
1.46: Surgical Management of Facial Fractures
- Page ID
- 17687

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
SURGICAL MANAGEMENT OF MAXILLOFACIAL TRAUMA
Prabhat Bhama, Mack Cheney
Maxillofacial trauma is typically caused by blunt trauma due to interpersonal violence, moving vehicle accidents (MVA), falls, or sporting activities1. Because these activities transcend cultural and geographic borders, maxillofacial trauma remains a global health issue. Technological advances have resulted in faster methods of transportation and with these developments maxillofacial trauma has become a major public health issue also in the developing world. Although management of the airway and cardiopulmonary system take precedence, facial injuries demand attention because of their potential for long-term impact on quality of life (QOL) and the patient’s psychological wellbeing2 as the face houses many vital structures necessary for sight, hearing, speech, olfaction, and mastication.
Pathophysiology
When energy transferred to a bone exceeds its stress tolerance, a fracture may result. Several factors determine if and how a bone fractures: the amount of energy transferred to the bone e.g. mechanism of injury, speed of collision, airbag deployment etc; vectors of forces; and the characteristics of the tissue involved e.g. anatomic location of impact and quality/health of the bone.
A simple fracture occurs when a single site of discontinuity exists between two bony segments. With a comminuted fracture there are multiple segments of bone. Bone segments protruding through skin are considered open fractures, as are fractures of the alveolar bone and sinuses. They are more susceptible to infection compared to their closed counterparts. Closed fractures are uncommon in the face.
The bony fragments may remain anatomically reduced or can become displaced depending on the mechanism of injury and muscular forces acting on the fragments. The degree of anatomic disruption of fractured segments is referred to as displacement. Blood flow to the fracture site results in callus formation over time followed by mineralization of the callus if the fracture site is immobilized.
Malunion occurs when fracture segments are not reduced and the bone heals in an anatomically incorrect position3. In the face, this can cause significant disfigurement and disability.
Disfigurement occurs because the skin soft tissue envelope (SSTE) of the face is dependent upon the underlying maxillofacial skeletal framework. Anatomic perturbations of the bony framework from maxillofacial trauma manifest as abnormal appearances of the SSTE. Depending on the location of the fracture(s), the aesthetic deformity may be inconspicuous e.g. minimally displaced anterior maxillary sinus wall fractures, or obvious e.g. displaced nasal bone fractures.
Disability occurs when malunion interferes with function. This is most evident with dentoalveolar or mandibular fractures, as malunion can result in dental malocclusion, making mastication difficult or impossible.
The surgeon must ensure that bony fragments are anatomically reduced and stabilized so that when healing is complete, callus formation is minimized to minimize disfigurement and disability. Even when reduction is achieved, the result may not be ideal. Poor blood supply or wound infection may cause delayed union when bone fails to mineralize3 months after reduction and immobilization. Fibrous union may occur (usually within 10 days in adults) if bones are reduced but inadequately immobilized. Non-union may result if bone is lost or the wound is contaminated with foreign material. Therefore, the surgeon must ensure that a fracture site is clean, free of foreign material (insomuch as possible), and well vascularized prior to reduction and immobilization. Antibiotics are sometimes warranted to counter bacterial contamination.
Basic Management Principles
Not all maxillofacial fractures require intervention. The primary goals of repair of craniomaxillofacial (CMF) fractures are restoration of premorbid anatomy and function:
- Craniofacial structure
- Facial height
- Facial width
- Facial projection
- Craniofacial function
- Dental occlusion
Fracture reduction and fixation are best performed in the 1st two weeks following injury5. Strict attention to the following principles optimize bone healing and surgical outcomes
- Anatomic reduction (realignment) of fracture segments
- Fixation (immobilization) of bones across fracture sites in the operating room
- Postoperative immobilization of bones across fracture sites (prevention of reinjury or stress to fracture sites)
- Preventing infection
Anatomic reduction of fractured segments requires a 3-dimensional understanding of maxillofacial anatomy. Nonetheless, substantial individual variation is common, and premorbid photographs or examination of the unaffected side of the face can be beneficial. Intraoperative imaging is also used by some to achieve adequate reduction5, although such technology is costly and time consuming. Bilateral fractures may preclude using the contralateral face as a template. In many cases, the surgeon must reference normal anatomic landmarks. However, when there are no anatomically normal bony landmarks to use as reference, one should first restore dental occlusion, followed by the buttresses of the face (see section on maxillomandibular fixation and anatomy).
