
1.18: Supracricoid - Laryngectomy
- Page ID
- 17629

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
SUPRACRICOID LARYNGECTOMY
Alejandro Castro, Javier Gavilán
Supracricoid laryngectomy consists of en bloc resection of both vocal cords, the paraglottic spaces and the thyroid cartilage (Figure 1). It was first described by Majer in 19591 and Piquet in 19742. It is used for the treatment of selected early and locally advanced glottic and transglottic carcinoma in an oncologically safe manner, while preserving laryngeal function i.e. swallowing (airway protection), breathing and phonation.
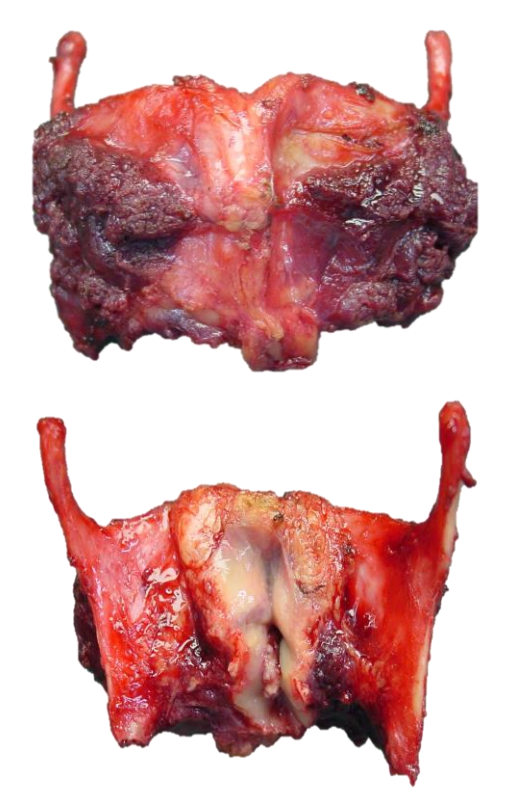
Figure 1: Typical supracricoid laryngectomy specimen
Indications and limitations
Supracricoid laryngectomy is used to treat glottic carcinoma affecting one/both vocal cords, including cancers with deep invasion of the paraglottic space and altered vocal cord mobility. The epiglottis and pre-epiglottic space can be included in the specimen, allowing for resection of transglottic tumors that invade the supraglottic and glottic regions. One arytenoid can also be resected. However combined resection of the epiglottis and one arytenoid usually results in poor functional outcomes and increases the chance for aspiration and delayed decannulation.
Types of supracricoid operations
With supracricoid laryngectomy the hyoid bone is approximated directly to the cricoid with three sutures (Figures 2a-c). Types of supracricoid laryngectomy are illustrated below i.e. cricohyoidoepiglottopexy (CHEP), cricohyoidopexy (CHP), and tracheocricohyoidoepiglottopexy (Figures 2a-c). With tracheocricohyoidoepiglottopexy the anterior cricoid is resected for an additional tumor margin anteriorly.
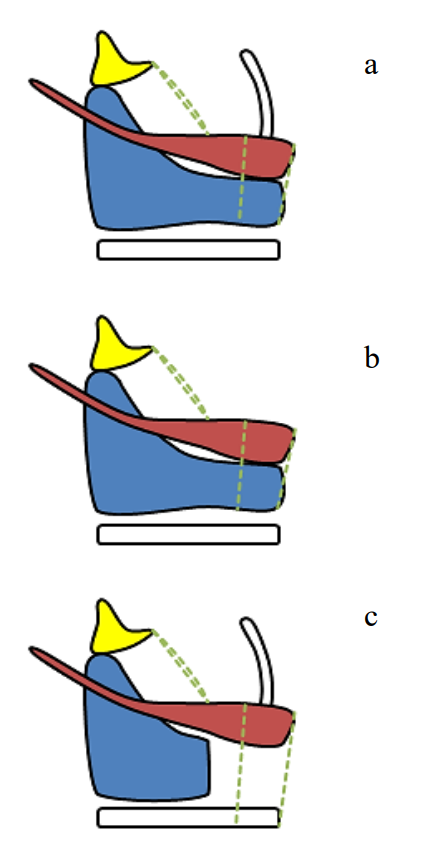
Figure 2: Cricohyoidoepiglottopexy (a), cricohyoidopexy (b), and tracheocricohyoidoepiglottopexy (c)
Function
Key functional outcomes are airway, phonation and swallowing without aspiration. Phonation and swallowing depend on the arytenoids being able to tilt forwards and make contact with the base of the tongue; to breathe the arytenoids tilt posteriorly to open the airway (Figures 3, 4).
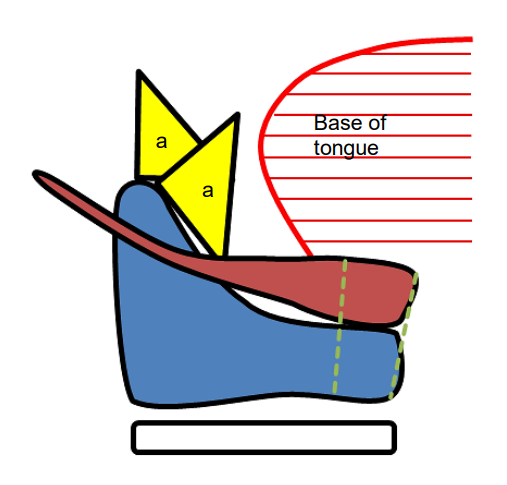
Figure 3: Arytenoids tilt forwards and backwards for phonation, swallowing and breathing
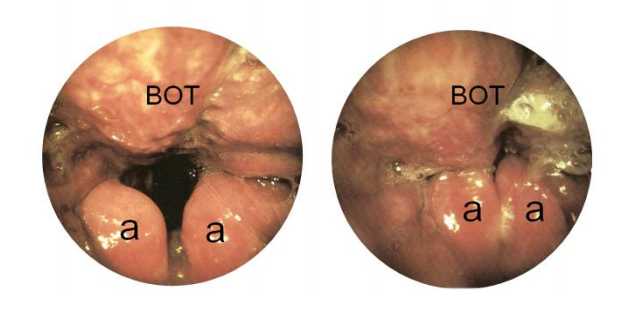
Figure 4: Arytenoids tilt backwards and forwards for breathing, phonation, swallowing
Cricoarytenoid unit(Figures 5, 6)
An intact cricoarytenoid unit is critical for function. It comprises the arytenoid mounted on an intact posterior cricoid ring, with a functioning recurrent laryngeal nerve and lateral and posterior cricoarytenoid muscles. Ideally one should preserve both cricoarytenoid units; sacrificing one unit increases the chance of disabling aspiration in the cases where the epiglottis is resected.
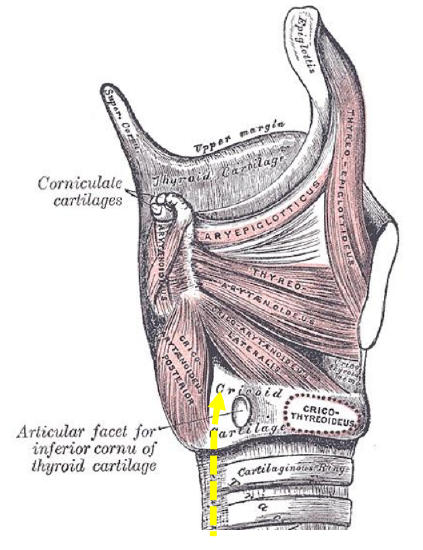
Figure 5: Anatomy of the cricoarytenoid unit and the course of the recurrent laryngeal nerve (yellow arrow) directly behind the articular facet of the inferior cornu of the thyroid cartilage
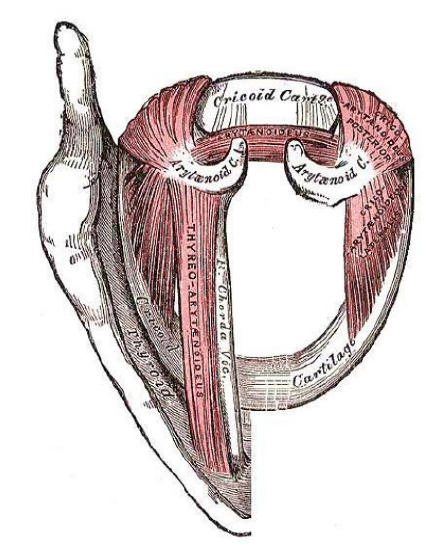
Figure 6: Right side illustrates the situation after supracricoid laryngectomy with preserved cricoarytenoid unit
Preoperative Evaluation
Careful selection of candidates is the key to success of supracricoid laryngectomy. Both tumor and patient factors must be taken into account to ensure satisfactory oncologic and functional outcomes.
