
4.17: Carpal Tunnel Syndrome
- Page ID
- 59242
Carpal tunnel syndrome is a condition characterized by tingling, numbness and pain in the hand and fingers (particularly the thumb, index, middle and ring fingers). These symptoms are often the result of median nerve irritation in the wrist or forearm.
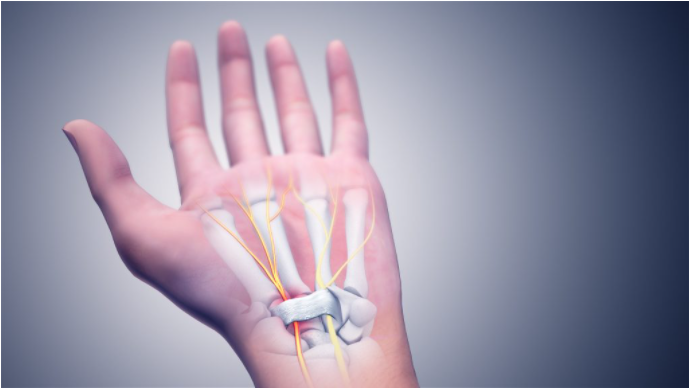
Carpal tunnel syndrome is a condition characterized by tingling, numbness, and pain in the hand and fingers (particularly the thumb, index, middle, and ring fingers).
Pathophysiology
The median nerve passes through several anatomical structures and it may be exposed to mechanical irritation at many different points. Prolonged irritation of a peripheral nerve triggers the release of inflammatory mediators, known as “neurogenic inflammation”; this noxious substance can disrupt the normal function of nerves. Ongoing tissue hypoxia or inflammatory responses lead to molecular signaling that promote the development of fibrosis, this may contribute to further peripheral nerve dysfunction (Barbe et al., 2020; Bove et al., 2019).
Clinical Examination
A thorough health history intake can be done to gather information about patients’ limitations, course of pain, and prognostic factors for delayed recovery (e.g., low self-efficacy, fear of movement, ineffective coping strategies, fear-avoidance, pain catastrophizing) and answers to health-related questions. Screen patients to identify those with a higher likelihood of serious pathology/red flag conditions. Then undertake a physical examination: neurological screening test, assess mobility and/or muscle strength.
Outcome Measurements
Incorporate one or more of the following outcome measurements when assessing and monitoring patient progress:
- Self-Rated Recovery Question
- Patient Specific Functional Scale
- Brief Pain Inventory (BPI)
- Visual Analog Scale (VAS)
- DASH Outcome Measure
- CTS-6 Evaluation Tool
- Kamath and Stothard Questionnaire
- Katz and Stirrat hand symptom diagram
- Upper Extremity Functional Index
- Brigham and Women’s Carpal Tunnel Questionnaire
- Boston Carpal Tunnel Questionnaire (BCTQ)
- Patient-Rated Wrist Evaluation (PRWE)
- Patient-Rated Wrist/Hand Evaluation (PRWHE)
Physical Examination
Incorporate one or more of the following physical examination tools to determine the likelihood of carpal tunnel syndrome and interpret examination results in the context of all clinical exam findings.
- Spurling’s Test (Foraminal Compression Test)
- Cervical Distraction Test
- Cervical Compression Test
- Scalene Cramp Test
- Adson’s Test
- Halstead Maneuver (Reverse Adson’s Test or Wright’s Test or Hyperabduction Test)
- Costoclavicular Test (Military Brace)
- Upper Limb Tension Tests (1, 2, 3, & 4)
- Phalen Test
- Tinel Sign
- Carpal Compression Test
Treatment
Education
Provide reassurance and patient education on condition and management options and encourage the use of active approaches (lifestyle, physical activity) to help manage symptoms.