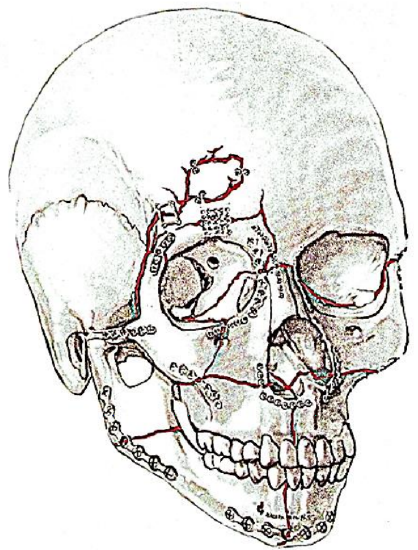
Figure 1: Plating of pan-facial fractures

Figure 2: Plain film following ORIF of multiple fractures

Figure 3: Reconstruction (blue) vs. minilates (grey)
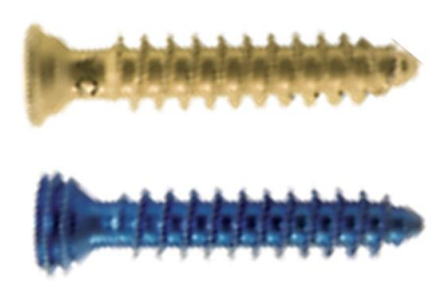
Figure 4: Locking (below) vs. non-locking (above) screws
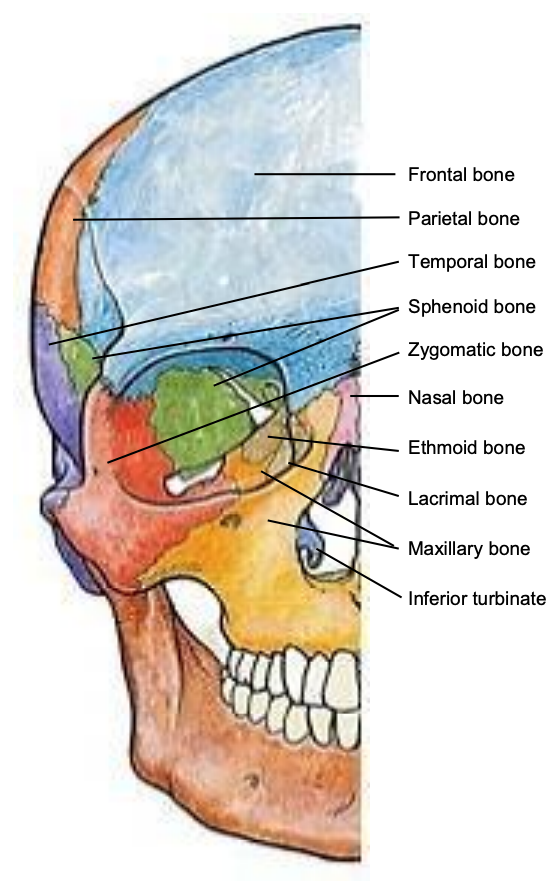
Figure 5: Frontal view of bones of skull
Fixation of bone across fracture sites is done to immobilize the bone against musculoskeletal forces and to permit mineralization to occur. Fixation is generally accomplished using titanium plates secured with screws (Figures 1, 2, 3, 4).
Screws are either self-tapping or self-drilling. Self-tapping screws require predrilling prior to inserting the screws, but also require less force which is advantageous when fixing fragile bony segments. Larger plates and screws provide greater stability and immobilization. Nonlocking plates are typically used for the midface. These plates must be shaped to fit the bone precisely or they will distract the bony segment towards the plate when the screw is engaged.
Locking plates can be helpful when immobilizing mandibular fractures. When used with locking head screws, locking plates do not require exact coaptation of the plate to the bone as the bone is not compressed against the plate (Figures 3, 4). This avoids impairing cortical bone perfusion and provides a more stable fixation when compared to a non-locking system.
Because titanium plates and screws are too expensive for many developing world centers, reliance is placed on stainless steel wire to reduce and fix fractures.
Preventing infection begins with initial management in the emergency unit. Open wounds are copiously irrigated with sterile isotonic fluid. Badly contaminated wounds are thoroughly cleaned and irrigated. Pressurized pulsatile irrigation methods have been demonstrated to be useful in wound debridement6 and are particularly useful to cleanse wounds with particulate matter e.g. sand and road debris. Prophylactic antibiotics to prevent infection when treating non-mandibular maxillofacial fractures have been discouraged 7, although a recent review highlighted the lack of large high quality randomized controlled trials to evaluate antibiotic use in non-mandibular facial fractures. When treating fractures of the mandible, prophylactic antibiotics are likely beneficial when used in the immediate perioperative period 8. In any case, adherence to sterile technique in the operating room and good quality postoperative wound care should not be compromised.
Surgical Anatomy
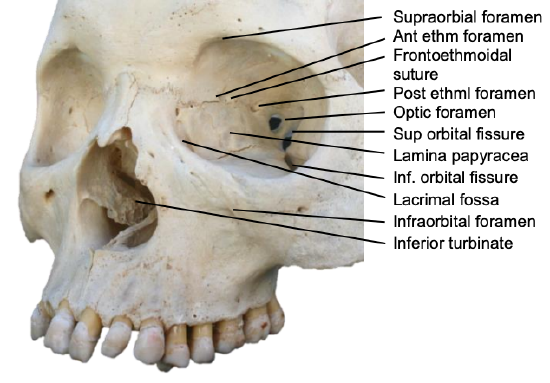
Figure 6: View of orbit
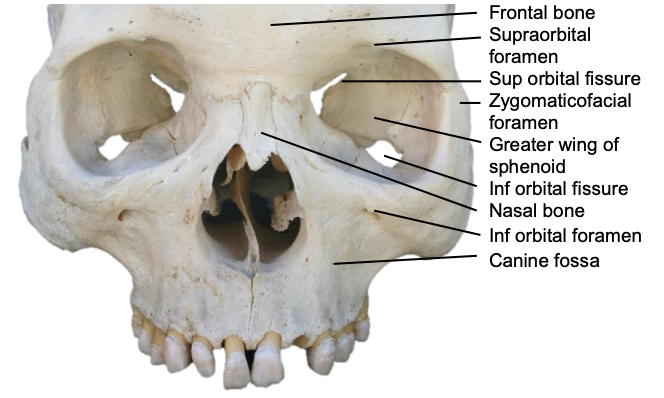
Figure 7: Frontal view of the skull
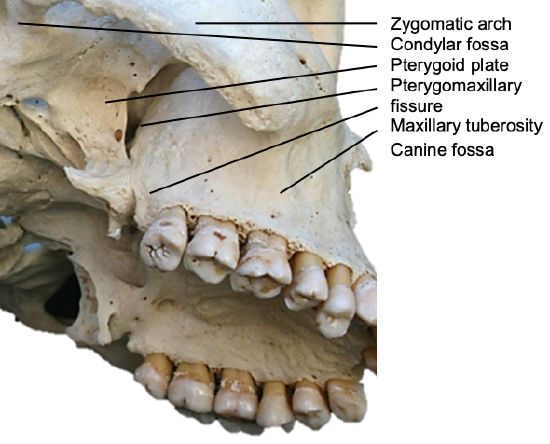
Figure 8: The internal maxillary artery passes through the pterygomaxillary fissure to enter the pterygopalatine fossa
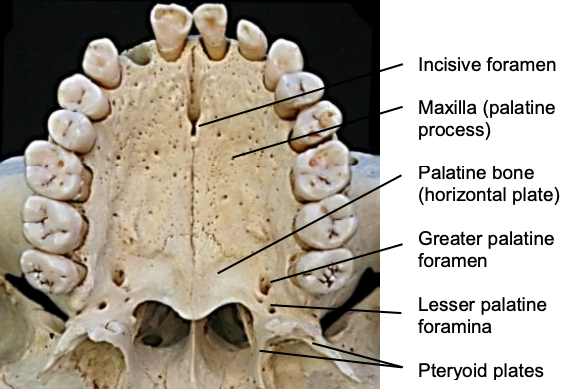
Figure 9: Palatal anatomy
Knowing which fractures require treatment requires a thorough understanding of the anatomy of the craniomaxillofacial (CMF) skeleton and how forces are transmitted (Figures 5-9). This anatomical knowledge, coupled with a detailed history, physical examination, and imaging permit the surgeon to establish a treatment plan for various fracture patterns.