1. Tumor factors
TNM classifications were not developed to guide the indications for different surgical techniques; other factors should be taken into account when considering supracricoid laryngectomy. In general, supracricoid laryngectomy is indicated for T1 and selected T2-3 glottic as well as selected T2-4a supraglottic cancers. Nevertheless supracricoid laryngectomy is usually appropriate, for example, for virtually any T2 glottic cancer but it is contraindicated for those rare T2 glottic cancers with extensive subglottic extension.
Two types of vocal cord immobility should be taken into account when considering supracricoid laryngectomy
- Tumors that invade the paraglottic space and “fix” the vocal cord, but with some preserved mobility of the arytenoid: These tumors can usually be resected by supracricoid laryngectomy as resection of the arytenoid is likely to produce a negative margin
- Cricoarytenoid joint invasion: This must be suspected when the arytenoid is “frozen”. Supracricoid laryngectomy is not recommended as even resecting the arytenoid is unlikely to yield a negative margin
The extent of the tumor relative to the resection limits of supracricoid laryngectomy must be considered
- Inferiorly: Superior border of cricoid cartilage: Routine intraoperative frozen section is strongly recommended to ensure negative mucosal margins at the superior border of the cricoid cartilage. Some authors describe partial or complete resection of the anterior cricoid arch3, 4. Although this might be oncologically safe, in our hands it compromises the functional results and should be performed only in very carefully selected cases (Figure 2c)
- Superiorly: Epiglottis or tongue base, depending on the upper extent of the tumor: The epiglottis and pre-epiglottic space can be included in the resection (Figure 2b). Although limited extension to the base of the tongue can be excised, resection should not extend beyond the circumvallate papillae as the base of the tongue plays a critical role with laryngeal closure during swallowing (Figures 3, 4)
- Laterally: Pyriform sinus: Limited resection of the medial wall of the pyriform sinus can be accomplished. However, wide resection which includes the lateral wall may compromise swallowing
- Posteriorly (midline): The interarytenoid space must be free of tumor: It is strongly recommended to preserve both arytenoids when the epiglottis is included in the resection. At least one mobile arytenoid must always be preserved
- Thyroid cartilage: As the paraglottic spaces and thyroid cartilage are resected en bloc, involvement of only the inner perichondrium is not a contraindication However, more extensive invasion of the thyroid cartilage is a contraindication to supracricoid laryngectomy. Yet cancers of the anterior commissure invading thyroid cartilage in the midline may be considered for supracricoid laryngectomy.
Careful preoperative evaluation should be undertaken to ensure that the primary tumor falls within these above mentioned limits. As a rule, indirect (fiberoptic) and/ or direct laryngoscopy are adequate for this purpose. CT scan or other imaging techniques may help in some cases, particularly to determine extralaryngeal extension through thyroid cartilage.
Extending the resection beyond the above mentioned parameters reduces the chance of functional success (aspiration and/or inability to be decannulated) and should be performed only in very carefully selected patients. Employing supracricoid laryngectomy with too advanced tumors or relying on postoperative radiotherapy to treat positive margins is unacceptable as it increases recurrence rates and reduces survival.
Frozen section should always be used with any type of open partial laryngectomy. With supracricoid laryngectomy, it should be obtained to confirm oncologic safety of every close margin, and routinely at the level of the cricoid. Patients should agree preoperatively that total laryngectomy will be performed if negative margins cannot be obtained.
Neck dissection can be performed simultaneously. T1-2 glottic cancer without evidence of neck metastases can be treated with supracricoid laryngectomy without neck dissection. Elective ipsilateral neck dissection is advocated for locally advanced, purely glottic tumors (vocal cord fixation). Bilateral neck dissection is recommended in all patients with tumor invading the supraglottis regardless of T and N stage.
2. Patient factors
Patients need to learn new ways to swallow after removal of part of the larynx. Every patient undergoing supracricoid laryngectomy will experience aspiration of varying degrees during the initial postoperative days. Age is an important consideration as the brain’s plasticity decreases with age as does a patient’s ability to learn new swallowing techniques. Classically, 65-70 years is considered the cut-off for open partial laryngectomy. However, a patient’s general status is more important than age itself, and successful results have been reported in older patients5, 6.
