a skin crease over the cyst. Note that the platysma muscle may be absent in the midline, so take care not to puncture the cyst (Figure 10)
- Raise superior and inferior flaps in subplatysmal planes. The superior flap should be raised to approximately 2 cm above the body of the hyoid bone
- Identify the infrahyoid strap muscles that are stretched over the superficial aspect of the cyst
- Divide the cervical fascia vertically in the midline, separate the infrahyoid strap muscles, and expose the cyst (Figure 11)
- Divide the mylohoid and geniohyoid muscles just above the body of the hyoid bone with diathermy remaining between the lesser cornua of the hyoid so as not to place the hypoglossal nerves or lingual arteries at risk of injury (Figure 12)
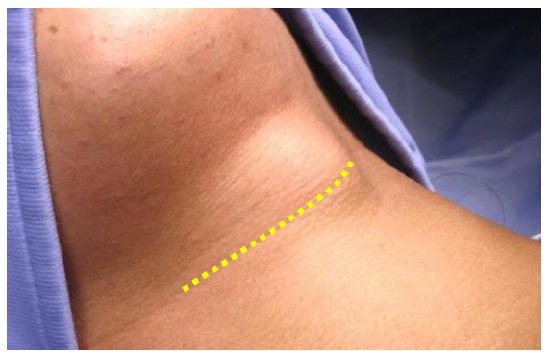
Figure 10: Initial skin crease incision
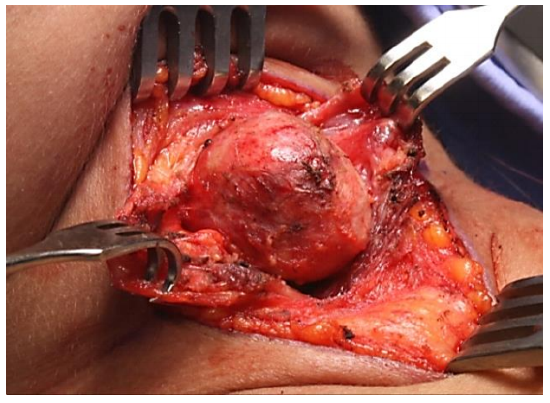
Figure 11: Expose and part infrahyoid strap muscles overlying cyst
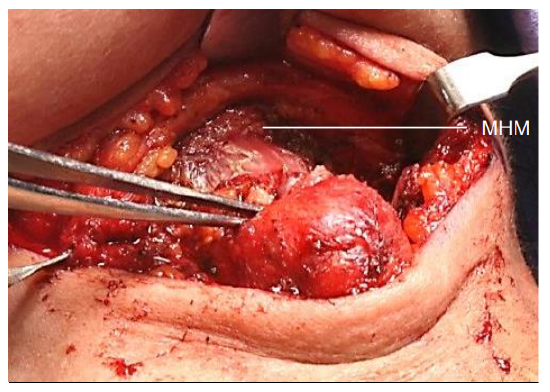
Figure 12: Divide mylohoid (MHM) and geniohyoid muscles just above body of hyoid bone
- Divide the inferior attachments of the thyroglossal duct cyst, and mobilize the deep aspect of the cyst from the thyrohyoid membrane up to the hyoid bone with sharp dissection (Figure 13)
- Expose the hyoid bone on either side of the cyst (Figure 14)
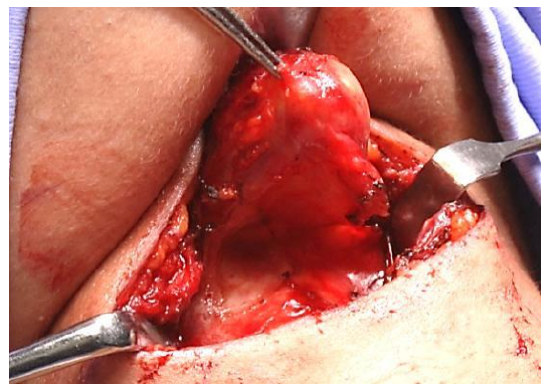