Because of the complexity of the CMF skeleton, it is helpful to divide injuries into the following anatomic regions: frontal sinus, nasoethmoid complex (NEC), zygomaticomaxillary complex (ZMC), midface, palatoalveolar, and mandible.
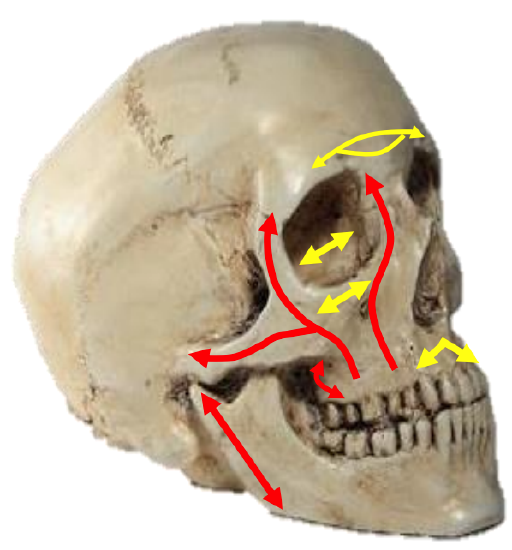
Figure 10: Vertical (red) and transverse (yellow) buttresses
Four paired, vertically-oriented bony pillars (buttresses) i.e. the nasomaxillary (NM), zygomaticomaxillary (ZM), and pterygomaxillary (PM) buttresses10, and the vertical rami of the mandible support the sinus cavities and give structure to the craniofacial skeleton (Figure 10). They resist deformation by the powerful forces of mastication and other vertical forces9.
The NM buttress extends from the nasion inferiorly along the pyriform aperture. The ZM buttress extends from the frontozygomatic suture line inferiorly through zygomaticomaxillary suture line to the maxillary alveolus. The PM buttress extends from the cranial base superiorly to the inferior border of the pterygoid plates. Transversely oriented buttresses include the frontal bar, infraorbital rim and nasal bones, and the hard palate and maxillary alveolus (Figure 10).
It is helpful to think of the face as skin and soft tissue draped over the sinus cavities which are enclosed by thin bone; hence the appearance and structure of the skin depends on the structure of the underlying craniofacial skeleton and the integrity of the buttresses. Repair of maxillofacial injuries is therefore directed at re-establishing relationships between the buttresses and surrounding bone and soft tissue, as well as reduction and stabilization of the integrity of the buttress(es).
Assessment of fractures
History
The craniofacial trauma surgeon generally remains uninvolved with patient care in the emergency department until stabilization of the airway and cardiopulmonary systems is complete. Nonetheless, it is certainly possible that craniofacial trauma may compromise the airway or vascular system in which case the experience of a head and neck surgeon can be particularly helpful. In such scenarios, an abbreviated history can be obtained while surgical intervention is taking place in the emergency department. For instance, a patient with bilateral mandibular fractures may present in airway distress because of posterior displacement of the oropharyngeal tongue. In such a case, anterior traction on the tongue using a penetrating towel clamp or by digitally grasping the tongue with a gauze swab can facilitate endotracheal intubation. In some cases, endotracheal intubation may be difficult or precluded (because of suspected laryngeal injury), necessitating tracheostomy or cricothyroidotomy. In cases of vascular compromise, exsanguination is a risk. Typically, tamponade is crucial for hemostasis in emergency situations until formal wound exploration and repair can be completed. Once the airway, breathing, and circulatory systems have been stabilized, a more thorough history can be obtained.
The surgeon should determine the mechanism of injury i.e. fall, assault, moving vehicle collision, and the speed of the injury. While treatment of the patient can continue without knowing the exact mechanism of injury, information regarding mechanism can help the clinician understand the injury pattern and possibly reveal more inconspicuous injuries. For instance, a patient involved in a high-speed motor vehicle collision will typically be at higher risk for more severe injuries to the craniofacial skeleton. Knowing this information may encourage a clinician to order more comprehensive imaging studies.
In addition to the mechanism of injury, the time and location of the injury can be important. These factors can provide clues regarding the status of the patient’s wounds i.e. presence of debris, risk of infection, etc. It is also crucial to ascertain the condition of the patient when the first respondents arrived e.g. was the patient unconscious, cooperative, or combative? This information can provide clues regarding the neurologic status of the patient. The Glasgow Coma Scale (GCS) on arrival of the first responders is information typically presented to the trauma surgeon.
It is not uncommon that patients with craniofacial injuries were under the influence of alcohol or drugs when they sustained an injury. This information should also be obtained.