Careful evaluation of comorbidities is important to ensure successful functional outcomes. The cough reflex is of critical importance to deal with aspiration. In our series, up to 15% of patients developed pneumonia7. Pulmonary and cardiac reserve is crucial to overcome this complication. Some authors recommend routine preoperative pulmonary function tests8, 9. We believe that a detailed clinical history is adequate, focusing attention on symptoms relating to chronic obstructive pulmonary disease e.g. dyspnoea when walking up a flight of stairs and types of medication.
Supracricoid laryngectomy operation
The operation is done under general anesthesia with the patient in a supine position. Antibiotics are given perioperatively.
1. Surgical approach
- A U-shaped cervical incision is made. The vertical limbs of the incision start a few centimetres above the hyoid bone and run along the anterior borders of the sternocleidomastoid muscles. The horizontal limb passes 2-3 cm above the sternal notch
- If neck dissection is planned, the Ushaped incision runs from mastoid-tomastoid close to the posterior border of the sternocleidomastoid muscle to create a broader flap. Neck dissections are done before the laryngectomy
- A superiorly based subplatysmal apron flap is elevated to expose the supraand infrahyoid muscles of the neck (Figures 7, 8)
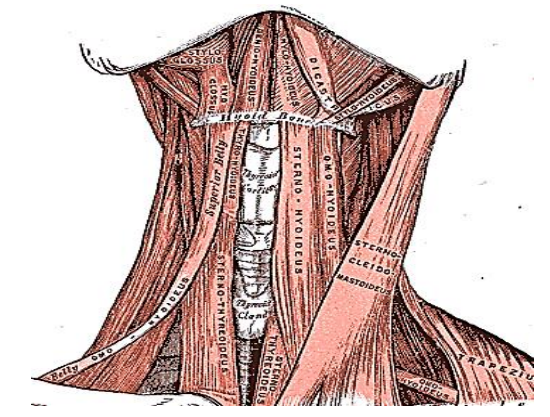
Figure 7: Infra- and suprahyoid muscles
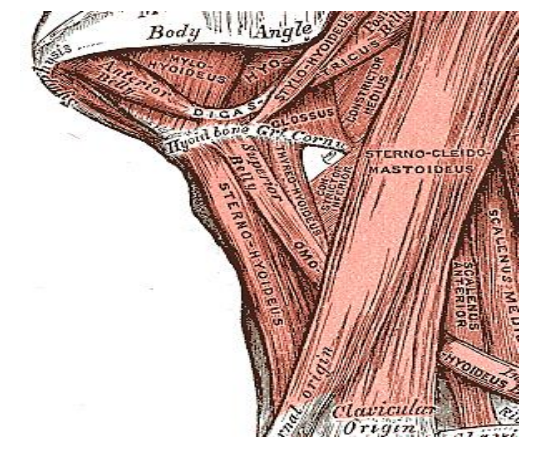
Figure 8: Infra- and suprahyoid muscles
- Detach the sternohyoid muscles from the hyoid bone and reflect them inferiorly to the level of the 1st tracheal ring (Figure 9)
- Retract the omohyoid muscles laterally (Figure 10)
- Detach the thyrohyoid muscles from the hyoid and reflected them inferiorly to their insertions on the thyroid cartilage (Figure 10)
- Section the sternothyroid muscles at the inferior border of the thyroid cartilage (Figure 11)
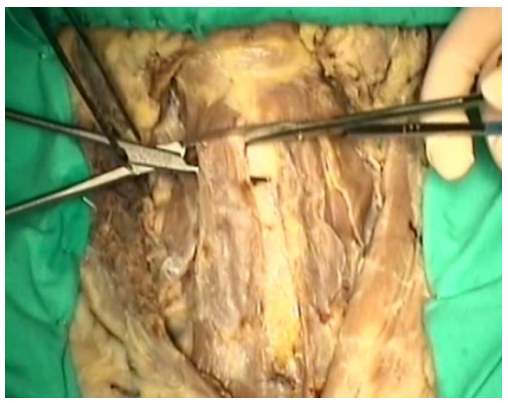
Figure 9: Divide sternohyoid muscle

Figure 10: Retract omohyoid and divide thyrohyoid muscle
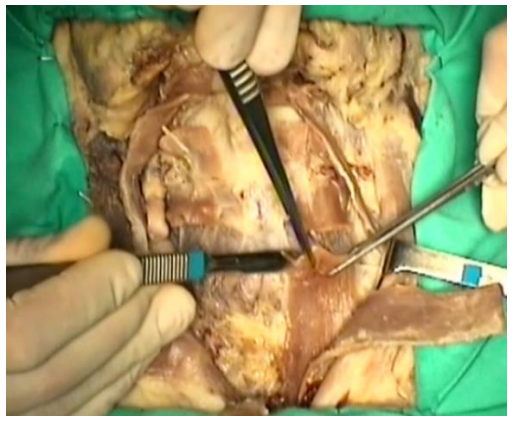
Figure 11: Divide sternothyroid muscle
- Exposed, ligate and divide the isthmus of the thyroid gland
- Dissect both thyroid lobes off the larynx and trachea to expose the thyroid and cricoid cartilages, as well as the first tracheal rings (Figure 12)
- Stop the dissection posteriorly at the level of the inferior cornu of the thyroid cartilage to avoid injuring the recurrent laryngeal nerves (Figure 5)
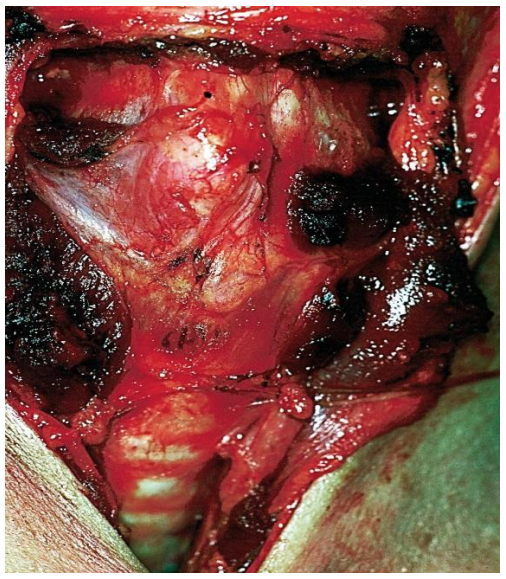
Figure 12: Surgical view of exposed larynx with strap muscles reflected. Thyroid lobes have been dissected and retracted laterally exposing the larynx and the first tracheal rings. Note that the anterior wall of the trachea has been dissected to facilitate cricohyoidopexy at the end of the surgery
- Identify, ligate and divide the superior laryngeal artery and vein over the thyrohyoid membrane (Figure 13)
- One may preserve the internal branch of the superior laryngeal nerve when the epiglottis and pre-epiglottic space are preserved (Some authors report better swallowing when supraglottic sensation is preserved, but in our opinion preservation of the internal branch of the superior laryngeal nerve does not improve swallowing)

Figure 13: Divide superior laryngeal vessels
- Rotate the larynx with a hook placed at the posterior border of the thyroid cartilage (Figure 14)
- Identify and divide the lateral thyrohyoid ligament (Figure 14)

Figure 14: (Right side) Rotate the larynx with a hook placed at the posterior border of the thyroid cartilage and divide the lateral thyrohyoid ligament at its insertion on the superior cornu of the thyroid cartilage
- Divide the inferior constrictor muscle along the posterior border of the thyroid cartilage (Figures 15a, b)
- When reaching the inferior cornu, direct this cut obliquely in an anteroinferior direction to follow the anterior border of the cornu in order to protect the recurrent laryngeal nerve which lies close to the posterior aspect of the inferior cornu (Figure 15a)
- Expose the pyriform sinus submucosa after cutting the inferior constrictor muscle and dissect it from the inner perichondrium of the thyroid lamina (Figure 15b)
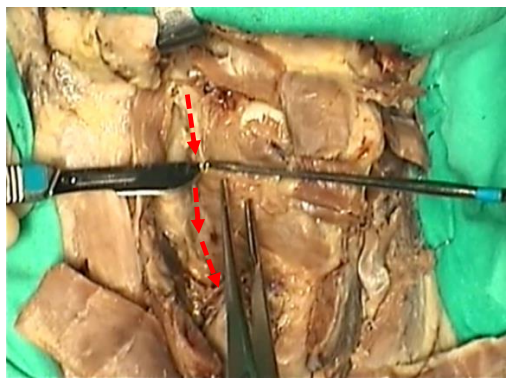
Figure 15a: Divide the inferior constrictor muscle. Traction on the muscle is generated by rotating the larynx with a hook placed at the posterior border of the thyroid cartilage. The dotted red line marks the course of the cut. Note that the cut turns anteriorly as it approaches the inferior cornu to protect the recurrent larynxgeal nerve
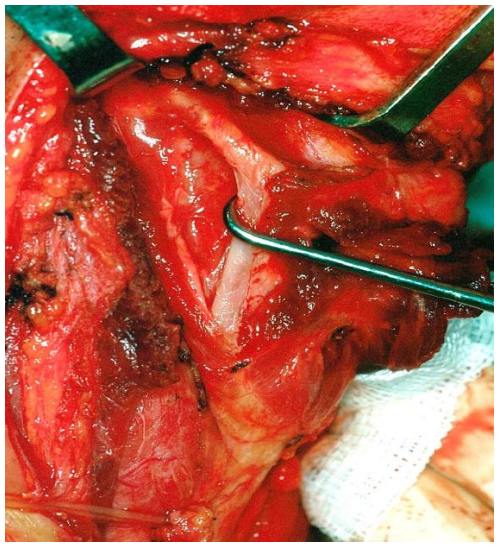
Figure 15b: The inferior constrictor muscle has been divided over the lateral border of the right thyroid ala exposing the submucosa of the pyriform sinus
- Place a submucosal stitch in the pyriform sinus without violating the mucosa, and leave it in place; this stitch is used later during reconstruction (Figures 16, 31)
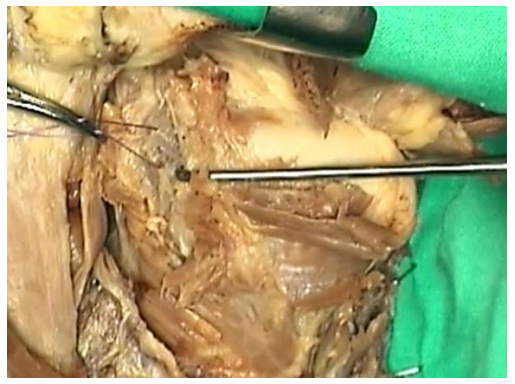
Figure 16: A suture is passed through the pyriform sinus submucosa
- Separate the thyroid and cricoid cartilages. The recurrent laryngeal nerve is close to the cricothyroid joint and may be injured at this point. We recommend transecting the inferior cornu of the thyroid cartilage at its base with scissors while the assistant steadies the thyroid and cricoid cartilages to avoid the blades slipping (Figure 17).