Manual Therapy
The responses to massage therapy are complex and multifactorial – physiological and psychological factors interplay in a complex manner. Systematic reviews have also shown that manual therapy combined with multimodal care can improve symptoms, decrease disability, and improve function for patients who suffer from carpal tunnel syndrome (Huisstede et al., 2018). Research has looked at both peripheral and central responses elicited by massage therapy treatments, by working within the patients’ pain tolerance, massage therapy may help modulate nociceptive barrage into the central nervous system (peripheral drive) and activate endogenous pain networks (central drive).
Central Drive
Massage has a modulatory effect on peripheral and central processes via input from large sensory neurons that prevents the spinal cord from amplifying the nociceptive signal. This anti-nociceptive effect of massage therapy can help ease discomfort in patients who suffer from carpal tunnel syndrome.
Peripheral Drive
Carpal tunnel specific work may also involve specific soft tissue treatment to optimize the ability of mechanical interfaces to glide relative to the median nerve. The application of appropriate shear force and pressure impart a mechanical stimulus that may attenuate tissue levels of fibrosis and TGF-β1 (Bove et al., 2016; Bove et al., 2019). Furthermore, passive stretching may help diminish intraneural edema and/or pressure by mobilizing the median nerve as well as associated vascular structures (Boudier-Revéret et al., 2017).
Myofascial trigger point: Infraspinatus
The etiology of myofascial trigger points is still not well understood, but that does not deny the existence of the clinical phenomenon. From a clinical perspective, myofascial trigger points describe an observable phenomenon that may help clinicians investigate common pain patterns. An international panel of 60 clinicians and researchers was recently consulted to establish a consensus for identification of a myofascial trigger point. The panel agreed on two palpatory and one symptom criteria: a taut band, a hypersensitive spot, and referred pain (Fernández-de-Las-Peñas & Dommerholt, 2018). For patients with carpal tunnel syndrome studies have demonstrated that assessing and treating the infraspinatus muscle may be an effective treatment option for a sub-group of patients (Meder et al., 2017).
Structures to be Aware of When Treating Carpal Tunnel Syndrome
A massage therapy treatment plan should be implemented based on patient-specific assessment findings and patient tolerance. Structures to keep in mind while assessing and treating patients suffering from carpal tunnel syndrome may include neurovascular structures and investing fascia of:
- Costo-Clavicle Space
- Scalene Muscle Group (anterior scalene, middle scalene, and posterior scalene)
- Pectoral Region (pectoralis major, pectoralis minor, serratus anterior and subclavius)
- Rotator Cuff (subscapularis, infraspinatus, teres minor, supraspinatus)
- The Upper Arm (biceps brachii, brachialis, coracobrachialis, triceps brachii)
- Superficial Anterior Compartment of the Forearm (pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, flexor carpi ulnaris)
- Deep Anterior Compartment of the Forearm (flexor digitorum profundus, flexor pollicis longus, and pronator quadratus)
- Anterior Interosseous Membrane
- Carpal Bones (trapezium, trapezoid, capitate, hamate, scaphoid, lunate, triquetrum, pisiform)
- Palmar Aponeurosis & Transverse Carpal Ligament
- Lumbricals
Self-Management Strategies
Massage therapists not only provide hands-on treatment they can also develop self-management programs to help patients manage symptoms. Simple home-care recommendations such as stretching, splinting and home exercises have been shown to be useful for carpal tunnel syndrome (Lewis et al., 2020; Shem et al., 2020).
Prognosis
Massage therapy as a therapeutic intervention is being embraced by the medical community, it is simple to carry out, economical, and has very few side effects. Randomized clinical trials have demonstrated that for some patients who suffer from carpal tunnel syndrome there is no significant differences in pain and functional outcomes at a six month, twelve month, and four year follow up when surgical and conservative care are tested (Fernández-de-Las Peñas et al., 2017; Fernández-de-Las-Peñas et al., 2019; Fernández-de-Las-Peñas et al., 2020).