In an awake and appropriately responsive patient, it is helpful to obtain a complete history directly from the patient as well. Important questions to ask include:
- Neurologic status relating to the head and neck (pain, paraesthesia, etc.)
- Visual changes
- Changes in dental occlusion
- Changes in hearing
- Changes in smell and/or taste
Once the patient’s complaints have been documented, a complete past medical and surgical history should be obtained. The surgeon should be aware of the status of the cervical spine which may preclude positioning changes in the operating room. Additionally, a list of current medications, allergies, family history and review of systems should be obtained. The patient’s tobacco, alcohol, and illicit drug use history should be noted.
Clinical examination
A complete head and neck examination is performed. This includes a neurological examination which begins with assessment of the patient’s sense of person, place, and time. Cranial nerves II-XII are examined. Visual acuity, pupillary light reflexes, and extraocular movements are assessed. Facial sensation should be noted in all three divisions of the Vn. The motor division of the Vn is examined by asking the patient to bite down while palpating the masseter muscle. Facial nerve function should be carefully examined by asking the patient to raise the eyebrows, close the eyes tightly, smile, purse lips, puff cheeks, and depress the lower lip. The cochlear division of the VIIn can be grossly assessed using a conversational voice, and more detailed information regarding audiologic status can be obtained with a tuning fork exam. The IXn and Xn can be tested with the gag reflex and the voice quality. XIn function can be examined via shoulder shrug and head turn. The XIIn can be examined by assessment of tongue movement.
The scalp should be carefully examined for lacerations, foreign debris, or hematomas.

Figure 11: Battle’s sign that appeared four days after the temporal bone fracture
Otoscopy is essential to rule out external auditory canal lacerations which can result in canal stenosis if left untreated. The tympanic membrane should be visualized to rule out hemotympanum, which may be an indicator of a temporal bone fracture. Clear or thin bloody otorrhoea may be due to cerebrospinal fluid (CSF) leakage. In such cases, fluid should be collected and sent for beta-2 transferrin analysis. The mastoid bone should then be examined for Battle’s sign (Figure 11) along with the auricle.

Figure 12: Halo sign of CSF mixed with blood
Nasal examination is important to rule out obvious fractures. Anterior rhinoscopy is performed to rule out septal hematoma or epistaxis. Septal hematoma requires drainage to prevent abscess formation and/ or cartilage destruction, which can result in severe nasal disfigurement. Open fractures of the nasal septum can sometimes be found on anterior rhinoscopy. The surgeon should also assess for watery rhinorrhoea which may be indicative of CSF leakage. Beta-2 transferrin testing can confirm the identity of the fluid. When unavailable, the halo test can sometimes be helpful: a drop of the fluid is placed on a gauze swab; blood coalesces in the center leaving a ring of CSF around the blood (Figure 12). If deemed necessary, nasendoscopy can also be performed to further examine for CSF leakage.
Examination of the oral cavity begins with assessment of occlusion. While all patients will not have Angle Class I occlusion, it is imperative to assess if the patient’s occlusion has changed since the accident. A gross dental exam is also helpful to determine if oral-maxillofacial surgery consultation is required. The maxilla should be grasped and assessed to determine stability. The oral cavity is then examined with attention to the buccal mucosa, Stensen’s duct, floor of mouth, tongue, palate, and maxillary/mandibular alveolar ridges. The oropharynx is then examined. If indicated, nasolaryngoscopy can be performed to examine the larynx. This is required if the patient presents with otherwise unexplained respiratory distress, voice changes, or crepitus.
The facial soft tissues are then carefully examined to rule out lacerations and abrasions. The underlying bony skeleton can be palpated to assess for step-offs.
The neck should then be examined. Palpation can reveal hematoma, crepitus, or displacement of the airway. Cervical spine status is essential to know prior to manipulating the patient’s head and/or neck.
Imaging

Figure 13: CT scan demonstrating zygomaticomaxillary fractures
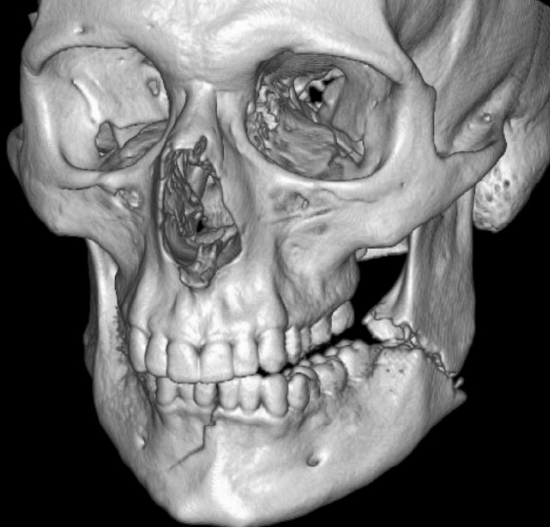
Figure 14: 3-D reconstruction demonstrates a fractured mandible

Figure 15: Panorex of fractured mandible
Imaging may be required to exclude injury to the brain, vasculature, and cervical spine and other associated injuries. Standard modern-day imaging for CMF skeleton includes fine cut, uncontrasted computed tomography (CT) of the CMF skeleton (Figure 13). It is often helpful to obtain coronal reformats and three-dimensional reconstructions (Figure 14). In the absence of CT imaging, reliance is placed on plain X-rays; panorex images are helpful with mandibular fractures (Figure 15). When available, the ideal imaging study of choice for maxillofacial trauma is noncontrast CT scan of the face with fine cuts, coronal and sagittal reformats, and 3D reconstructions.
Dental Occlusion
The most important consideration when reducing facial fractures involving or altering the occlusal surface is to ensure that premorbid dental occlusion is restored.
