
10.3: Ileus
- Page ID
- 14846

ACR – Gastrointestinal – Acute (non-localized) Abdominal Pain and Fever
Case 1
Adynamic, Generalized Ileus
Clinical:
History – This patient had surgery 2 days prior to these images for a ruptured appendix.
Symptoms – Vague abdominal pain, low-grade fever (37.9C), Not passing flatus or stool for 2 days.
Physical – The abdomen was mildly distended. The laparoscopic access sites were normal. There was a paucity of bowel gas sounds. No focal tenderness, guarding or rebound.
DDx:
Ileus
Small bowel obstruction
Abscess
Large bowel obstruction
Imaging Recommendation
ACR – Gastrointestinal – Acute (non-localized) Abdominal Pain and Fever, Variant 1
Three views of the abdomen – supine, upright, and right side up decubitus view.
CT Abdomen
ODIN Link for Adynamic Ileus images (3 Views of the Abdomen), Figure 10.4A and B: mistr.usask.ca/odin/?caseID=20160412201915071

Imaging Assessment
Findings:
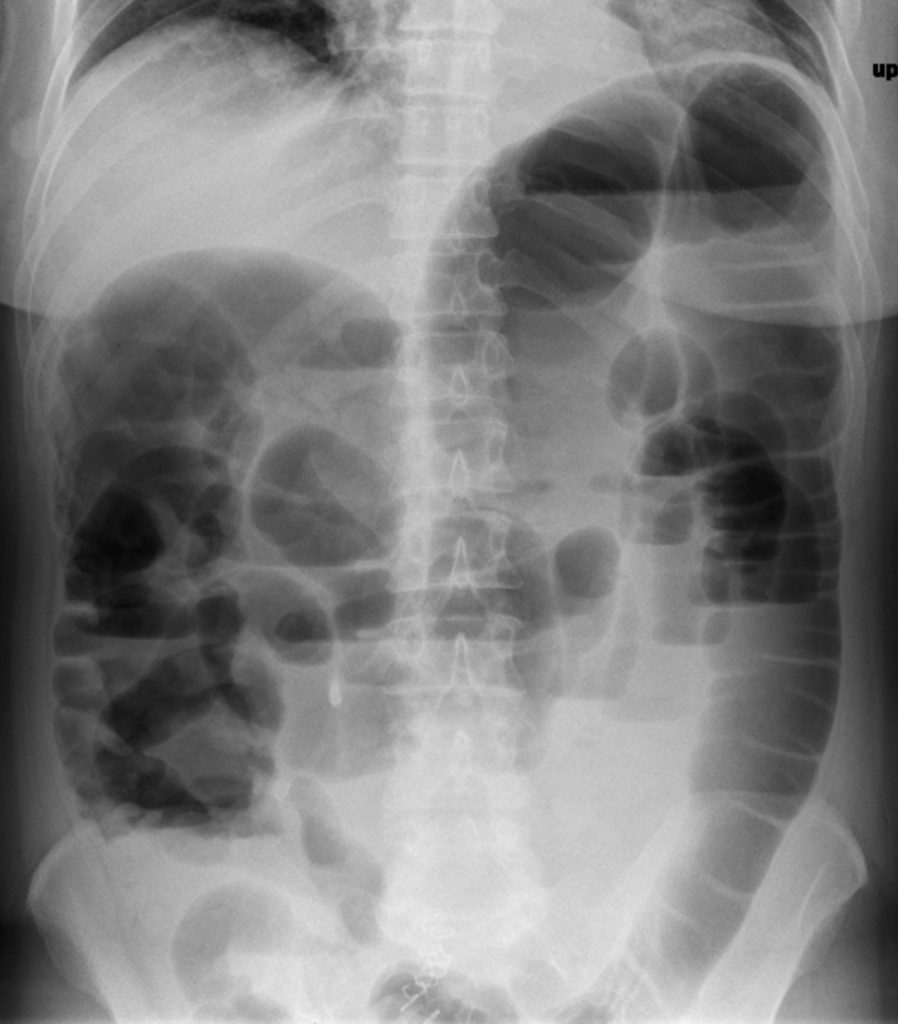
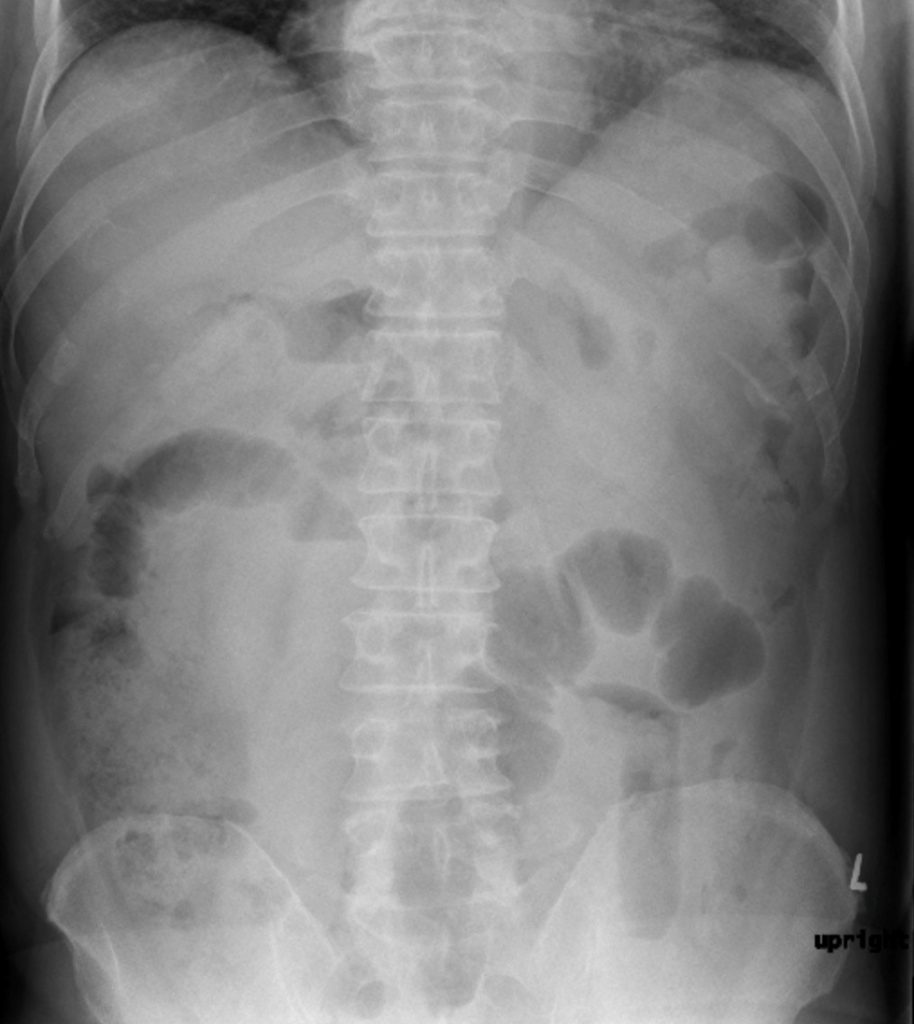
No free intraperitoneal gas. No extra-intestinal gas pattern to suggest an abscess. There was atelectasis in the left lower lung. The bowel, small and large, was diffusely, mildly, dilated. There were several small bowel air-fluid levels. No other findings.
Interpretation:
Left lower lobe atelectasis. Adynamic ileus.
Diagnosis:
Adynamic, Generalized Ileus
Discussion:
Ileus can be Generalized or Localized.
Dilated small bowel is wider than 3 cm in diameter. Small bowel dilation related to an ileus usually does not dilate as greatly as that seen in mechanical bowel obstruction.
Generalized – Adynamic Ileus
Seen in the setting of post-operative abdomen/pelvis and Diabetic Ketoacidosis
