
29.18A: Ectopic Pregnancy
- Page ID
- 8393
An ectopic pregnancy is implantation and development of the embryo outside the uterus, typically in the fallopian tubes.
- Identify the factors involved in ectopic pregnancies
Key Points
- An ectopic pregnancy, or eccysis, is a complication of pregnancy in which the embryo implants outside the uterine cavity. With rare exceptions, ectopic pregnancies are not viable. Furthermore, they are dangerous for the mother, since internal haemorrhage is a life threatening complication.
- Most ectopic pregnancies occur in the Fallopian tube (called tubal pregnancies), but implantation can also occur in the cervix, ovaries, and abdomen. An ectopic pregnancy is a potential medical emergency, and, if not treated properly, can lead to death.
- If left untreated, about half of ectopic pregnancies will resolve without treatment and are called tubal abortions.
- A heterotopic pregnancy occurs when there are two fertilized eggs, one outside the uterus and the other inside.
- The mortality rate from ectopic pregnancies in Western countries is very low (less than one percent), but in underdeveloped countries, especially in Africa, the maternal death rate is extremely high and are a major cause of death among women of childbearing age.
Key Terms
- heterotopic pregnancy: A heterotopic pregnancy is a rare complication of pregnancy in which both extra-uterine (ectopic pregnancy) and intrauterine gestation occur simultaneously.
- ectopic pregnancy: A pregnancy in which the fertilized ovum is implanted in any tissue other than the uterine wall.
An ectopic pregnancy, or eccysis, is a complication of pregnancy in which the embryo implants outside the uterine cavity. With rare exceptions, ectopic pregnancies are not viable. Furthermore, they are dangerous for the mother, since internal haemorrhage is a life threatening complication that may result. Most ectopic pregnancies occur in the Fallopian tube (so-called tubal pregnancies), but implantation can also occur in the cervix, ovaries, and abdomen. An ectopic pregnancy is a potential medical emergency, and, if not treated properly, can lead to death.
In a normal pregnancy, the fertilized egg enters the uterus and settles into the uterine lining where it has plenty of room to divide and grow. About 1% of pregnancies are in an ectopic location with implantation not occurring inside of the womb; of these pregnancies, 98% occur in the Fallopian tubes.
Detection
Detection of ectopic pregnancy in early gestation has been achieved mainly due to enhanced diagnostic capability. Despite all these notable successes in diagnostics and detection techniques ectopic pregnancy remains a source of serious maternal morbidity and mortality worldwide, especially in countries with poor prenatal care.
Treatment
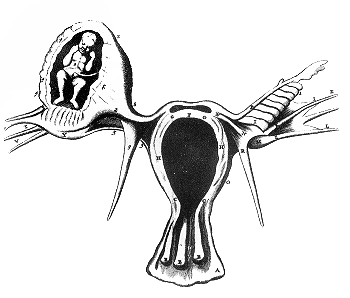
Ectopic pregnancy: schematic view of ectopic pregnancy
In a typical ectopic pregnancy, the embryo adheres to the lining of the fallopian tube and burrows into the tubal lining. Most commonly, this invades vessels and will cause bleeding. This intratubal bleeding hematosalpinx expels the implantation out of the tubal end as a tubal abortion. Tubal abortion is a common type of miscarriage. There is no inflammation of the tube in ectopic pregnancy. The pain is caused by prostaglandins released at the implantation site, and by free blood in the peritoneal cavity, which is a local irritant. Sometimes the bleeding might be heavy enough to threaten the health or life of the woman. Usually, this degree of bleeding is due to delay in diagnosis, but sometimes, especially if the implantation is in the proximal tube (just before it enters the uterus), it may invade into the nearby Sampson artery, causing heavy bleeding earlier than usual.
If left untreated, about half of ectopic pregnancies will resolve without treatment. These are the tubal abortions. The advent of methotrexate treatment for ectopic pregnancy has reduced the need for surgery; however, surgical intervention is still required in cases where the Fallopian tube has ruptured or is in danger of doing so. This intervention may be laparoscopic or through a larger incision, known as a laparotomy.
While a fetus of ectopic pregnancy is typically not viable, very rarely, a live baby has been delivered from an abdominal pregnancy. In such a situation the placenta sits on the intraabdominal organs or the peritoneum and has found sufficient blood supply. This is generally bowel or mesentery, but other sites, such as the renal (kidney), liver or hepatic (liver) artery or even aorta have been described.
In rare cases of ectopic pregnancy, there may be two fertilized eggs, one outside the uterus and the other inside. This is called a heterotopic pregnancy. Often the intrauterine pregnancy is discovered later than the ectopic, mainly because of the painful emergency nature of ectopic pregnancies. Since ectopic pregnancies are normally discovered and removed very early in the pregnancy, an ultrasound may not find the additional pregnancy inside the uterus. When hCG levels continue to rise after the removal of the ectopic pregnancy, there is the chance that a pregnancy inside the uterus is still viable. This is normally discovered through an ultrasound.
Risk Factors
There are a number of risk factors for ectopic pregnancies. However, in as many as one third to one half of ectopic pregnancies, no risk factors can be identified. Risk factors include: pelvic inflammatory disease, infertility, use of an intrauterine device (IUD), previous exposure to DES, tubal surgery, intrauterine surgery (e.g., D&C), smoking, previous ectopic pregnancy, and tubal ligation.
Prognosis
The prognosis in Western countries is very good; maternal death is rare. For instance, in the UK, between 2003 and 2005 there were 32,100 ectopic pregnancies resulting in 10 maternal deaths (meaning that 1 in 3,210 women with an ectopic pregnancy died). In the developing world, however, especially in Africa, the death rate is very high, and ectopic pregnancies are a major cause of death among women of childbearing age.
Fertility following ectopic pregnancy depends upon several factors, the most important of which is a prior history of infertility. The treatment choice, whether surgical or nonsurgical, also plays a role. For example, the rate of intrauterine pregnancy may be higher following methotrexate compared to surgical treatment. Rate of fertility may be better following salpingostomy than salpingectomy.