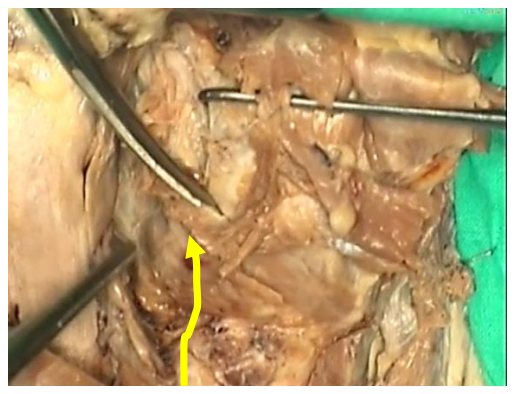
Figure 17: The larynx is rotated with a hook. The inferior cornu of the thyroid cartilage is divided with scissors taking the course of the recurrent laryngeal nerve (yellow line) into consideration
- Repeat the same surgical steps on opposite side either simultaneously or sequentially
- Free the thyroid cartilage from its attachments so that it can be easily displaced in any direction
2. Resecting the larynx
The supracricoid laryngectomy specimen is resected by means of two horizontal and two vertical cuts (Figure 18)
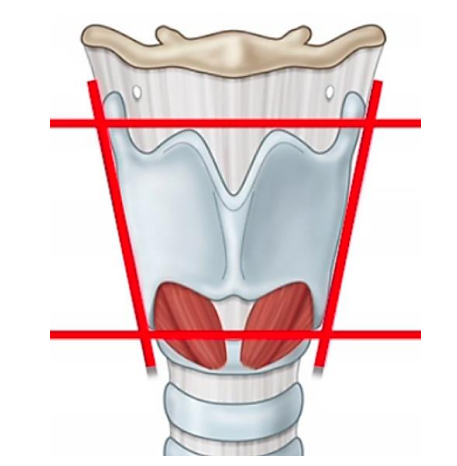
Figure 18: Horizontal and vertical cuts
Inferior horizontal cut
- Make a wide cricothyrotomy at the level of the superior border of the anterior cricoid arch, extending from one inferior thyroid cartilage cornu to the other (Figures 19 a)
- Retract the cricothyroid membrane and directly inspect the inner surface of the cricoid cartilage
- Obtain frozen sections of this margin
- Remove the orotracheal tube and insert a new tube through the cricothyrotomy; this facilitates the subsequent steps of the operation (Figures 19b)
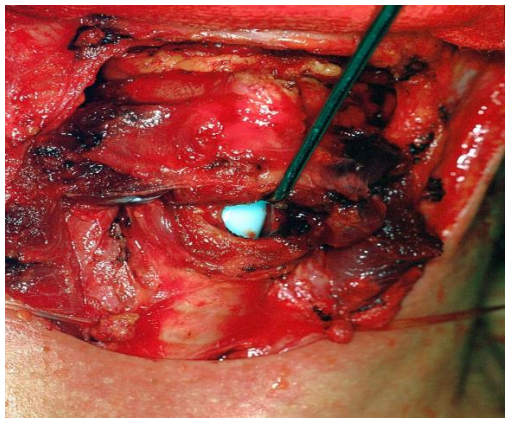
Figure 19a: Surgical view of the inferior horizontal cut. Note that the endotracheal tube is still in place
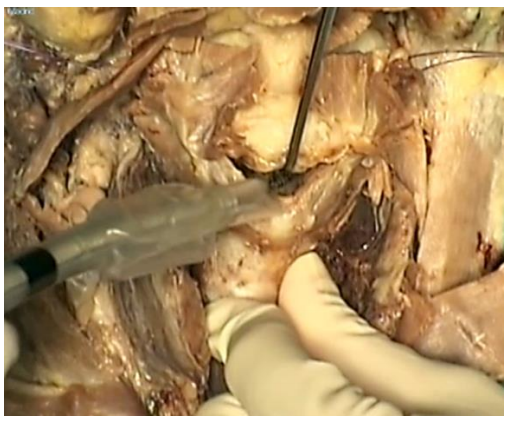
Figure 19b: Inferior horizontal cut (cricothyrotomy); the orotracheal tube is removed and a new tube is inserted through the cricothyrotomy
Superior horizontal cut
This can be made at two different levels, depending on the superior extension of the tumor
- Tumors not invading epiglottis (cricohyoidoepiglottopexy) (Fig 20a-e)
- Make the cut at the level of the superior border of the thyroid lamina through the thyrohyoid membrane and epiglottis
- Place a #11 scalpel in the midline, perpendicular to the larynx
- Stab the scalpel through the epiglottic cartilage into the pharyngeal lumen taking care not to injure the posterior pharyngeal wall
- Cut laterally first to one side, then the other to create a clean horizontal cut above the ventricular bands and the epiglottic petiole, which are included in the specimen (Figures 20a-e)
- Obtain frozen section at this margin if needed
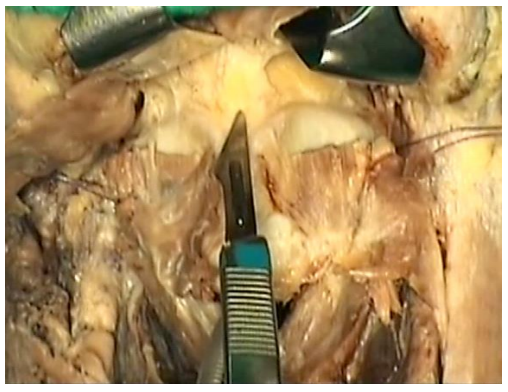
Figure 20a: Superior horizontal cut for epiglottis-preserving approach. Scalpel is inserted in the midline immediately above the superior border of the thyroid cartilage
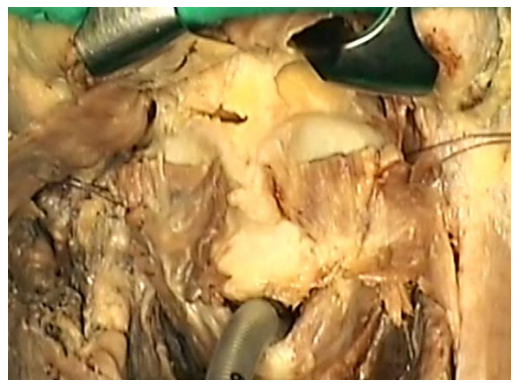
Figure 20b: A cut is been made to one side
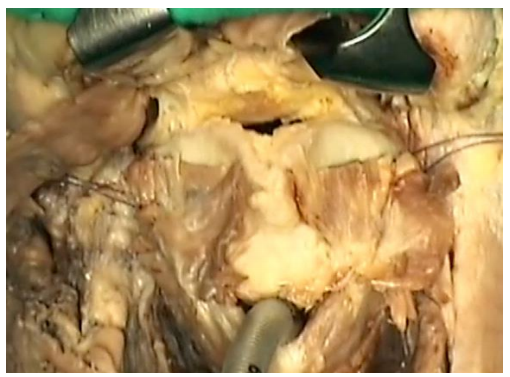
Figure 20c: The cut is completed on the contralateral side
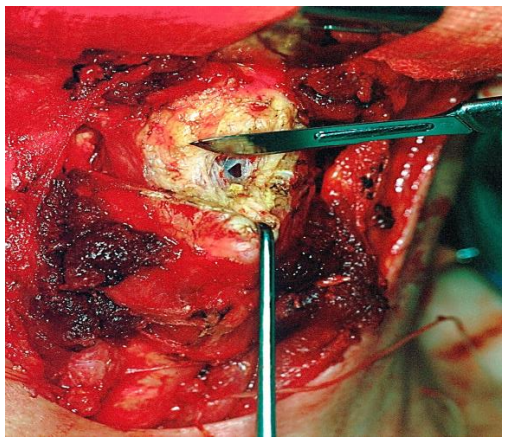
Figure 20d: Surgical view of the superior horizontal cut. The mucosa is opened in the midline before the cut is completed
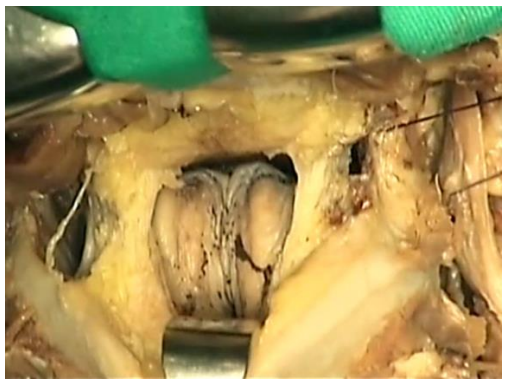
Figure 20e: Arytenoids visible through superior horizontal cut
- When the entire epiglottis and preepiglottic space need to be resected (cricohyoidopexy) (Figures 21a-c)
- Make a superior infrahyoid horizontal cut (not into the pharynx)
- Using sharp dissection with scissors, remove tissue from the preepiglottic space until the submucosa of the valleculae is reached
- Make an opening in the mucosa of the vallecula on one side, as far from tumor as possible
- Introduced a blade of the scissors inside the pharynx through the opening, with the other blade remaining outside
- Cut across both valleculae from side-to-side
- Introduce a finger into the pharynx through the mucosal opening to palpate the tumor, or directly inspect the tumor to assure a macroscopically free margin o Obtain frozen sections whenever the tumor approaches the resection margins
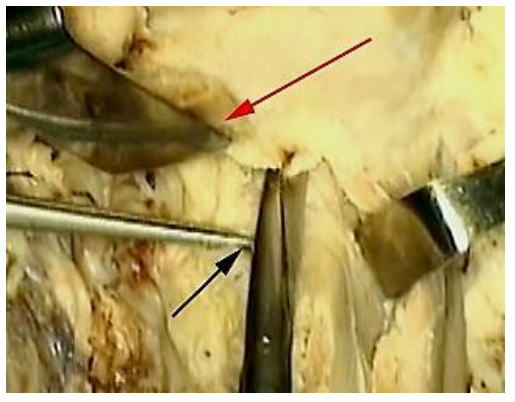
Figure 21a: Superior horizontal cut for a supracricoid laryngectomy with removal of epiglottis. The hyoid is retracted superiorly (red arrow) and traction with forceps (black arrow) is applied to the preepiglottic fat. The pre-epiglottic space is dissected by cutting with scissors against the inner aspect of the hyoid bone
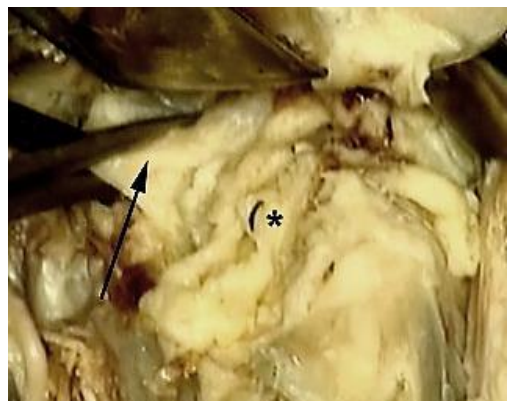
Figure 21b: The submucosa of the vallecula (arrow) is exposed. The fat of the preepiglottic space is included in the resection (asterisk)
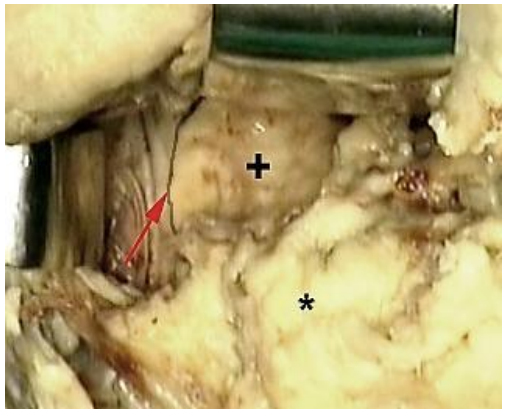
Figure 21c: The cut runs across both valleculae to expose the lingual surface of the epiglottis. Note the fat of the pre-epiglottic space (asterisk), the lingual surface of the epiglottis (+), and the posterior pharyngeal wall and free margin of the epiglottis (red arrow).