The entire bowel is aperistaltic or hypoperistaltic. Swallowed air dilates, and fluid fills most loops of both small and large bowel.
A generalized adynamic ileus is almost always the result of abdominal or pelvic surgery, in which the bowel is manipulated during the surgery.
Localized Ileus
Localized relates to something in the abdomen that has the capacity to affect a segment of bowel and result in hypoperistalsis and dilation of a localized region of intestine. This is most often seen associated with an adjacent pathology i.e. pancreatitis, inflammatory bowel disease, contained perforation (abscess), diverticulitis, or appendicitis.
X-ray findings may include:
- One, or two, persistently dilated segments of bowel (usually small bowel). Persistently means that these segments remain dilated on multiple views of the abdomen (supine, prone, upright abdomen) or on serial studies done over the course of time.
- Infrequently, the sentinel segment may be large bowel, rather than small bowel. This can especially occur in the cecum, with diseases such as appendicitis.
- Air–fluid levels may be seen in sentinel segment.
- There may be gas in the rectum or sigmoid colon.
Case 2
Localized Ileus/Sentinel segment
Clinical:
History – This patient had a history of Crohn’s disease. She was not currently on any medications for this condition. She was experiencing increasing abdominal pain and bloody diarrhea.
Symptoms – Moderate abdominal pain, localized to the right lower quadrant, low-grade fever (37.9C).
Physical – The abdomen was mildly distended. There was a paucity of bowel gas sounds. Focal tenderness was elicited in the right lower quadrant.