Figure 13: Mobilize deep aspect of cyst from thyroid cartilage and thyrohyoid membrane
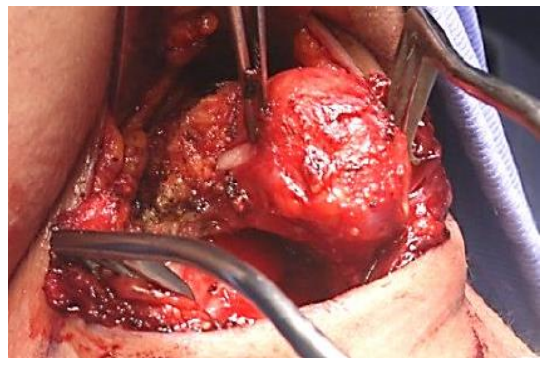
Figure 14: Expose hyoid bone on either side of cyst
- Divide the hyoid bone about 1 cm to each side of the midline with heavy scissors (children) or a bone cutter (Figures 15, 16)
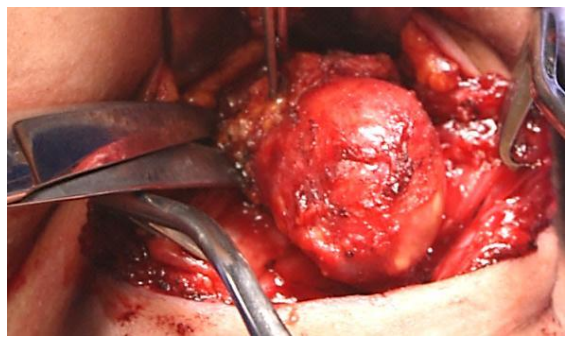
Figure 15: Dividing hyoid bone
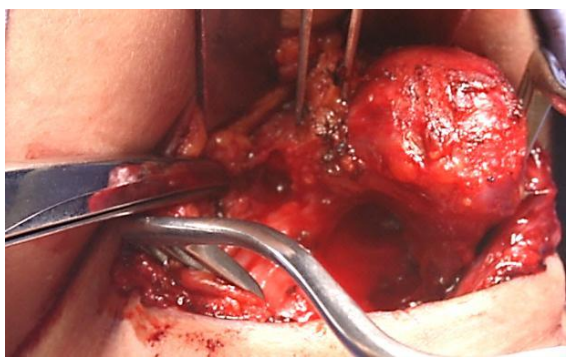
Figure 16: Divided hyoid bone
- Next resect the suprahyoid thyroglossal duct. Do not attempt to identify the thyroglossal duct, as branches of the duct may be transected in the process increasing the likelihood of recurrence
- Using monopolar diathermy resect a 2 cm wide core of tongue tissue (hyoglossus) in continuity with the remainder of the operative specimen, including the hyoid bone, directed at an angle of approximately 45o in the sagittal (vertical) plane towards the foramen caecum (Figures 17, 18, 19)
- If in doubt about the required direction, place a finger in the mouth and on the foramen caecum as a guide. It is remarkable how much base of tongue tissue can be resected without interfering with speech or swallowing. Note the proximity of the hyoid bone to the vallecula. Should the vallecula or base of tongue be accidentally entered, simply close the defect with vicryl sutures from the neck side.