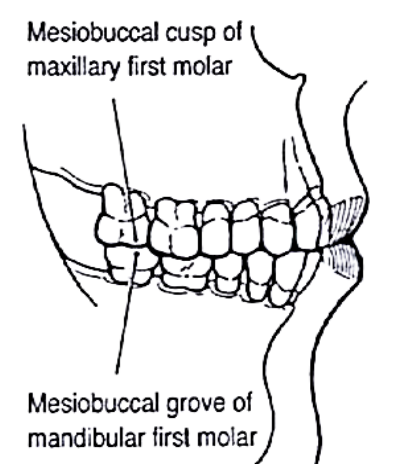
Figure 16: Class I Angles’ occlusion (Angle E. Treatment of malocclusion of the teeth. 7th ed. Philadelphia: SS White, 1907)
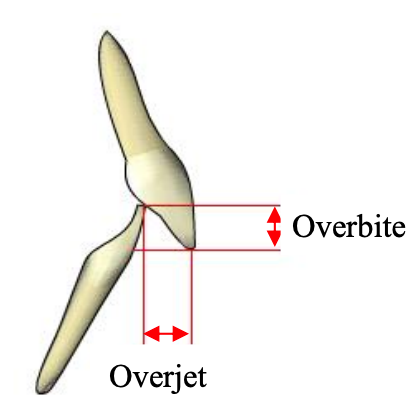
Figure 17: Incisal relationships - overbite and overjet
Angle class I occlusion is considered normal. It is defined as intercuspation of the mesial buccal cusp of the 1st maxillary molar with the buccal groove of the 1st mandibular molar (Figure 16). The maxillary incisors should extend slightly anteriorly past the mandibular incisors, known as overjet. The amount of overlap between the labial surface of the mandibular incisor and the lingual surface of the maxillary incisor is termed overbite (Figure 17).
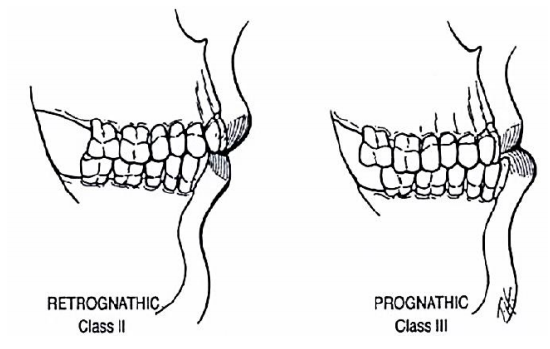
Figure 18: Angles’ classification of occlusion (Angle E. Treatment of malocclusion of the teeth. 7th ed. Philadelphia: SS White, 1907)
Angle class II (retrognathic) and Angle class III (prognathic) occlusions describe alternative relationships. Angle’s occlusal classification does not address anterior or transverse dental relationships (Figure 18).
One to 3 mm of overjet and overbite is considered normal; if excessive, it is considered to be a form of malocclusion. Transversely, the buccal cusps of the mandibular molars should lie between the buccal and lingual cusps of the maxillary molars (Figure 16).
Stepwise treatment of fractures
Treatment of facial fractures should not necessarily be tailored to achieve Class I occlusion; rather, the goal should be to restore premorbid occlusion. Premorbid occlusion is determined by assessing the positions of wear facets on the dentition intraoperatively.
Reduction and MMF

Figure 19: Wiring archbars together
Prior to fixation of fracture sites, appropriate reduction is achieved and the patient is placed into mandibulomaxillary fixation (MMF) using arch bars, bone supported devices or with direct interdental wiring techniques11 (Figure 19). For a detailed description of arch bar placement, readers are referred to the cited URL4.
Arch bars can often be removed if adequate fixation has been achieved with plating. However, if arch bars have been used as a tension band, they should remain in place for 6 weeks.
Exposing fractures
Once the patient has been placed into MMF (if required), the fracture sites are exposed. Several approaches are available to access the facial skeleton depending on the site and extent of the fractures. Lacerations overlying the fractures are utilized to access the underlying bone if possible.
Fractures of frontal bone and nasal root

Figure 20: Coronal incision
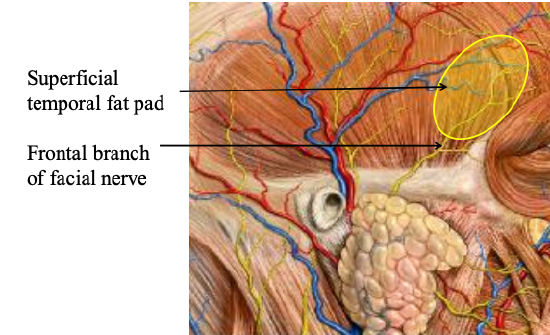
Figure 21: Anatomy of frontal branch of facial nerve
These can be addressed using a coronal incision (Figure 20). The incision extends from just superior to the root of the helix and is carried across the parietal bone keeping behind the hairline of the scalp, ending just superior to the contralateral helical root. Medially the incision may be extended to the pericranium if a pericranial flap is planned, or onto the cranium; laterally the dissection is typically kept in a plane just deep to the temporoparietal fascia with special care taken when approaching the zygoma to avoid the frontal branch of the facial nerve which resides in this plane (Figure 21).
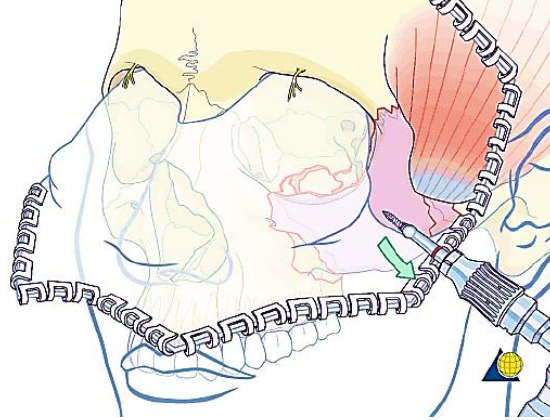
Figure 22: Coronal flap has been raised anteriorly to expose the frontal bone, root of the nose and lateral orbital rim (AO Foundation)
Figure 22 illustrates the coronal flap reflected anteriorly, taking care to preserve the supraorbital nerves if possible.