1st Vertical cut(Figures 22a, b)
- The 1st vertical cut is made on the side opposite to the tumor; it connects the lateral ends of the superior and inferior horizontal cuts
- The surgeon moves to the head of the patient to look inside the larynx through the superior horizontal cut
- Identify all structures by direct vision and/or palpation before cutting
- Introduce one blade of the scissors through the opening of the superior horizontal cut, while the other blade crosses over the lateral soft tissues of the larynx (Figure 22a)
- Cut through the aryepiglottic fold (if epiglottis is included in the specimen)
- Cut along the anterior surface of the arytenoid (Figure 22b)
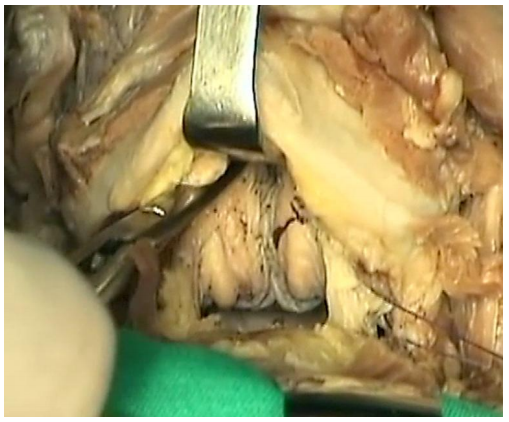
Figure 22a: (View from head of table). The surgeon moves to the head of the patient to perform the 1 st vertical cut through the superior horizontal cut. One blade of the scissors is inside the larynx and the other over the lateral laryngeal soft tissues
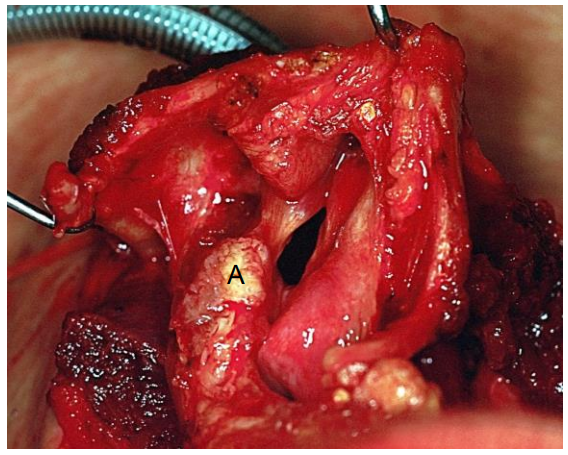
Figure 22b: Surgical view of the larynx from the head of the table. The first vertical cut has been made along the anterior surface of the left arytenoid (A). The left vocal cord is still in place. The right side remains untouched
- Cut the vocal ligament where it attaches to the vocal process
- Cut vertically through the subglottis and along the superior aspect of the cricoid up to the lateral edge of the cricothyrotomy
2nd Vertical cut
- The surgeon then moves back to the patient’s side
- Grip the thyroid laminae with the fingers of both hands, fracture the thyroid cartilage down the midline and open the larynx like a book to expose the endolarynx and the tumor (Figure 23a)
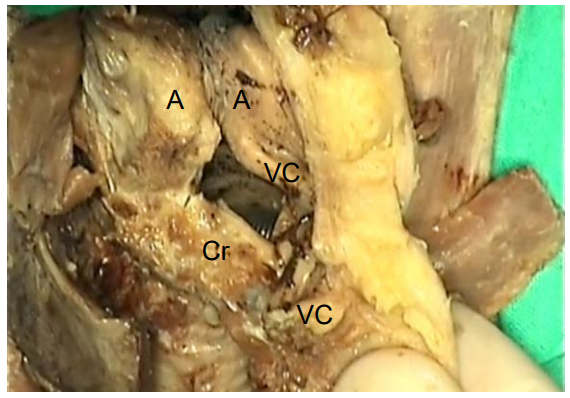
Figure 23a: Thyroid cartilage has been fractured in midline to expose arytenoids (A), cricoid (Cr) and vocal cords (VC)
- Make the 2nd vertical cut as on the 1st (non-tumor) side using a #15 scalpel under direct vision, ensuring free margins (Figures 23b, c, d)
- If needed, the arytenoid is resected, providing that the epiglottis has been preserved
- Frozen section of the margins is encouraged
- This completes the resection, leaving in place the cricoid cartilage, hyoid bone, arytenoid cartilages and epiglottis depending on the extent of the resection (Figure 24).
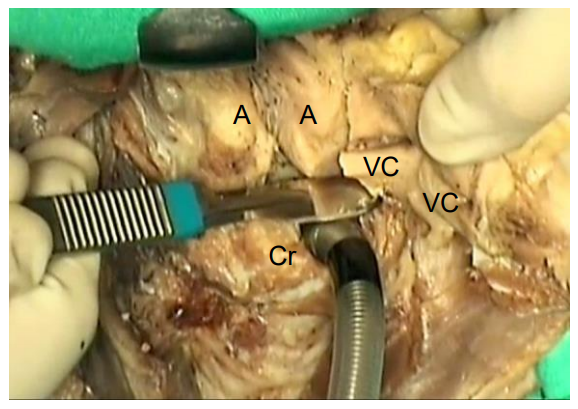
Figure 23b: The endotracheal tube is inserted through the cricothyrotomy. The 2nd vertical cut is being made with a scalpel; Arytenoids (A), cricoid (Cr) and vocal cords (VC)
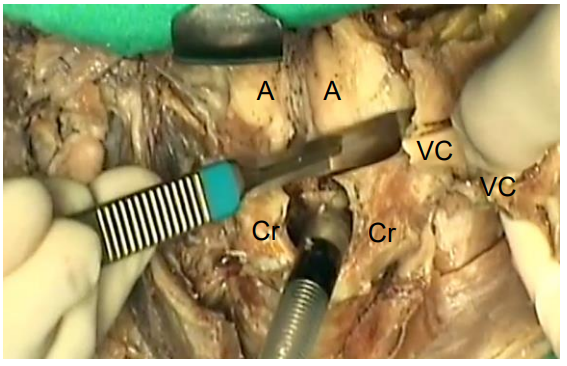
Figure 23c: Final stage of vertical cut
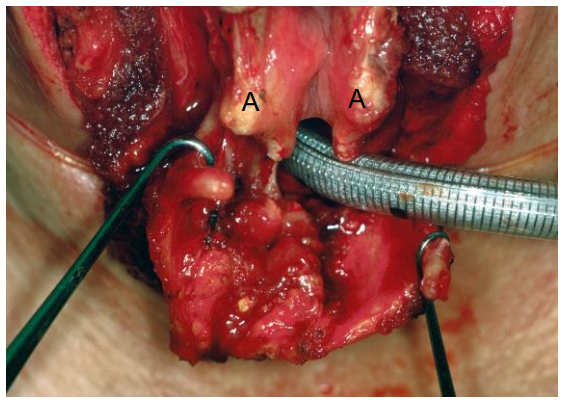
Figure 23d: Surgical view of the larynx before completing the resection. The vertical cut on the left side has been completed. The right vocal cord is the only structure still retaining the larynx in place (A = arytenoid)
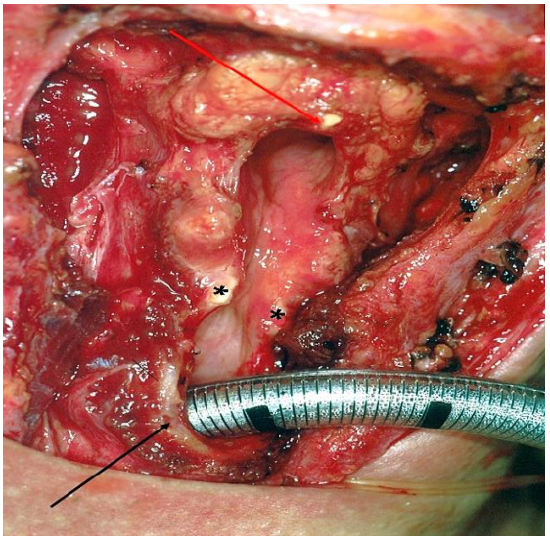
Figure 24: Surgical view of the remaining larynx: Preserved epiglottis (red arrow); vocal processes of arytenoids (asterisks); and cricoid arch (black arrow)
The resected specimen includes the “voice box”: thyroid cartilage, both vocal cords, and both ventricular bands (Figures 1, 25). One arytenoid or the epiglottis may also be included depending on tumor extension.