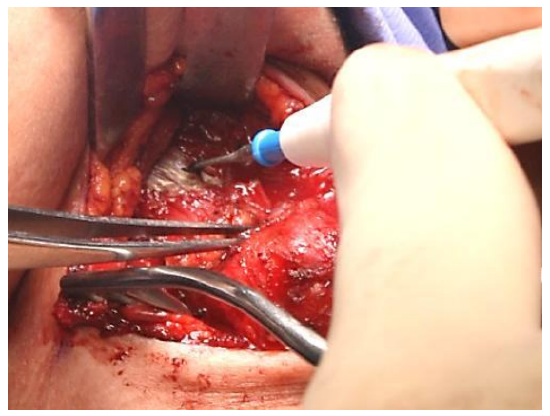
Figure 17: Resect a 2 cm wide core of tongue (hyoglossus) tissue

Figure 18: Superimposed image (yellow) illustrates direction of suprahyoid dissection and extent of final resection; note proximity of vallecula to hyoid
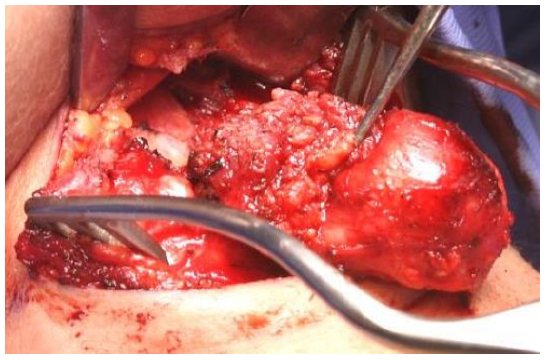
Figure 19: Core of tongue (hyoglossus) tissue extending up to just short of foramen caecum
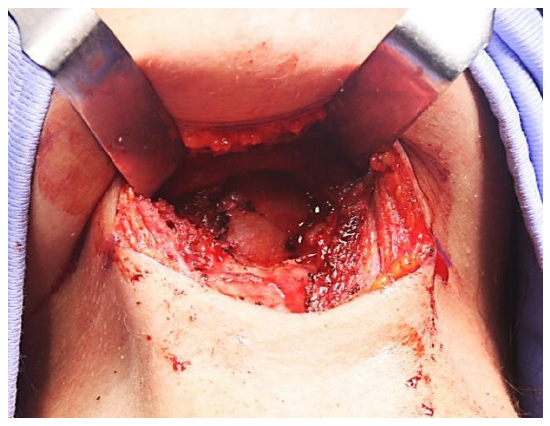
Figure 20: Final defect in base of tongue up to just short of forman caecum with free floating cut ends of hyoid bone
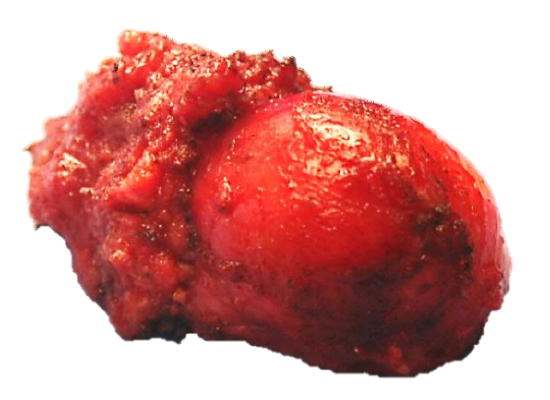
Figure 21: Resected specimen
- The tongue defect (Figure 20) is then partially obliterated with vicryl sutures. The two cut ends of the hyoid are not approximated, but left floating free. The supra- and infrahyoid muscles are approximated in a transverse plane, as is the platysma muscle, and the skin is closed over a drain
- Antibiotics are not required unless the oral cavity has been entered
Recurrent TGDR
Managing recurrent TGDR becomes challenging because cysts may be multifocal with the presence of fibrosis, distorted surgical landmarks and possible absence of hyoid bone. It is important to obtain an accurate description of the original surgery to determine whether the hyoid bone and suprahyoid tissues had been resected. An MRI scan should be done to serve as a roadmap for the surgeon to find residual TGDRs (Figure 21).
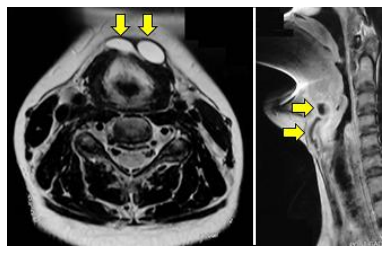
Figure 22: MRI of recurrence demonstrating multiple cysts
Reference
Mondin V, Ferlito A, Muzzi E, Silver CE, Fagan JJ, Devaney KO, Rinaldo A. Thyroglossal duct cyst: Personal experience and literature review. Auris Nasus Larynx 35 (2008) 11–25
Author & Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za

The Open Access Atlas of Otolaryngology, Head & Neck Operative Surgery by Johan Fagan (Editor) johannes.fagan@uct.ac.za is licensed under a Creative Commons Attribution - Non-Commercial 3.0 Unported License