
1.26: Tracheostomy
- Page ID
- 17648

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
TRACHEOSTOMY
Johan Fagan
Tracheostomy refers to the creation of a communication between the trachea and the overlying skin. This may be done either by open or percutaneous technique. This chapter will focus on the open surgical technique in the adult patient.
Indications
Tracheostomy is done for airway obstruction, respiratory support (assisted ventilation), pulmonary hygiene, elimination of dead space, and treatment of obstructive sleep apnoea.
Preoperative evaluation
Level of obstruction: A standard tracheostomy will not bypass obstruction in the distal trachea or bronchial tree.
Anatomy of the neck: The surgeon should anticipate a difficult tracheostomy in patients with short necks, thick necks, and necks that cannot be extended due to e.g. rheumatoid or osteoarthritis of the cervical spine.
Coagulopathy: A coagulopathy should be corrected prior to surgery. If not completely corrected, then have electrocoagulation available at surgery to aid haemostasis.
Cardiorespiratory status: Patients with upper airway obstruction may have cor pulmonale, or respiratory acidosis. Some patients may be dependent on physiological PEEP to maintain O2 saturation, or an elevated pCO2 to maintain respiratory drive; relieving upper airway obstruction with a tracheostomy may paradoxically cause such patients to stop breathing and become hypoxic.

Figure 1: Tracheal deviation due to tuberculosis
Deviation of cervical trachea: A chest X-ray will alert the surgeon to tracheal deviation due to cervical and mediastinal tumors, or traction on the trachea due to fibrosis (Figure 1).
Laryngeal cancer: If airway obstruction is because of laryngeal cancer, then one should attempt not to enter the tumor during tracheostomy. This may require a lower tracheostomy if tumor involves the cervical trachea. It is prudent to send a sample from the tracheal window for histological examination as involvement by tumor might be useful information for the surgeon subsequently doing the laryngectomy.
Tracheostomy procedure
A tracheostomy is best done in the operating room with good lighting, instrumentation, suction, diathermy and assistance. Patients may cough on inserting the tracheostomy tube; hence eye protection is recommended to prevent transmission of infections such as HIV and hepatitis.
Anesthesia: Unless the patient can safely be intubated or the patient can be ventilated with a mask, a tracheostomy should be done under local anesthesia. If there is concern about the anesthetist’s ability to maintain an airway, then the surgeon should be present during induction; the skin, soft tissue and trachea (into the lumen) should be infiltrated with local anesthesia with adrenaline before induction; and a set of tracheostomy instruments should be set out before induction of anesthesia so that an emergency tracheostomy can be done if required.
Positioning and draping
- Place the patient in a supine position with neck extended by a pillow or bag placed under the shoulders to deliver the trachea out of the thorax and to give adequate access to the cervical trachea.
- Such extension may not be possible in patients with neck injuries, or rheumatoid and osteoarthritis of the cervical spine.
- Some patients with impending airway obstruction may not tolerate a recumbent position; the tracheotomy may then be done with the patient in a sitting position with neck extended.
- Sterilize the skin of the anterior neck and chest and drape the neck.
- If the tracheostomy is being done under local anesthesia, the face be uncovered.