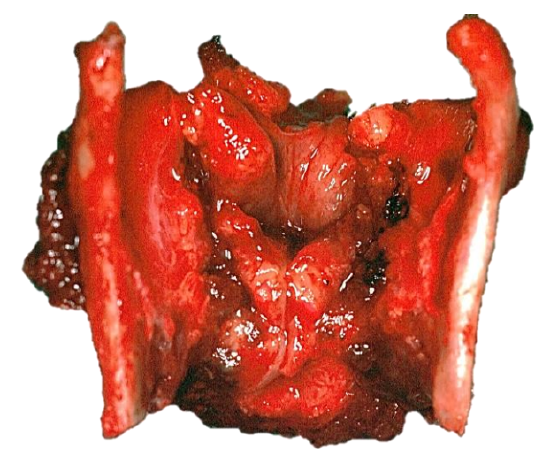
Figure 25: The surgical specimen includes the thyroid cartilage with both vocal cords and ventricular bands
3. Tracheostomy and feeding tube
- To allow one to pull the cricoid up to the level of the hyoid bone, mobilize the trachea by dissecting bluntly with a finger along the anterior tracheal wall taking care not to disturb the tracheal vasculature that enters through its lateral walls (Figure 26)

Figure 26: Dissecting bluntly with a finger along the anterior tracheal wall
- While maintaining the cricoid in this position, create a tracheostomy at the level of the suprasternal skin incision (usually 4th/5th tracheal rings) (Figure 27)
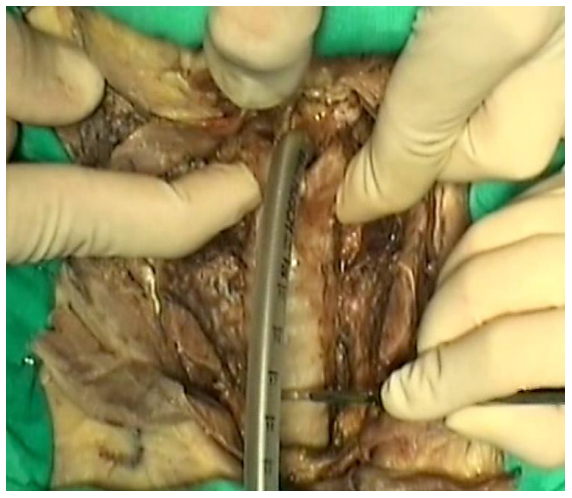
Figure 27: With cricoid abutting hyoid, create a tracheostomy at the level of the suprasternal skin incision
- Resite the endotracheal tube into the new tracheostoma (Figure 28)
- Insert a nasogastric feeding tube under direct vision of the hypopharynx to ensure its proper positioning
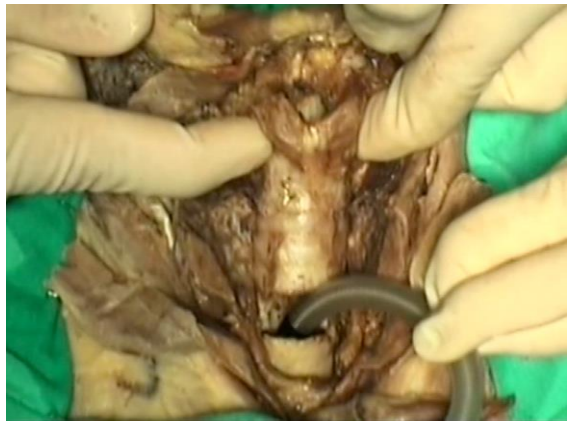
Figure 28: Resiting the endotracheal tube into the new tracheostoma
4. Reconstruction
Arytenoids
- Place two 3-0 vicryl sutures between the superior aspects of the arytenoids and the cricoid arch (Figures 2, 29)
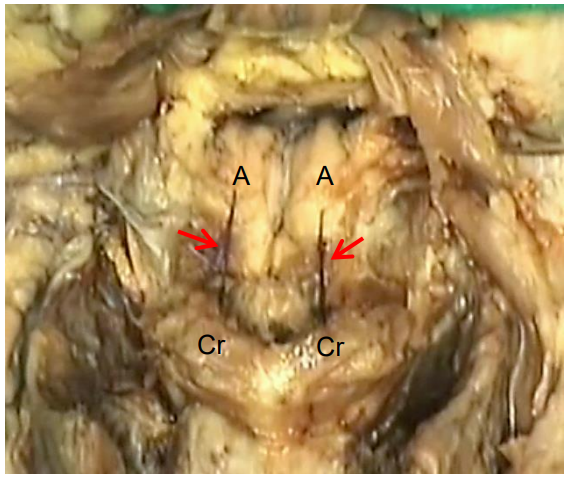
Figure 29: Sutures (red arrows) are placed between each vocal process and the cricoid (Cr) to pull the arytenoids (A) forwards. Do not tie them too tightly as their role is simply to prevent posterior rotation of the arytenoids during healing
- Do not tie the sutures too tightly
- The sutures avoid posterior rotation of the arytenoid and allow healing to occur in the correct position; by maintaining the arytenoids in a more anterior position, closure of the laryngeal entry during deglutition is improved10
Closing the airway
- Cricohyodopexy/CHP (epiglottis resected) or cricohyoidoepiglottopexy / CHEP (epiglottis preserved) is used to close the airway
- Pass three #1 vicryl sutures around the cricoid arch and the body of the hyoid
- One suture is placed in the midline and the other two are placed 0.5 cm to each side (Figures 2, 30a-e)

Figure 30a: Cricohyoidoepiglottopexy
- The needle is passed from outside through the cricotracheal membrane and is directed submucosally through the posterior surface of the cricoid arch (Figure 30b)
- It re-enters again through the inferior border of the sectioned epiglottis, runs 1-2 cm between the epiglottic cartilage and the pre-epiglottic fat and exits through the pre-epiglottic fat (Figure 30c)
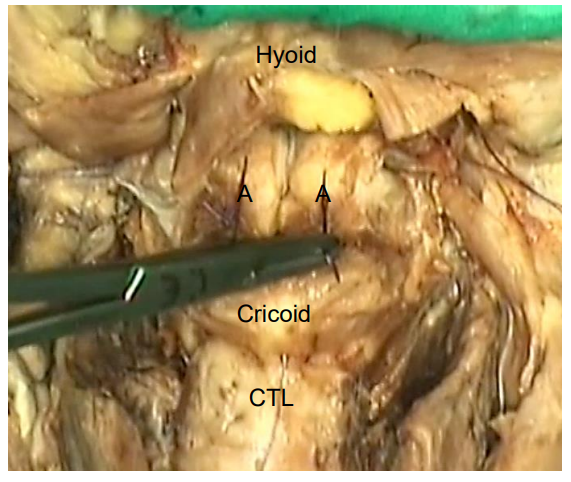
Figure 30b: The needle is passed through the cricotracheal ligament (CTL), runs submucosally on the posterior surface of the cricoid arch, and exits at its superior border; note sutures pulling arytenoids (A) forwards
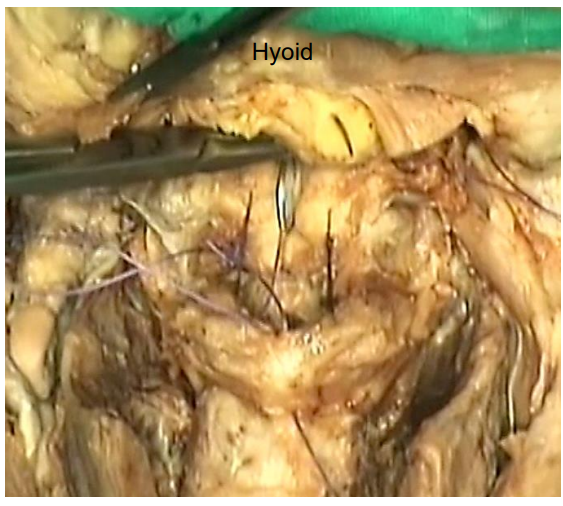
Figure 30c: The same needle re-enters between the epiglottic cartilage and preepiglottic fat, runs a few cm parallel to the anterior surface of the epiglottis, and exits through the epiglottic fat below the hyoid
- Finally, it surrounds the posterior and superior aspect of the body of the hyoid bone and exits above the bone through the suprahyoid musculature (Figure 30d)
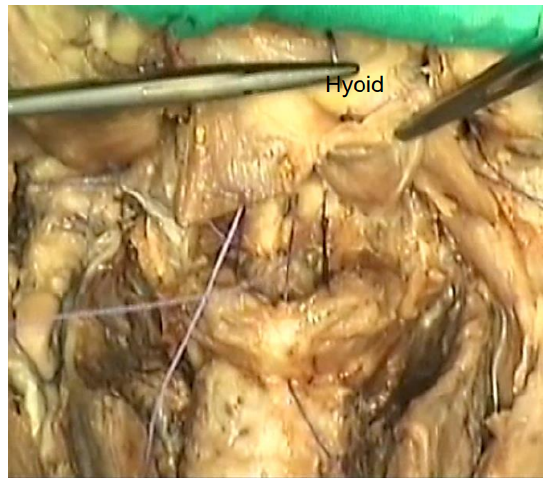
Figure 30d: Finally, the needle re-enters and passes behind the hyoid body, and exits through the suprahyoid muscles
- If the epiglottis has been preserved, it is important that the suture runs 1-2 cm parallel to the epiglottic cartilage in order to prevent inversion of the epiglottis that may compromise the outcome11. If the epiglottis has been resected, the sutures are passed around the cricoid cartilage and hyoid bone submucosally in a similar manner
- The 1st throw of the knots of the two lateral sutures are tightened simultaneously by the surgeon and the assistant
- Tighten the midline suture; while maintaining tension on the two other sutures, throw at least 3 knots on every suture to avoid dehiscence of the pexy (Figure 30e)
- Align the anterior borders of the cricoid and the hyoid; if this is not done then the size of the neoglottis is reduced and the functional outcome may be compromised
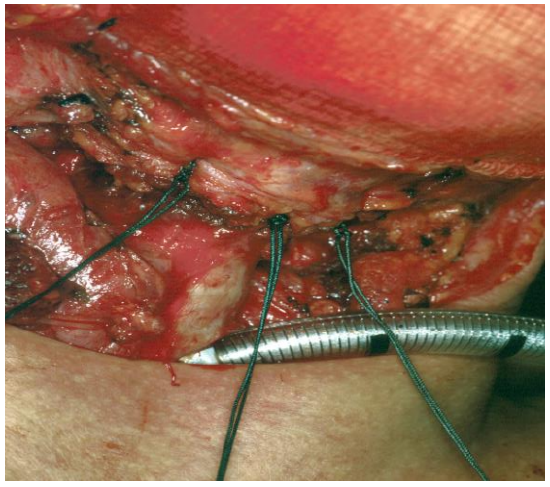
Figure 30e: Surgical view of the 3 pexy stitches after being tied
Pyriform sinuses
- With loss of support of the thyroid laminae, the pyriform sinuses lose their shape and collapse