DDx:
Ileus
Small bowel obstruction
Abscess
Large bowel obstruction
Imaging Recommendation
ACR – Gastrointestinal – Acute (non-localized) Abdominal Pain and Fever, Variant 1
Three views of the abdomen – supine, upright, and right side up decubitus view.
CT Abdomen
ODIN Link for Localized Ileus images (3 Views of the Abdomen), Figure 10.5A and B: mistr.usask.ca/odin/?caseID=20170410095031868
Imaging Assessment
Findings:
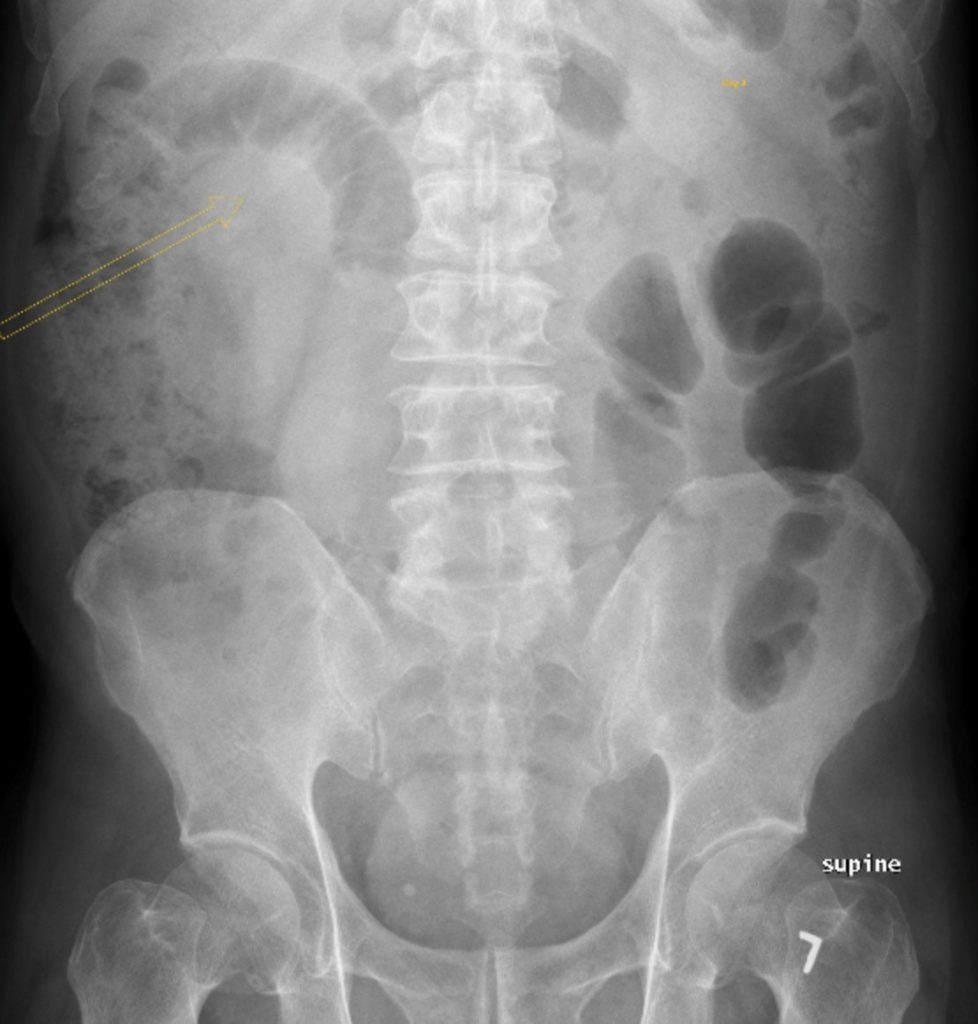
No free intraperitoneal gas. No extra-intestinal gas pattern to suggest an abscess. There was a localized, persistently dilated, segment of small bowel in the right mid to lower abdomen. This was seen on the supine and upright views, unchanged in the interval between the two images. There was no evidence of air/fluid levels or dilated bowel elsewhere. No other findings.
Interpretation:
Localized, right abdominal, ileus.
Diagnosis:
Localized Ileus. Active Crohn’s disease effecting the terminal ileum.
Attributions
Figure 10.4A Abdominal x-ray, supine, revealing mild, generalized bowel dilation, generalized ileus by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
Figure 10.4B Abdominal x-ray, upright, revealing mild, generalized bowel dilation, generalized ileus by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
Figure 10.5A Abdominal x-ray, supine, suspicious for localized ileus in right upper quadrant by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.
Figure 10.5B Abdominal x-ray, upright, suspicious for localized ileus by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC-BY-NC-SA 4.0 license.