Surface landmarks (Figure 2)
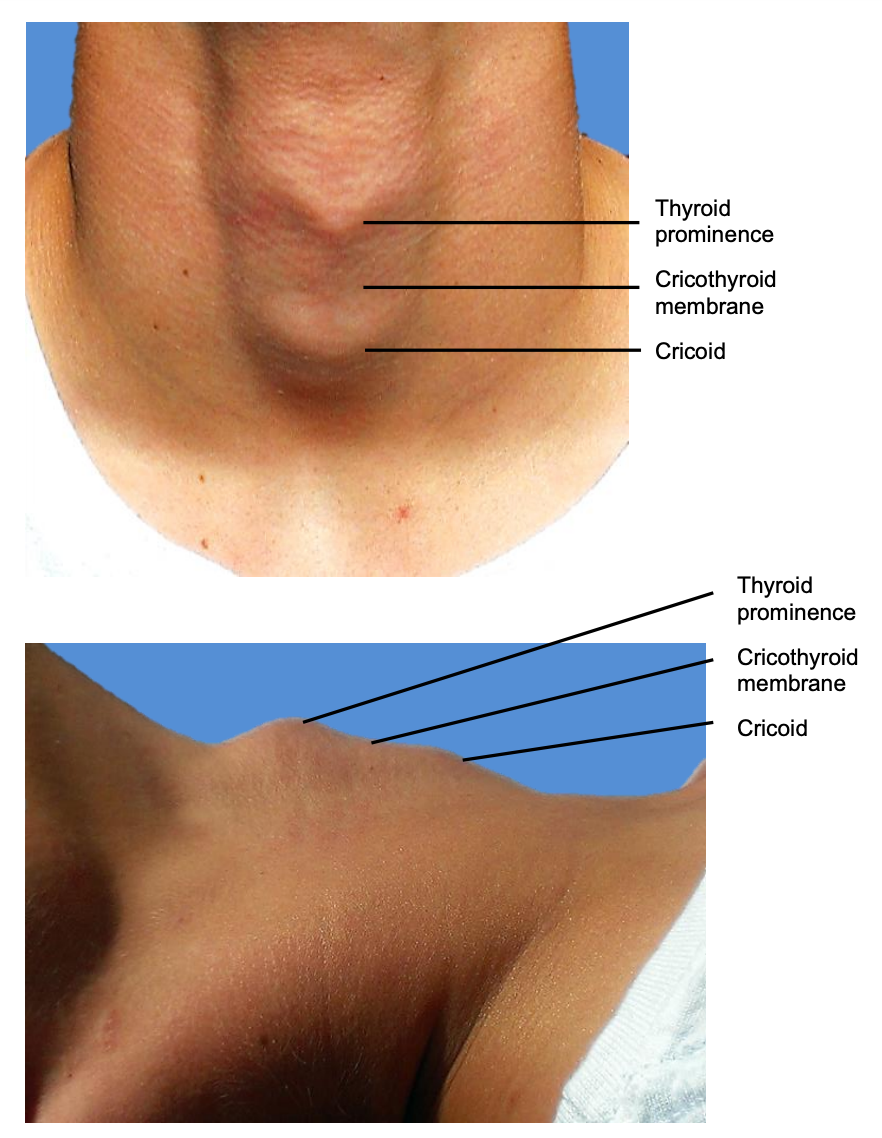
Figure 2: Surface anatomy
- The tracheostomy is created below the 1st tracheal ring to avoid subglottic stenosis as a result of scarring.
- Run your finger up the midline of the neck starting inferiorly at the sternal notch: the 1st prominence encountered is the thyroid isthmus, followed by the cricoid.
- Alternatively, identify the thyroid prominence or “Adam’s apple”. Moving inferiorly the finger slips into the depression of the cricothyroid membrane, followed by the solid prominence of the cricoid cartilage.

Figure 3: Minimum set of instruments.
- Minimum instruments: A minimum set of instruments is demonstrated in Figure 3.
Skin incision
- Make a horizontal incision one fingerbreadth below the cricoid prominence. It is cosmetically preferable to a vertical midline incision.
- Extend the incision through skin and subcutaneous tissue (platysma is generally absent in the midline).
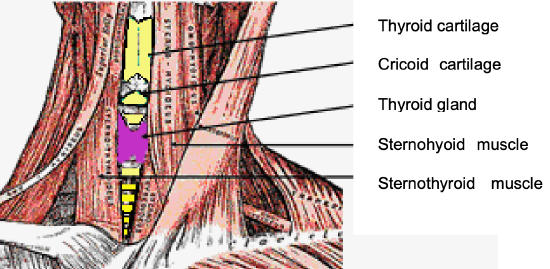
Figure 4: Infrahyoid strap muscles
- Take care not to transect the anterior jugular veins which are just superficial to the strap muscles within the investing cervical fascia. They can be preserved and retracted laterally (Figure 4).
Infrahyoid strap muscles
- Figure 4 illustrates the infrahyoid strap muscles.
- Dissect towards the trachea by parting the tissues with scissors, remaining strictly in the midline in a vertical plane to avoid injury to the inferior thyroid veins.
- Identify the midline cervical fascial plane between the sternohyoid muscles.