Massage Sloth: Massage Tutorial: Carpal Tunnel Syndrome
Contemporary multimodal massage therapists are uniquely suited to incorporate several rehabilitation strategies for carpal tunnel syndrome based on patient-specific assessment findings including, but not limited to:
- Manual Therapy (soft tissue massage, neural mobilization, joint mobilization)
- Education that is Person-Centered (e.g., biopsychosocial model of health and disease, self-efficacy beliefs, active coping strategies)
- Stretching & Loading Programs (e.g., concentric, eccentric, isometric exercises)
- Hydrotherapy (hot & cold)
- Self-Management Strategies (e.g., engaging in physical activity and exercise, social activities, and healthy sleep habits)
References and Sources
Barbe, M. F., Hilliard, B. A., Fisher, P. W., White, A. R., Delany, S. P., Iannarone, V. J., Harris, M. Y., Amin, M., Cruz, G. E., & Popoff, S. N. (2020). Blocking substance P signaling reduces musculotendinous and dermal fibrosis and sensorimotor declines in a rat model of overuse injury. Connective tissue research, 61(6), 604–619. https://doi.org/10.1080/03008207.2019.1653289
Barbe, M. F., Hilliard, B. A., Amin, M., Harris, M. Y., Hobson, L. J., Cruz, G. E., … Popoff, S. N. (2020). Blocking CTGF/CCN2 reverses neural fibrosis and sensorimotor declines in a rat model of overuse-induced median mononeuropathy. Journal of orthopaedic research: official publication of the Orthopaedic Research Society, 10.1002/jor.24709. Advance online publication. https://doi.org/10.1002/jor.24709
Boudier-Revéret, M., Gilbert, K. K., Allégue, D. R., Moussadyk, M., Brismée, J. M., Sizer, P. S., Jr, … Sobczak, S. (2017). Effect of neurodynamic mobilization on fluid dispersion in median nerve at the level of the carpal tunnel: A cadaveric study. Musculoskeletal science & practice, 31, 45–51. doi:10.1016/j.msksp.2017.07.004
Bove, G. M., Harris, M. Y., Zhao, H., & Barbe, M. F. (2016). Manual therapy as an effective treatment for fibrosis in a rat model of upper extremity overuse injury. Journal of the neurological sciences, 361, 168–180. doi:10.1016/j.jns.2015.12.029
Bove, G. M., Delany, S. P., Hobson, L., Cruz, G. E., Harris, M. Y., Amin, M., … Barbe, M. F. (2019). Manual therapy prevents onset of nociceptor activity, sensorimotor dysfunction, and neural fibrosis induced by a volitional repetitive task. Pain, 160(3), 632–644. doi:10.1097/j.pain.0000000000001443
Bueno-Gracia, E., Ruiz-de-Escudero-Zapico, A., Malo-Urriés, M., Shacklock, M., Estébanez-de-Miguel, E., Fanlo-Mazas, P., … Jiménez-Del-Barrio, S. (2018). Dimensional changes of the carpal tunnel and the median nerve during manual mobilization of the carpal bones. Musculoskeletal science & practice, 36, 12–16. doi:10.1016/j.msksp.2018.04.002
Dabbagh, A., MacDermid, J. C., Yong, J., Macedo, L. G., & Packham, T. L. (2020). Diagnosing Carpal Tunnel Syndrome: Diagnostic Test Accuracy of Scales, Questionnaires, and Hand Symptom Diagrams-A Systematic Review. The Journal of orthopaedic and sports physical therapy, 50(11), 622–631. https://doi.org/10.2519/jospt.2020.9599
Donnelly, C. R., Chen, O., & Ji, R. R. (2020). How Do Sensory Neurons Sense Danger Signals?. Trends in neurosciences, 43(10), 822–838. https://doi.org/10.1016/j.tins.2020.07.008