- Sutures were earlier inserted into the submucosa of the pyriform sinuses during the approach stage of the operation (Figure 16)
- To restore the shape of the sinuses, use these sutures to hitch the outer surfaces of the pyriform sinuses to each side of the pexy (Figure 31)
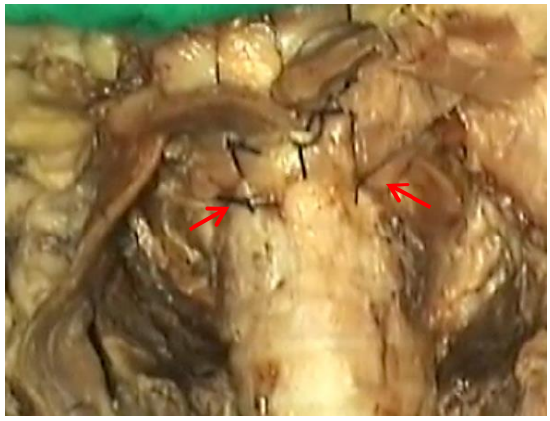
Figure 31: After performing the cricohyoido(epiglotto)pexy the pyriform sinuses are pulled forwards by suturing the stitches (red arrows) to the anterior tracheal wall
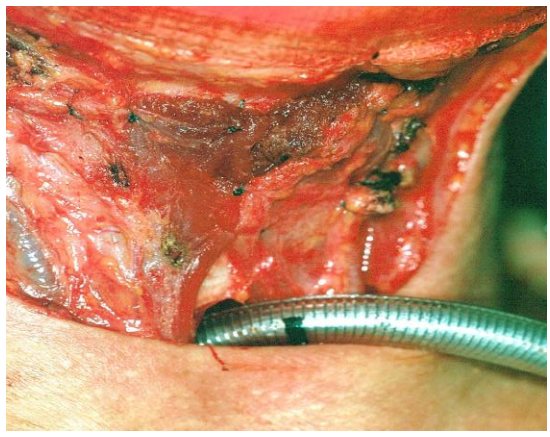
Figure 32: The strap muscles are sutured over the cricohyoidoepiglottopexy. The tracheostomy is secured in its final position
- Suture the strap muscles to the hyoid bone with vicryl to cover the pexy (Figure 32)
- Insert a single suction drain that crosses the midline; bilateral drains are inserted if neck dissections have been done
- Suture the skin, leaving a gap in the lower midline to introduce a cuffed tracheostomy tube
Postoperative Care
- A slightly compressive dressing is placed around the neck and changed every day for 5-7 days
- Drains are maintained for 2-3 days
- Some surgeons use prophylactic antibiotics during the 1st postoperative days, but we do not think it necessary unless there are factors that may favor infection
- Tracheostomy tube
- The cuff is deflated 24 hrs after surgery
- Significant coughing is guaranteed for 5-10 min
- If the cough persists after a few minutes, the cuff is reinflated and the maneuver is repeated 24 hrs later
- The sooner that the cuff can be left deflated, the quicker the recovery will be
- An uncuffed fenestrated tracheostomy tube is inserted as soon as the patient tolerates the cuff deflated for 24-48 hours
- The tube is plugged as soon as it is comfortably tolerated
- The tracheostomy tube is removed when the patient tolerates a plugged tube for 24-48 hrs continuously (including at night). This usually happens 7-14 days after surgery
- The tracheostomy wound is occluded with a dressing while it heals by second intention
- Swallowing
- Provide nutrition by nasogastric feeding tube
- If no complications have occurred, attempt oral nutrition on Day 10
- Use “supraglottic swallow” and the “chin tuck” techniques, starting with yogurt or custard consistencies. The patient takes a deep breath and holds it, lowers the head until the chin touches the chest, introduces a small volume of food and swallows twice while maintaining this position, elevates the head and coughs immediately after the 2nd swallow, and subsequently breathes normally. After 2-3 attempts a significant cough will be noted. The patient then rests for 1-2 hours and tries again
- As swallowing is progressively better tolerated, the supraglottic swallow and chin tuck techniques are abandoned
- A noticeable improvement in swallowing occurs when the tracheostomy tube is removed
- Thicker and more liquid consistencies are gradually introduced
- Once oral intake is adequate to ensure correct nutrition, the feeding tube is removed (usually 10-20 days after surgery)
- This process is prolonged following resection of the epiglottis or one arytenoid
Radiotherapy
If required, postoperative radiotherapy is commenced when the healing process is complete i.e. 3-4 weeks after surgery. The authors used to leave the tracheostomy tube in situ until the end of radiotherapy as many patients develop oedema that requires endoscopic resection (e.g. with CO2 laser) prior to definitive decannulation. Swallowing rehabilitation is also retarded by radiotherapy, and some patients need a new feeding tube during this period.
Outcomes
Several large series12-16 have demonstrated that the oncologic results of supracricoid laryngectomy are equivalent to those of total laryngectomy, providing that candidates are properly selected and negative margins are obtained on frozen section. The authors previously reported a 5-year actuarial local control rate of >90% for T1- T2 tumors, and ca. 70% for T3 tumors 17.
Laryngeal function is maintained in a large proportion of patients. Decannulation and adequate oral intake are achieved in >90% of patients7, 12, 13, 18.
Quality of life has been shown to be better than that of patients submitted to total laryngectomy with tracheoesophageal puncture16. In a previous study, the authors reported excellent voice and swallowing in a group of patients as measured by the Voice Handicap Index and the MD Anderson Dysphagia Inventory7.