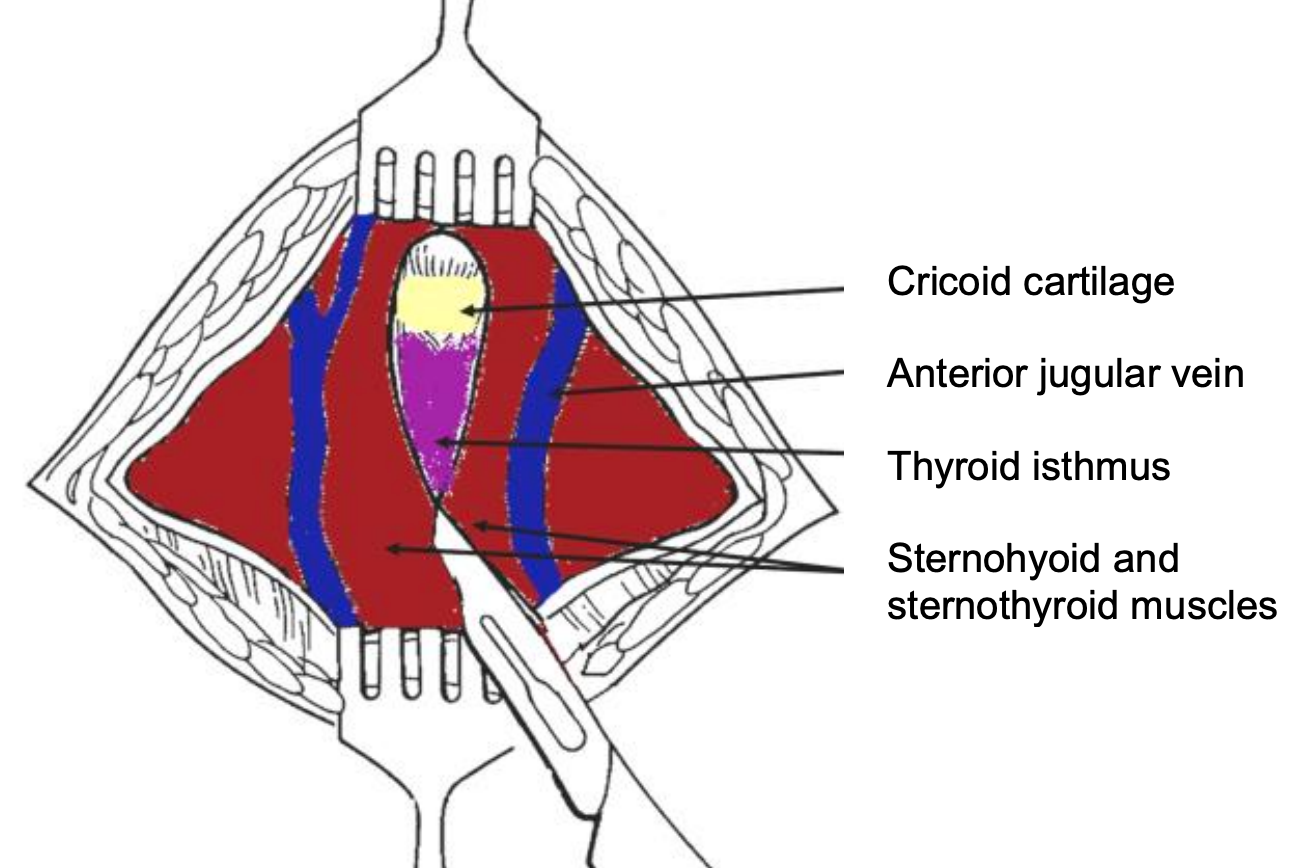
Figure 5: Exposure of anterior jugular veins and cervical fascia
- Divide this intermuscular plane by spreading with a pair of scissors (Figure 5).
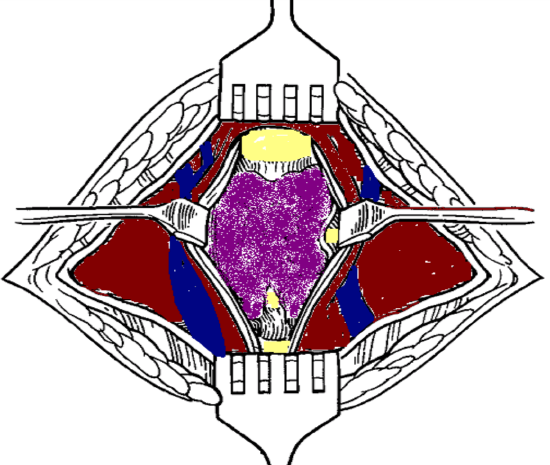
Figure 6: Retracting sternohyoid and sternothyroid muscles exposes the thyroid isthmus
- Repeat this manoeuvre to separate the sternothyroid muscles and retract the muscles laterally (Figure 6).