Fractures of lateral orbital rim and frontozygomatic suture
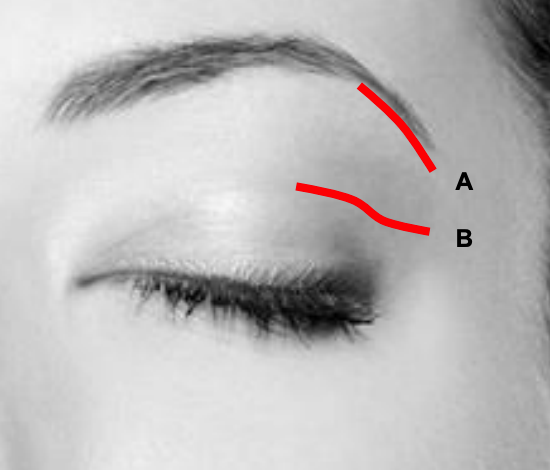
Figure 23: Lateral brow (A) and lateral lid crease incisions (B)
Access to the lateral orbital rim and frontozygomatic suture can be achieved by lateral brow or lateral lid crease incisions (Figure 23). Oftentimes isolated fractures of this region can be fixed using a miniplate with at least 2 screws on each side of the fracture line.
The lateral brow approach provides direct access to the superolateral orbital rim. No neurovascular structures are at risk. Scarring is generally concealed if the incision is placed within the hairs of the brow although it can cause alopecia if not carefully placed. It is used for fractures high up on the lateral orbital rim.
- Protect the cornea with a temporary tarsorrhaphy or a corneal cover shield
- Inject local anasthetic/vasoconstrictor into the skin and subcutaneous tissue
- Moisten and part the hair of the lateral eyebrow to open a linear gap for the incision
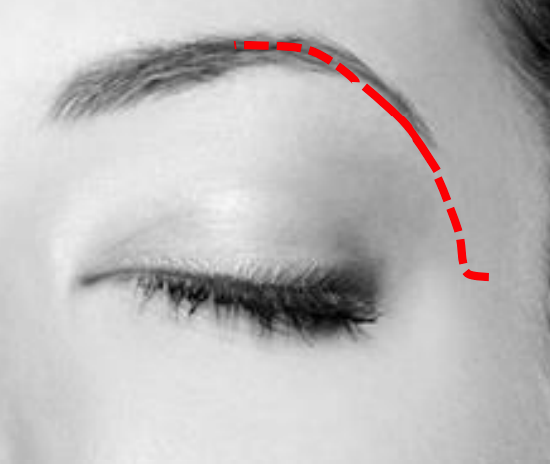
Figure 24: Lateral brow incision with medial and lateral extension for additional exposure
- Make a 2 cm incision within the confines of the lateral eyebrow through skin, subcutaneous fat and muscle (Figure 24)
- Cut parallel to the hair follicles to avoid injuring the hair follicles
- For additional exposure extend the incision medially within the eyebrow towards the supraorbital foramen and nerve; or inferiorly along the orbital rim by way of a small angled skin-only extension into a skin crease laterally, at least 6-7 mm above the lateral canthus (Figure 24)
- Undermine the orbicularis oculi muscle to expose the periosteum
- Dissect in an extraperiosteal dissection plane to expose the frontozygomatic suture line and fracture area
- Incise the periosteum with a scalpel along the superolateral orbital rim
- First expose the medial aspect of the superolateral orbital rim to gain access to the fossa containing the lacrimal gland
- Carry the subperiosteal dissection from this bony concavity inside the anterolateral portion of the orbital roof over the superolateral orbital rim. Widely undermining skin and periosteum facilitates exposure of the inferior lateral orbital rim
- Close the wound in three layers i.e. periosteum, muscle, and skin.
The lateral lid crease approach provides direct access to the lateral orbital rim (Figure 23).
- Protect the cornea with a temporary tarsorrhaphy or a corneal cover shield
- Inject local anesthetic/vasoconstrictor into the skin and subcutaneous tissue
- Incise the skin in the lateral half of the upper eyelid in a natural supratarsal skin crease. It is a curvilinear incision with the medial portion curved convexly superiorly and the lateral portion kept in line with the lateral canthus
- If a lid fold is not apparent, then place the incision 10 mm above the lash line in the centre of the lid and 6-7 mm above the lateral canthus
- The incision may be extended laterally onto the lateral orbital rim, and then curved superiorly for improved access
- Make a small slit at the lateral end of the wound and introduce scissors into the preseptal plane and dissect medially underneath the orbicularis oculi muscle
- Divide the orbicularis oculi leaving the orbital septum intact
- Elevate the skin/muscle flap with scissors from medial-to-lateral until the periosteum is exposed at the superolateral orbital rim
- Use an elevator to reflect the periosteum from the inside of the anterolateral orbital roof, and then from the lateral and posterior surface of the superolateral orbital rim
- The lacrimal gland may herniate if the periosteum is breached
- Incise the periosteum along the superolateral orbital rim
- Close the wound in three layers i.e. periosteum, muscle, and skin
Fractures of the inferior orbital rim and orbital floor
The inferior orbital rim and orbital floor can be accessed via a preseptal transconjunctival approach12; visualization can be augmented with endoscopy13. Alternatively, a transcutaneous approach can also be made via subciliary, subtarsal, or infraorbital incisions.
The preseptal transconjunctival approach provides access to the orbital floor and rim. This approach may be combined with lateral canthotomy and cantholysis for extended access to the lateral orbit.