Erickson, M., Lawrence, M., Jansen, C., Coker, D., Amadio, P., & Cleary, C. (2019). Hand Pain and Sensory Deficits: Carpal Tunnel Syndrome. The Journal of orthopaedic and sports physical therapy, 49(5), CPG1–CPG85. doi:10.2519/jospt.2019.0301
Fernández-de-Las Peñas, C., Ortega-Santiago, R., de la Llave-Rincón, A. I., Martínez-Perez, A., Fahandezh-Saddi Díaz, H., Martínez-Martín, J., Pareja, J. A., & Cuadrado-Pérez, M. L. (2015). Manual Physical Therapy Versus Surgery for Carpal Tunnel Syndrome: A Randomized Parallel-Group Trial. The journal of pain: official journal of the American Pain Society, 16(11), 1087–1094.https://doi.org/10.1016/j.jpain.2015.07.012
Fernández-de-Las-Peñas, C., Cleland, J., Palacios-Ceña, M., Fuensalida-Novo, S., Pareja, J. A., & Alonso-Blanco, C. (2017). The Effectiveness of Manual Therapy Versus Surgery on Self-reported Function, Cervical Range of Motion, and Pinch Grip Force in Carpal Tunnel Syndrome: A Randomized Clinical Trial. The Journal of orthopaedic and sports physical therapy, 47(3), 151–161. doi:10.2519/jospt.2017.7090
Fernández-de-Las-Peñas, C., & Dommerholt, J. (2018). International Consensus on Diagnostic Criteria and Clinical Considerations of Myofascial Trigger Points: A Delphi Study. Pain medicine (Malden, Mass.), 19(1), 142–150. doi:10.1093/pm/pnx207
Fernández-de-Las-Peñas, C., Ortega-Santiago, R., Díaz, H. F., Salom-Moreno, J., Cleland, J. A., Pareja, J. A., & Arias-Buría, J. L. (2019). Cost-Effectiveness Evaluation of Manual Physical Therapy Versus Surgery for Carpal Tunnel Syndrome: Evidence From a Randomized Clinical Trial. The Journal of orthopaedic and sports physical therapy, 49(2), 55–63. doi:10.2519/jospt.2019.8483
Fernández-de-Las-Peñas, C., Arias-Buría, J. L., Ortega-Santiago, R., & De-la-Llave-Rincón, A. I. (2020). Understanding central sensitization for advances in management of carpal tunnel syndrome. F1000Research, 9, F1000 Faculty Rev-605. https://doi.org/10.12688/f1000research.22570.1
Fernández-de-Las-Peñas, C., Arias-Buría, J. L., Cleland, J. A., Pareja, J. A., Plaza-Manzano, G., & Ortega-Santiago, R. (2020). Manual Therapy Versus Surgery for Carpal Tunnel Syndrome: 4-Year Follow-Up From a Randomized Controlled Trial. Physical therapy, 100(11), 1987–1996. https://doi.org/10.1093/ptj/pzaa150
Hamzeh, H., Madi, M., Alghwiri, A. A., & Hawamdeh, Z. (2020). The long-term effect of neurodynamics vs exercise therapy on pain and function in people with carpal tunnel syndrome: A randomized parallel-group clinical trial. Journal of hand therapy: official journal of the American Society of Hand Therapists, S0894-1130(20)30144-7. Advance online publication. https://doi.org/10.1016/j.jht.2020.07.005
Huisstede, B. M., van den Brink, J., Randsdorp, M. S., Geelen, S. J., & Koes, B. W. (2018). Effectiveness of Surgical and Postsurgical Interventions for Carpal Tunnel Syndrome-A Systematic Review. Archives of physical medicine and rehabilitation, 99(8), 1660–1680.e21. doi:10.1016/j.apmr.2017.04.024
Huisstede, B. M., Hoogvliet, P., Franke, T. P., Randsdorp, M. S., & Koes, B. W. (2018). Carpal Tunnel Syndrome: Effectiveness of Physical Therapy and Electrophysical Modalities. An Updated Systematic Review of Randomized Controlled Trials. Archives of physical medicine and rehabilitation, 99(8), 1623–1634.e23. doi:10.1016/j.apmr.2017.08.482