- The trachea and cricoid can now be palpated.
Thyroid isthmus
- The thyroid isthmus overlies the 2nd/3rd tracheal rings.
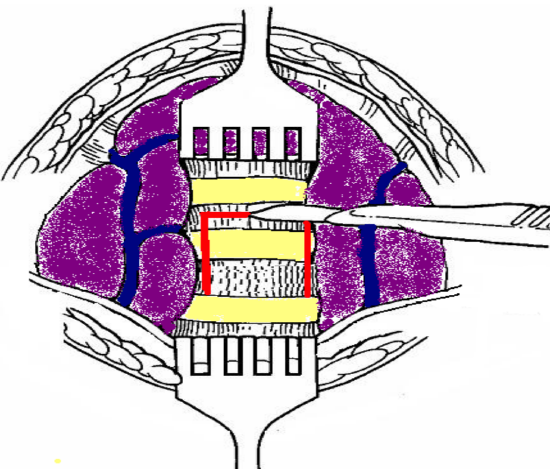
Figure 7: Thyroid isthmus retracted superiorly and an inferiorly based flap cut (along red lines) in anterior tracheal wall
- Retract the isthmus superiorly with Langenbeck retractors to expose the trachea (Figure 7).
- Only very rarely does the thyroid isthmus need to be doubly clamped, divided, and (suture) ligated, or if small, divided with eletrocautery.
Expose trachea
- Expose the infrathyroid trachea by carefully parting the overlying soft tissues with a pair of scissors, taking care not to tear the inferior thyroid veins.
- Ensure that the surgical field is completely dry before proceeding, as it is difficult to achieve haemostasis once the tracheostomy tube has been inserted.
- Should there be doubt about the location of the trachea, or there be concern it being confused with the carotid artery, aspirating air with a needle attached to a syringe will confirm its location.
Create a tracheostoma
- In the awake patient, inject lignocaine into tracheal lumen prior to incising the trachea and inserting the tube to reduce coughing.
- A tracheal hook inserted under a tracheal ring may be used to pull superiorly to deliver the trachea from the chest and to stabilize the trachea.
- The safest tracheostomy in adults is to create an inferiorly based flap raised from the anterior wall of the 3rd and 4th tracheal rings.
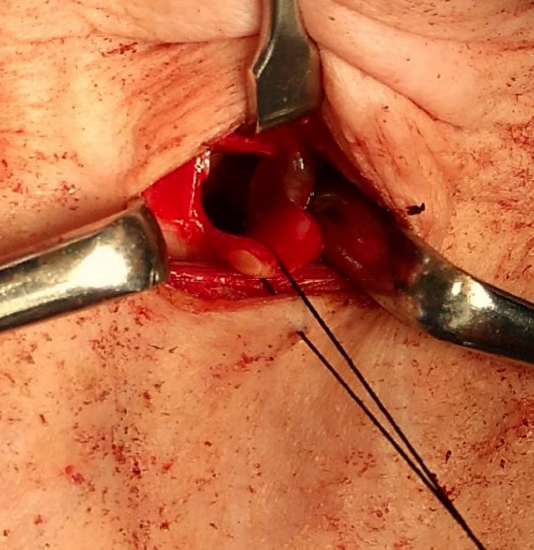
Figure 8: Flap reflected inferiorly with traction suture attached to flap
- A silk traction suture is passed through this anterior tracheal flap and loosely secured to the skin (Figure 8).
- Traction on the suture facilitates reinsertion of the tracheostomy tube in case of accidental decannulation and avoids the tube passing into a false tract anterior to the trachea (Figure 8).
- Alternately one may remove an anterior cartilage segment of the 2nd, 3rd or 4th tracheal rings.
Insertion of tracheostomy tube
- Assess the size of the trachea and select the largest cuffed tracheostomy tube that comfortably fits the tracheal lumen.
