
9.2: Tubes and Catheters
- Page ID
- 14834

All inserted or implanted medical devices have some form of identifiable markings embedded in them that allows for localization of the device on radiographs. X-ray imaging is the best modality for localization and identification of these types of medical devices.
Tubes and Catheters
Endotracheal Tube
An endotracheal tube (ET) helps to provide gases to the lungs in a controlled manner. It can also be used to suction secretions from the airways.
The tube should be in the upper trachea, roughly 3 cm from the carina, and not enter the right or left main stem bronchus. There is a small amount of mobility of the tube noted if the neck is flexed or extended. The endotracheal tube must be closely monitored and daily radiographs are recommended.
ODIN Link for Endotracheal tube, Figure 9.3: mistr.usask.ca/odin/?caseID=20150915221432751
The endotracheal tube is in excellent position, distal to the upper trachea and within 3 cm of the carina. The tube is well centered in the trachea.
Tubes and Catheters
Central Venous Catheters
Any venous catheter placement that results in the tip of the catheter being positioned in the superior or inferior vena cava can be considered to be a central venous catheter.
There are a variety of routes that one can employ to allow the catheter tip to be centrally positioned. The venous access site may be limited due to the type and size of the device i.e. large caliber dialysis type catheters cannot be implanted in the basilic vein.
Best practices dictate that access to the venous system for central vein catheterization should be guided by ultrasound, if possible. Use of this technology helps to diminish the risk of inadvertent arterial injury and other adverse events related to inappropriate insertion needle trajectory.
For catheters implanted in the superior vena cava (SVC), the optimal landing point for the catheter tip is considered to be in the SVC just cranial to the right atrium.
ODIN Link for Internal Jugular, Figure 9.4A: mistr.usask.ca/odin/?caseID=20170407155334051

Internal Jugular Line – The image demonstrated a large caliber catheter the enters into the right neck and terminates with the tip overlying the SVC-Right atrial junction.
ODIN Link for Subclavian Line, Figure 9.4B: mistr.usask.ca/odin/?caseID=20170407155825956

Subclavian Line – There was a medium size catheter seen paralleling the under surface of the right clavicle and terminating with the tip overlying the lower mediastinum.
ODIN Link for PICC, Figure 9.4C: mistr.usask.ca/odin/?caseID=20150605095210559

PICC – There was a small caliber catheter that entered from the left arm and teminated with the tip superimposed on the SVC-Right atrial junction.
Tubes and Catheters
Nasogastric – Orogastric Tubes
Naso-Orogastric tubes are inserted to allow for the suctioning of the stomach or for the administration of medications and feeding solutions.
Optimally, they should be positioned 8 – 10 cm beyond the gastro-esophageal junction, in the stomach, without any kinks.
These tubes come in different sizes and lengths. They are radio-opaque to make them visible on radiographs. Local policies and procedures for placement and verification of tube placement should be consulted.
ODIN Link for Nasogastric Tube, Figure 9.5: mistr.usask.ca/odin/?caseID=20170116144501259
This radiograph excluded the anatomy of the upper hemithoraces. There was an NG tube seen that coils in the left upper quadrant of the abdomen. The NG tube was satisfactory in appearance.
ODIN Link for Feeding Tube, Figure 9.6: mistr.usask.ca/odin/?caseID=20151023225106034