- Protect the cornea with a temporary tarsorrhaphy or a corneal cover shield
- Make an incision through the palpebral conjunctiva and lower lid retractors immediately inferior to the lower border of the tarsal plate
- Dissect the posterior lamella away from the anterior lamella in the plane between the preseptal orbicularis oculi and the orbital septum
- This provides excellent access to the orbital rim
- Once the orbital rim is reached, the periosteum is sharply incised, revealing the underlying rim and providing access to the orbital floor
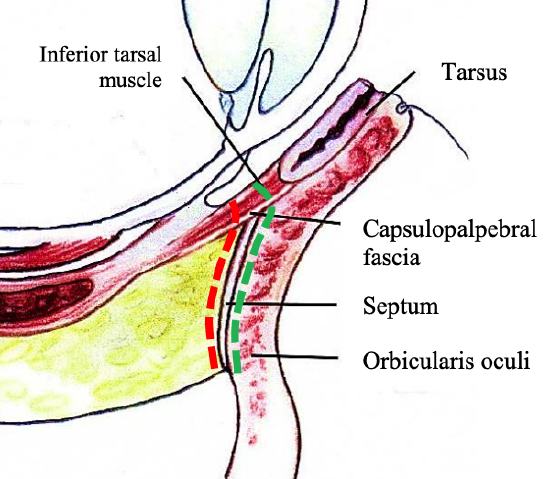
Figure 25: Preseptal (green) & retroseptal (red) routes
- Both the preseptal and retroseptal routes are shown in Figure 25; the authors prefer the preseptal route
Transcutaneous subciliary, subtarsal, or infraorbital incisions (Figure 26)
- Use existing lacerations in the lower eyelid if present to access the orbit
- Otherwise, incisions can often be made in existing relaxed-skin tension lines (RSTL)
- Even if not made in an RSTL, incisions in the lower eyelid are generally quite well hidden. In the diagram below, the following incisions are marked: A-subciliary, B-subtarsal, C-infraorbital, Dextended subciliary. These approaches differ only in the position of the skin incisions
- The plane of the approach to the orbital rim is otherwise similar
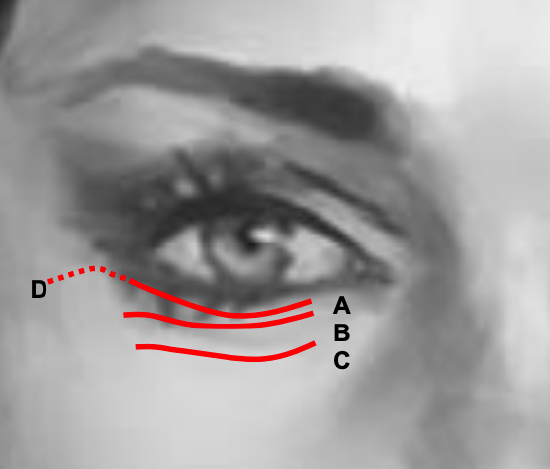
Figure 26: Transcutaneous subciliary (A), subtarsal (B), infraorbital (C), extended subciliary (D) incisions
- Subciliary incision (Figure 26)
- Carry the incision through skin to the pretarsal orbicularis oculi
- Develop the plane between the orbicularis oculi and subcutaneous tissue until the inferior border of the tarsal plate is reached
- Penetrate the orbicularis oculi
- Develop the plane between the orbicularis oculi and septum to reach the orbital rim
- Subtarsal incision (Figure 26)
- Make the skin incision inferior to the edge of the tarsal plate
- Carry the incision through the orbicularis oculi muscle
- Develop the plane between orbicularis oculi and orbital septum
- Infraorbital incision (Figure 26)
- The infraorbital incision is located directly superficial to the orbital rim
- Carry the incision through skin, orbicularis oculi, and periosteum of the orbital rim to gain direct access to the rim
Fractures of the medial orbital wall
The medial orbit can be accessed using a preseptal precaruncular transconjunctival approach 14. Dissection deep to periorbita may be facilitated by using a Freer’s suction elevator. Recent developments in multiportal endoscopic approaches to the skull base have also been reported15, 16.
Fractures of maxilla and lower midface
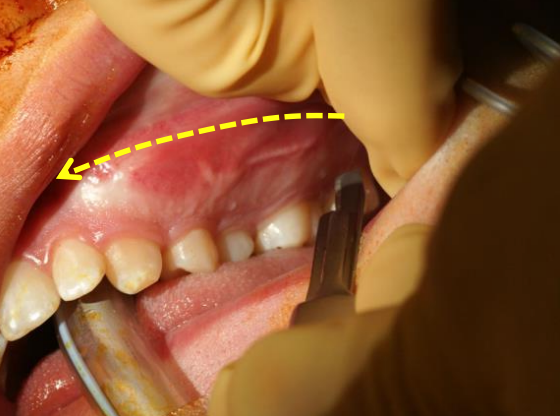
Figure 27: Sublabial approach to face of maxilla
The maxilla and lower midface can be exposed via a sublabial incision positioned approximately 1 cm from the labial sulcus to facilitate closure (Figure 27).