- Inject air into the inflatable cuff of the tracheostomy tube to test the integrity of the cuff.
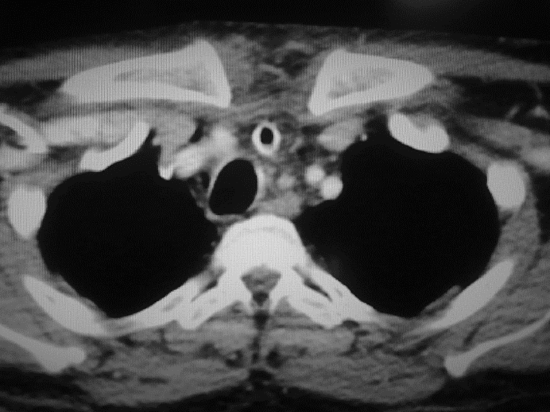
Figure 12: Tracheostomy tube visible in a paratracheal false tract
- Insert the introducer into the tracheostomy tube (Figure 12).
- If the patient has been intubated, the anesthetist slowly withdraws the endotracheal tube until the tip of the tube is visible in the stoma.
- Insert the tracheostomy tube into the tracheostomy under direct vision while applying traction to the silk traction suture attached to the tracheal flap.
- Ensure that the tube has been inserted into the tracheal lumen, and not into a false passage in the paratracheal soft tissues.
- Inflate the cuff, attach the anesthetic tubing.
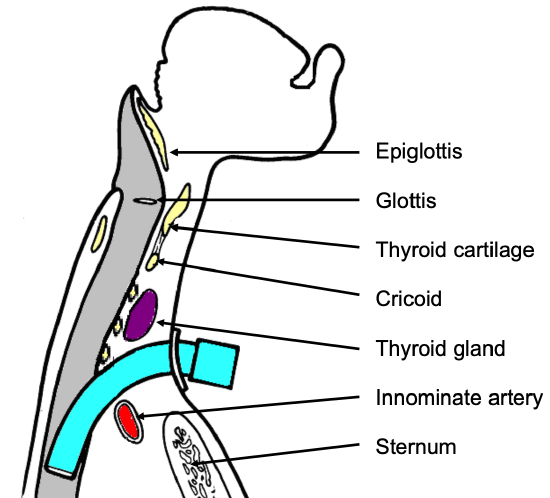
Figure 9: Position of tracheostomy tube
- Hand-ventilate while correct placement of the tube within the trachea is confirmed by checking the expired pCO2, checking for chest movement or listening for breath sounds (Figure 9).
- Do not suture the skin tightly around the tracheostomy tube as this can promote surgical emphysema.
Securing the tracheostomy tube
- Thread tapes through the holes in the flanges of the tracheostomy tube and pass them around the neck.
- Tie them with the neck flexed.
- If the tapes are tied with the neck extended, then they will be too loose when the patient flexes the neck.

Figure 10: Tracheostomy tube secured with Velcro tape
- The ties should be tight enough to admit no more than a single finger under the tape (Figure 10).
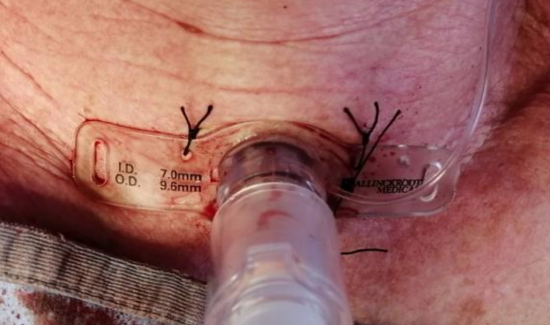
Figure 11: Tracheostomy tube sutured to suprastomal skin
- The author sutures the tracheotomy tube to the skin for the first few days until maturation of the tracheocutaneous tract (Figure 11).
- The sutures can then be removed, and only traditional tracheotomy tapes used.
- Following free microvascular transfer flap reconstruction, tracheostomy tapes should be avoided as tracheal tapes may cause jugular vein compression, thrombosis, venous outflow obstruction and flap failure; the tracheostomy should preferably be sutured to the suprastomal skin (Figure 11).
Pitfalls
Low tracheostomy: A tracheotomy should not be placed below the 4th tracheal ring as:
- The distance between the skin and the trachea increases inferiorly, which makes tracheal intubation more difficult.