Comparison with other treatments
The indications for supracricoid laryngectomy overlap with those of vertical partial laryngectomy and its permutations. However, while voice after vertical laryngectomy is very breathy, patients undergoing supracricoid laryngectomy preserve a rough but powerful voice with excellent phonation times. For this reason, supracricoid laryngectomy has displaced vertical laryngectomy techniques in the authors’ standard surgical armamentarium. Supraglottic carcinoma without glottic invasion is more properly treated with horizontal supraglottic laryngectomy, as voice quality is much better than after supracricoid laryngectomy. However, the latter allows one to treat supraglottic tumors with glottic invasion with open partial laryngectomy. In recent decades, transoral endoscopic laser resection of early and advanced carcinoma has been described. The main advantages of endoscopic procedures are the avoidance of tracheostomy in some patients and quicker swallowing rehabilitation. However, limited exposure may compromise a surgeon’s ability to obtain negative margins in bulky tumors, whereas long-term functional results do not differ from those of open partial laryngectomy. Moreover, the cost of a laser or a robot limits its application in many developing countries. Chemoradiation is often considered to be a more sophisticated treatment for laryngeal cancer. Although the overall survival is considered similar to total laryngectomy, local recurrence generally requires salvage surgery. The local control reported by the largest series of supracricoid laryngectomies for locally advanced carcinoma is superior to that reported by the main studies of nonsurgical treatment19, 20. Moreover, chemoradiated patients experience late toxicity that worsens their quality of life. Finally, the cost of chemoradiation is far higher than that of supracricoid laryngectomy. Total laryngectomy has been the classic treatment for laryngeal carcinoma for many years. While total laryngectomy patients experience excellent swallowing and voice can be successfully restored by different procedures21, the presence of a permanent tracheostoma is an unavoidable handicap that worsens their quality of life16, 22, 23.
Summary of authors’ routine practice
- Unilateral vocal cord cancers with preserved mobility and minimal invasion of the contralateral cord and/or ventricular band are treated by endoscopic resection (or laryngofissure if adverse anatomical features exist)
- More advanced glottic cancers are resected by supracricoid laryngectomy
- Supraglottic cancers without glottic invasion are managed by horizontal supraglottic laryngectomy (only small supraglottic tumors are endoscopically resected)
- Supracricoid laryngectomy is used for supraglottic cancer that invades the glottis
- Chemoradiotherapy is offered to patients that cannot be managed with any form of partial laryngectomy due to tumor or patient factors
- Total laryngectomy is currently considered a first line treatment for laryngeal and hypopharyngeal cancer when a tumor exceeds the limits of partial laryngectomy and presents with adverse factors for chemoradiation (bulky, cartilage invasion), or when the patient’s age or comorbidities contraindicate other surgical or non-surgical treatments
Conclusions
Supracricoid partial laryngectomy is a versatile technique for the treatment of glottic and transglottic carcinoma. The oncologic results are supported by several long-term series. Long-term functional results are comparable to transoral procedures in the treatment of T1-T2 glottic tumors, and to chemoradiation protocols in T3-T4 glottic and transglottic tumors. However, careful selection of candidates is mandatory to achieve these results.
References
- Majer EH, Rieder W. [Technic of laryngectomy permitting the conservation of respiratory permeability (cricohyoidopexy)]. Ann Otolaryngol. 1959; 76:677-81
- Piquet JJ, Desaulty A, Decroix G. [Cricohyoido-epiglottopexy. Surgical technic and functional results]. Ann Otolaryngol Chir Cervicofac. 1974;91 (12):681-6
- Laccourreye O, Ross J, Brasnu D, Chabardes E, Kelly JH, Laccourreye H. Extended supracricoid partial laryngectomy with tracheocricohyoidoepiglottopexy. Acta Otolaryngol. 1994;114-(6):669- 74
- Yang H, Shen W, Xiong X. [Extended supracricoid partial laryngectomy with tracheocricohyoidoepiglottopexy and tracheocricohyoidoglottopexy]. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2008;22(18):840-1
- Allegra E, Franco T, Trapasso S, Domanico R, La Boria A, Garozzo A. Modified supracricoid laryngectomy: oncological and functional outcomes in the elderly. Clin Interv Aging. 2012; 7:475-80
- Schindler A, Favero E, Capaccio P, Albera R, Cavalot AL, Ottaviani F. Supracricoid laryngectomy: age influence on long-term functional results. Laryngoscope. 2009; 119(6):1218-25
- Castro A, Sanchez-Cuadrado I, Bernal-dez R, Del Palacio A, Gavilan J. Laryngeal function preservation fol-lowing supracricoid partial laryngec-tomy. Head Neck. 2012;34(2):162-7
- Joo YH, Sun DI, Cho JH, Cho KJ, Kim MS. Factors that predict postoperative pulmonary complications after supracricoid partial laryngectomy. Arch Otolaryngol Head Neck Surg. 2009; 135(11):1154- 7
- Chow JM, Block RM, Friedman M. Preoperative evaluation for partial laryngectomy. Head Neck Surg. 1988; 10(5):319-23
- Seino Y, Nakayama M, Okamoto M, Hayashi S. Three-dimensional computed tomography analysis of neoglottis after supracricoid laryngectomy with cricohyoidoepiglottopexy. J Laryngol Otol. 2012;126(4):385-90
- Nakayama M, Okamoto M, Seino Y, Miyamoto S, Hayashi S, Masaki T, et al. Inverted epiglottis: a postoperative complication of supracricoid laryngec-tomy with cricohyoidoepiglottopexy. Auris Nasus Larynx. 2010;37(5):609-14
- Chevalier D, Laccourreye O, Brasnu D, Laccourreye H, Piquet JJ. Cricohyoidoepiglottopexy for glottic carcinoma with fixation or impaired motion of the true vocal cord: 5-year oncologic results with 112 patients. Ann Otol Rhinol Laryngol. 1997;106(5):364-9
- Mercante G, Grammatica A, Battaglia P, Cristalli G, Pellini R, Spriano G. Supracricoid Partial Laryngectomy in the Management of T3 Laryngeal Cancer. Otolaryngol Head Neck Surg. 2013 Aug 6. [Epub ahead of print]
- Page C, Mortuaire G, Mouawad F, Ganry O, Darras J, Pasquesoone X, et al. Supracricoid laryngectomy with cricohyoidoepiglottopexy (CHEP) in the management of laryngeal carcinoma: oncologic results. A 35-year experience. Eur Arch Otorhinolaryngol. 2013;270(6):- 1927-32
- Pinar E, Imre A, Calli C, Oncel S, Katilmis H. Supracricoid partial laryngectomy: analyses of oncologic and functional outcomes. Otolaryngol Head Neck Surg. 2012;147(6):1093-8
- Weinstein GS, El-Sawy MM, Ruiz C, Dooley P, Chalian A, El-Sayed MM, et al. Laryngeal preservation with supracricoid partial laryngectomy results in improved quality of life when compared with total laryngectomy. Laryngoscope. 2001; 111(2):191-9
- Sanchez-Cuadrado I, Castro A, Bernaldez R, Del Palacio A, Gavilan J. Oncologic outcomes after supracricoid partial laryngectomy. Otolaryngol Head Neck Surg. 2011;144(6):910-4
- Cho KJ, Joo YH, et al. Supracricoid laryngectomy: oncologic validity and functional safety. Eur Arch Otorhinolaryngol. 2010;267(12):1919-25
- Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003; 349(22):2091-8
- Wolf GT. Induction chemotherapy plus radiation compared with surgery plus radiation in patients with advanced laryngeal cancer. The Department of Veterans Affairs Laryngeal Cancer Study Group. N Engl J Med. 1991; 324(24):1685-90
- Torrejano G, Guimaraes I. Voice quality after supracricoid laryngectomy and total laryngectomy with insertion of voice prosthesis. J Voice. 2009; 23(2):240-6
- Herranz J, Gavilan J. Psychosocial adjustment after laryngeal cancer surgery. Ann Otol Rhinol Laryngol. 1999; 108(10):990- 7
- Singer S, Danker H, Guntinas-Lichius O, Oeken J, Pabst F, Schock J, et al. Quality of life before and after total laryngectomy: Results of a multicenter prospective cohort study. Head Neck. 2014 Mar;36(3):359-68. doi: 10.1002/hed.23305
Clinical practice guidelines
- Cancer of Glottis - https://developingworldheadandneckcance rguidelines.com/index-page-glotticcancers/
- Cancer of Supraglottis - https://developingworldheadandneckcance rguidelines.com/index-page-supraglotticcancers/
- Cancer of Hypopharynx - https://developingworldheadandneckcance rguidelines.com/index-pagehypopharyngeal-cancers/
Authors
Alejandro Castro, MD
Department of Otolaryngology
La Paz University Hospital
Madrid, Spain
alejandro.castro@idipaz.es
Javier Gavilán, MD
Professor and Chairman
Department of Otolaryngology
La Paz University Hospital
Madrid, Spain
javier.gavilan@salud.madrid.org
Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za

The Open Access Atlas of Otolaryngology, Head & Neck Operative Surgery by Johan Fagan (Editor) johannes.fagan@uct.ac.za is licensed under a Creative Commons Attribution - Non-Commercial 3.0 Unported License