This radiograph excludes the anatomy of the upper hemithoraces. There was a weighted feeding tube seen in the left upper quadrant. The tube was beyond the GE junction.
Tubes and Catheters
Chest Drains
Chest drains are most often placed in the pleural space to drain air or fluid (blood, chyle, pus, transudate).
The tube must have sufficient caliber to handle the substance to be drained i.e. larger tubes for thick, viscous fluid. Tubes should be monitored with sequential radiographs to ensure stable position and adequate function. If the drainage tube has side holes, these must be inside the pleural boundary or the pleural contents will leak into the chest wall (subcutaneous emphysema, chest wall fluid).
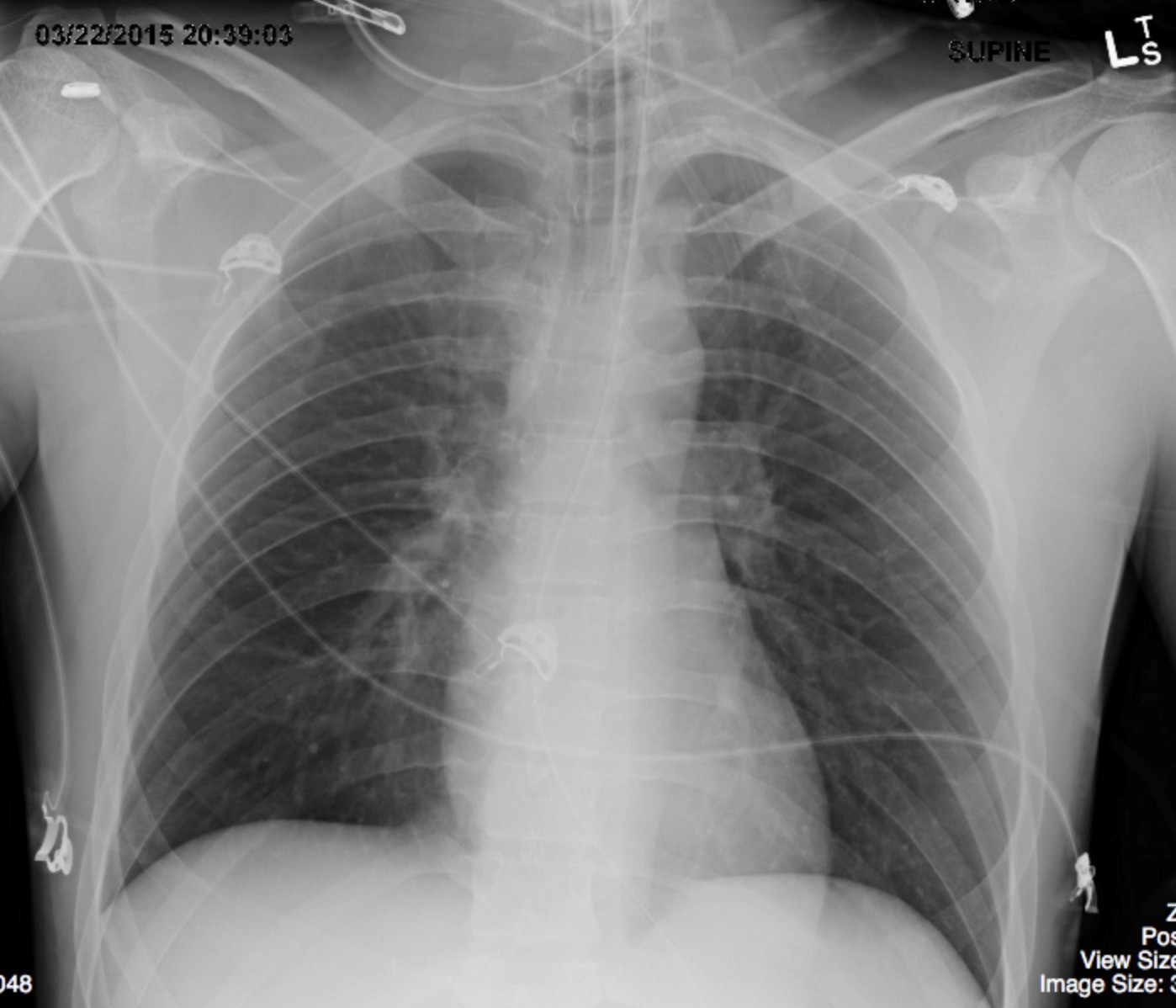
ODIN Link for Pleural Drains, Figure 9.7: mistr.usask.ca/odin/?caseID=20170117225944372
There were solitary, large caliber pleural drainage catheters in each hemithorax. The discontinuity in the white marker strip on the tube reveals that the side hole for each drain was well within the margin of the rib cage. The tubes were not kinked. Minimal, residual, pleural fluid was present bilaterally.
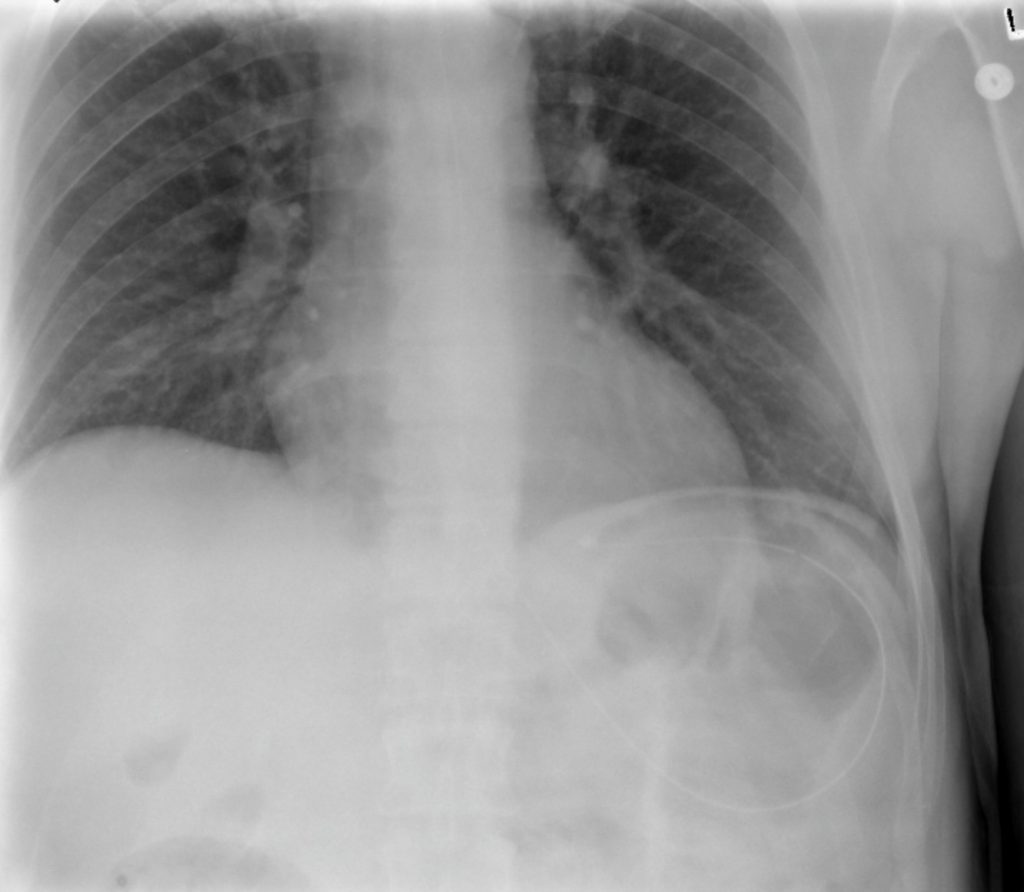
ODIN Link for Pleural Pigtails (Pre and Post-Insertion with Ultrasound), Figure 9.8: mistr.usask.ca/odin/?caseID=20170226235030319

There were solitary, bilateral, small caliber, pigtail type, pleural drains present. The patient made a poor inspiration for the radiograph. Minimal pleural fluid was seen. The patient had a known right aortic arch. The pleural effusions and basilar atelectasis have improved from previous images.
Attributions
Figure 9.3 X-ray of Endotracheal Tube by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
Figure 9.4A Internal Jugular Line by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
Figure 9.4B Subclavian Line by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
Figure 9.4C PICC – Peripherally Inserted Central Vein Catheter by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
Figure 9.5 Nasogastric Tube – Salem Sump – for Stomach Suction by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
Figure 9.6 Nasogastric Feeding Tube by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
Figure 9.7 Large Caliber Pleural Drains (bilateral) by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
Figure 9.8 Pigtail Pleural Drains (bilateral) by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.