- A low tracheostomy may compress and erode the innominate artery which passes between the manubrium sterni and the trachea (Figure 9). This may cause innominate artery erosion and fatal haemorrhage. This may be preceded by a so-called “sentinel bleed.”
High tracheostomy: It is important not to place the tracheotomy above the 2nd tracheal ring, as inflammation may cause subglottic oedema, chondritis of the cricoid cartilage, and subglottic stenosis.
Paratracheal false tract (Figure 12): Inadvertent extratracheal placement of the tracheostomy tube can be fatal. It is recognized by the absence of breath sounds on auscultation of the lungs, high ventilatory pressures, failure to ventilate the lungs, hypoxia, absence of expired CO2, surgical emphysema, and an inability to pass a suction catheter down the bronchial tree, and on chest X-ray.
Surgical emphysema, pneumomediastinum, and pneumothorax: Injury to the pleural domes is more likely to occur in children, struggling patients and patients on positive pressure ventilation. It can be complicated by a tension pneumothorax. Hence auscultation of the chest and a CXR should be performed after tracheostomy, especially in ventilated patients. Surgical emphysema may also be promoted by suturing the tracheostomy wound around the tracheostomy tube.
Airway fire: Do not enter the trachea with diathermy as this may cause an airway fire in a patient being ventilated with a high concentration of oxygen.
Choice of Tracheostomy Tube

Figure 13: Plastic low pressure cuffed tracheostomy tube with outer cannula, inner cannula and introducer (L to R)
A variety of tube designs and materials are available. The choice of tube should conform to the indication for which it is to be used. All tubes should have an inner cannula; this can safely be removed and cleaned without a need to remove the outer cannula and hence avoids risking losing the airway (Figure 13).
The following factors may influence the choice of tube:
Tube diameter: Because airway resistance is related to the 4th power of the radius with laminar flow, and the 5th power of the radius with turbulent flow, it is important to select a tube that that fits the trachea snugly. A range of sizes should be available. It also underscores the importance of keeping the tube clean, as accumulation of mucus increases airway resistance not only by reducing the diameter, but also by causing turbulent air flow.

Figure 14: Metal tracheostomy tube with outer cannula, inner cannula and introducer (L to R)
Tracheal seal: A cuffed, plastic tracheostomy tube is used to create a seal with the trachea in patients on positive pressure ventilation, and with fresh tracheostomy wounds (Figure 13) to prevent saliva or blood entering the lower airways. The cuffed tube may be replaced with an uncuffed tube, either plastic or metal (Figure 14) in patients who do not require positive pressure ventilation once the tract between the skin and the trachea has become well defined by granulation tissue at 48 hours, and tracheostomal bleeding has settled.
Tube material: Metal tubes are thinner walled, and hence have a better ratio of outer to inner wall diameter, thereby optimizing airway resistance (Figure 14).

Figure 15: Tracheostomy tube with adjustable flange
Tube length: Patients with very thick necks can be fitted with a tracheostomy tube with a flange that can be adjusted up or down the shaft of the tube (Figure 15). Tube length may also need to be adjusted when the carina is close to the tracheostoma or with tracheal stenosis or tracheomalacia distal to the tracheostoma that needs to be stented by the tube. Chest and neck X-rays are of value to determine the required length.
Tube shape: Laryngectomy patients require shorter tubes with a gentler curvature to conform to the stoma and the trachea.
Neck Flange: The neck flange should conform to the shape of the neck and fit snugly against the skin to avoid excessive tube movement, accidental decannulation, and soft tissue trauma.

Figure 16: Fenestrated tracheostomy tube

Figure 17: Speaking valve that fits onto the end of a tracheostomy tube and permits hands-free speech
Phonation: Patients with uncuffed tubes or fenestrated tubes (Figure 16) can phonate by occluding the end of the tracheostomy tube with a finger which permits air to bypass the tube and to pass through the larynx. Speaking valves fitted to the ends of tracheostomy tubes are one-way valves that open on inspiration, but close on expiration, thereby directing expired air through the larynx and permit hands-free speech (Figure 17). Fenestrated tubes with speaking valves are particularly well suited to patients with obstructive sleep apnoea, as they can have normal speech by day with the valve in place but uncap the tracheostomy tube at night to ensure unobstructed breathing.