Jesson, T., Runge, N., & Schmid, A. B. (2020). Physiotherapy for people with painful peripheral neuropathies: a narrative review of its efficacy and safety. PAIN Reports, 5(5), 1-e834
Lewis, K. J., Coppieters, M. W., Ross, L., Hughes, I., Vicenzino, B., & Schmid, A. B. (2020). Group education, night splinting and home exercises reduce conversion to surgery for carpal tunnel syndrome: a multicentre randomised trial. Journal of physiotherapy, 66(2), 97–104. https://doi.org/10.1016/j.jphys.2020.03.007
Maeda, Y., Kim, H., Kettner, N., Kim, J., Cina, S., Malatesta, C., … Napadow, V. (2017). Rewiring the primary somatosensory cortex in carpal tunnel syndrome with acupuncture. Brain: a journal of neurology, 140(4), 914–927. doi:10.1093/brain/awx015
Meder, M. A., Amtage, F., Lange, R., & Rijntjes, M. (2017). Reliability of the Infraspinatus Test in Carpal Tunnel Syndrome: A Clinical Study. Journal of clinical and diagnostic research: JCDR, 11(5), YC01–YC04. doi:10.7860/JCDR/2017/25096.9831
Piper, S., Shearer, H. M., Côté, P., Wong, J. J., Yu, H., Varatharajan, S., … Taylor-Vaisey, A. L. (2016). The effectiveness of soft-tissue therapy for the management of musculoskeletal disorders and injuries of the upper and lower extremities: A systematic review by the Ontario Protocol for Traffic Injury management (OPTIMa) collaboration. Manual therapy, 21, 18–34. https://doi.org/10.1016/j.math.2015.08.011.
Saunders, R., Astifidis, R., Burke, S., Higgins, J., McClinton, M., (2015). Hand and Upper Extremity Rehabilitation: A Practical Guide (4th ed.). Elsevier
Schmid, A. B., Fundaun, J., & Tampin, B. (2020). Entrapment neuropathies: a contemporary approach to pathophysiology, clinical assessment, and management. Pain reports, 5(4), e829.https://doi.org/10.1097/PR9.0000000000000829
Shem, K., Wong, J., & Dirlikov, B. (2020). Effective self-stretching of carpal ligament for the treatment of carpal tunnel syndrome: A double-blinded randomized controlled study. Journal of hand therapy: official journal of the American Society of Hand Therapists, 33(3), 272–280. https://doi.org/10.1016/j.jht.2019.12.002
Shi, Q., Bobos, P., Lalone, E. A., Warren, L., & MacDermid, J. C. (2020). Comparison of the Short-Term and Long-Term Effects of Surgery and Nonsurgical Intervention in Treating Carpal Tunnel Syndrome: A Systematic Review and Meta-Analysis. Hand (New York, N.Y.), 15(1), 13–22. https://doi.org/10.1177/1558944718787892
Skirven, T., Osterman, A. L., Fedorczyk, J., Amadio, P., Felder, S., Shin, E. (2021). Rehabilitation of the Hand and Upper Extremity (7th ed.). Elsevier
Spicher, C. (2020). Atlas of Cutaneous Branch Territories for the Diagnosis of Neuropathic Pain. Springer.
Stecco, C., Giordani, F., Fan, C., Biz, C., Pirri, C., Frigo, A. C., … De Caro, R. (2020). Role of fasciae around the median nerve in pathogenesis of carpal tunnel syndrome: microscopic and ultrasound study. Journal of anatomy, 236(4), 660–667. https://doi.org/10.1111/joa.13124
Wolny, T., & Linek, P. (2019). Is manual therapy based on neurodynamic techniques effective in the treatment of carpal tunnel syndrome? A randomized controlled trial. Clinical rehabilitation, 33(3), 408–417. doi:10.1177/0269215518805213