Figure 18: Tracheostomy with suction port
Suction port: In patients with secretions pooling above the cuff e.g. a laryngectomy patient with a pharyngocutaneous fistula, one can protect the patient from aspirating saliva or feeds by inserting a tracheostomy tube with a suction channel that is connected to negative suction (Figure 18).
Postoperative care
Pulmonary oedema: This may occur following sudden relief of airway obstruction and reduction in high intraluminal airway pressures. It may be corrected by CPAP or positive pressure ventilation.
Respiratory arrest: This may occur immediately following insertion of the tracheostomy tube and is attributed to the rapid reduction in arterial pCO2 following restoration of normal ventilation, and hence loss of respiratory drive.

Figure 19: Tracheostomy bib
Humidification: Tracheostomy bypasses the nose and upper aerodigestive tract which normally warms, filters, and humidifies inspired air. To avoid tracheal desiccation and damage to the respiratory cilia and epithelium and obstruction due to mucous crusting, the tracheostomy patient needs to breathe humidified warm air by means of a humidifier, heat and moisture exchange filter, or a tracheostomy bib (Figure 19).
Pulmonary Toilette: The presence of a tracheostomy tube and inspiration of dry air irritates the mucosa and increases secretions. Tracheostomy also promotes aspiration of saliva and food as tethering of the airway prevents elevation of the larynx during swallowing. Patients are unable to clear secretions as effectively as a tracheostomy prevents generation of subglottic pressure, hence making coughing and clearing secretions ineffective; it also disturbs ciliary function. Therefore, secretions need to be suctioned in an aseptic and atraumatic manner.
Cleaning the tube: Airway resistance is related to the 4th power of the radius with laminar flow, and the 5th power of the radius with turbulent flow. Therefore, even a small reduction of airway diameter and/or conversion to turbulent airflow as a result of secretions in the tube can significantly affect airway resistance. Therefore, regular cleaning of the inner cannula is required using a pipe cleaner or brush.
Securing the tube: Accidental decannulation and failure to quickly reinsert the tube may be fatal. This is especially problematic during the 1st 48 hours when the tracheocutaneous tract has not matured and attempted reinsertion of the tube may be complicated by the tube entering a false tract. Therefore, the tightness of the tracheostomy tapes should be regularly checked. Traction sutures on the tracheal flap facilitate reinsertion of the tracheotomy tube.
Cuff pressures: When tracheostomy tube cuff pressures against the tracheal wall mucosa exceed 30 cm H20, mucosal capillary perfusion ceases, ischemic damage ensues and tracheal stenosis may result. Mucosal injury has been shown to occur within 15 minutes. Therefore, cuff inflation pressures of >25 cm H20 should be avoided. Several studies have demonstrated the inadequacy of manual palpation of the pilot balloon to estimate appropriate cuff pressures. Measures to prevent cuff related injury include:
- Only to inflate the cuff if required (ventilated, aspiration).
- Minimal Occluding Volume Technique: Deflate the cuff, and then slowly reinflate until one can no longer hear air going past the cuff with a stethoscope applied to the side of the neck near the tracheostomy tube (ventilated patient).
- Minimal Leak Technique: The same procedure as above, except that once the airway is sealed, slowly to withdraw approximately 1mL of air so that a slight leak is heard at the end of inspiration.
- Pressure gauge: Regular or continuous monitoring of cuff pressures.
- Transport in unpressurized aircraft: Fill the cuff with water or saline as the reduction in air pressure during flight causes an air-filled cuff to expand.
Decannulation
A tracheostomy tube can be removed once the cause of the airway obstruction has been resolved. If any doubt exists about adequacy of the airway e.g. following pharyngeal or laryngeal surgery, then the tracheostomy tube is first downsized so that the patient can breathe freely past the tube. The tube is then plugged. The patient should be closely observed during this time and may be monitored with pulse oximetry. If the patient can tolerate the tracheostomy tube being plugged overnight, it can then be removed. The tracheostomy wound is covered with an occlusive dressing, and generally heals within a week without suturing the skin.
Percutaneous dilational tracheostomy surgical technique
Closure of pediatric tracheocutaneous fistula – surgical technique
Author
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za