- Incise the sublabial mucosa with a #15 scalpel blade or monopolar electrocautery
- Use electrocautery to incise the soft tissue overlying the maxilla until the bone is reached
- Use a periosteal elevator to dissect over the face of the maxilla in a subperiosteal plane to identify the fractures
- Take care to avoid applying excessive pressure to the fragile anterior maxillary sinus wall, particularly if there is a fracture in this location

Figure 28: Maxilla with infraorbital foramen
- The infraorbital nerve is at risk during this dissection and should be preserved if possible (Figure 28)
Nasoethmoid/Orbital Fractures
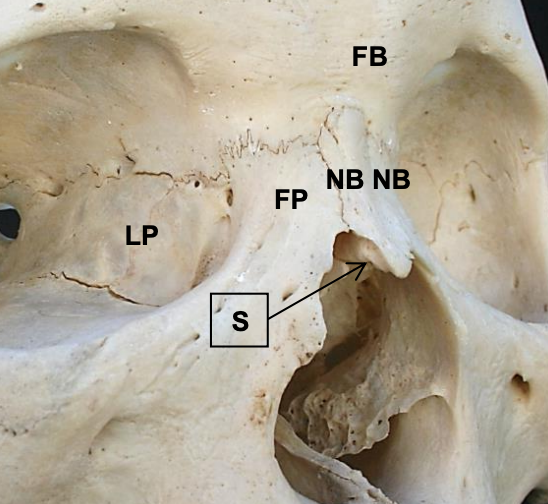
Figure 29: View of external nose: lamina papyracea (LP); nasal bones (NB); frontal bone (FB); frontal process of maxilla, bony septum (S)
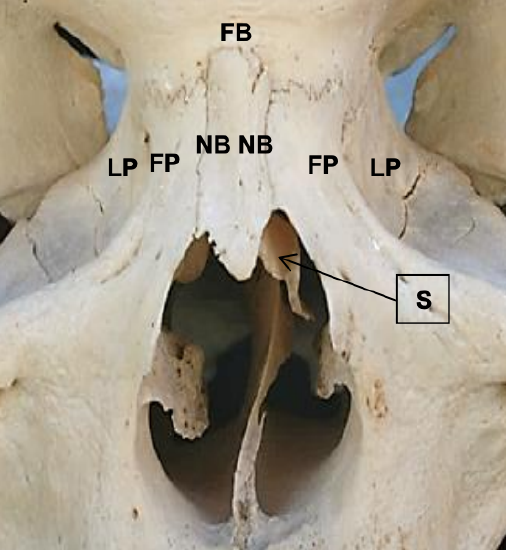
Figure 30: Anterior view of external nose: lamina papyraceae (LP); nasal bones (NB); frontal bone (FB); frontal process of maxilla (FP), bony septum (S)
Naso-orbital-ethmoid (NOE) complex fractures generally result from high-energy impact to the glabella or nasal root. Because the lamina papyraceae of the medial orbital walls are extremely thin (Figures 29, 30), these often fracture, resulting in posterior displacement of the nasal root. This presents a challenge because the fractures can involve the frontal sinus outflow pathways causing sinonasal dysfunction, or cerebrospinal fluid leaks.
NOE fractures are often best visualized with axial CT scans; both bony and soft tissue windows should be reviewed, particularly in the orbital region. Coronal images are helpful to delineate the floor of the anterior cranial fossa.
Surgical access may be technically challenging; accurate reduction and fixation are even more demanding. Fixation of these fractures can be achieved using microplate systems (1.0-1.3 mm with 2-3 mm screws). Fractures of the orbital floor are can be repaired using bone grafts, titanium mesh, porous polyethylene (PPE) sheets, composite PPE and titanium mesh, or resorbable materials.
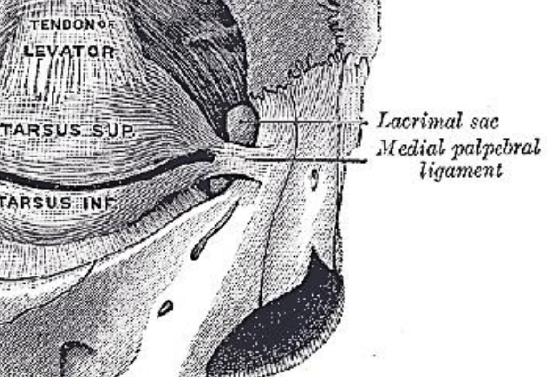
Figure 31: Medial canthal ligament
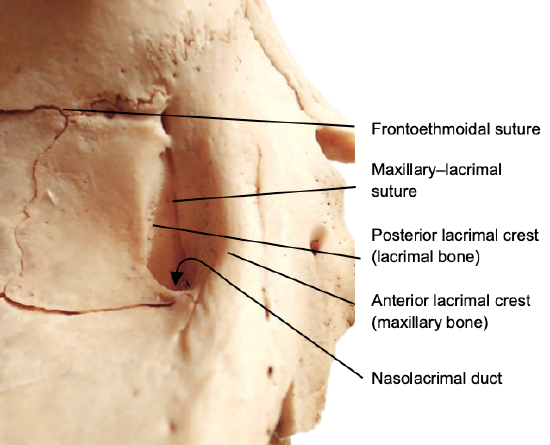
Figure 32: Anterior and posterior lacrimal crests are formed by the maxillary and lacrimal bones
The medial canthal ligaments represent the medial extensions of the orbicularis oculi muscles and are of importance in the management of NOE fractures (Figure 31).
The ligaments split into two primary components prior to their attachments to the anterior and posterior lacrimal crests, with some superior extensions as well (Figure 32). Fractures can displace the medial canthal ligaments resulting in malposition of the globe e.g. telecanthus.
The initial examination of the patient with an orbital wall fracture should include a thorough ophthalmologic examination with particular attention to extraocular muscle function and visual acuity. If either of these is compromised one should consult an ophthalmologist.
Orbital blowout fractures with herniation of orbital soft tissue into the maxillary or ethmoid sinuses and result in decreased orbital volume (enophthalmos) or diplopia due to entrapment of extraocular muscles causing limitation of ocular movements. Diplopia is a common consequence of orbital blowout fractures.
Entrapment of extraocular muscles requires immediate surgical intervention. Delay in reconstituting the periorbita and the entrapped muscle can result in fibrosis of the tissues and permanent diplopia. If a blowout defect is large enough to permit substantial herniation of tissue, hypoglobus and/or enophthalmos can result. In such defects, it is uncommon to have entrapment of extraocular muscles.
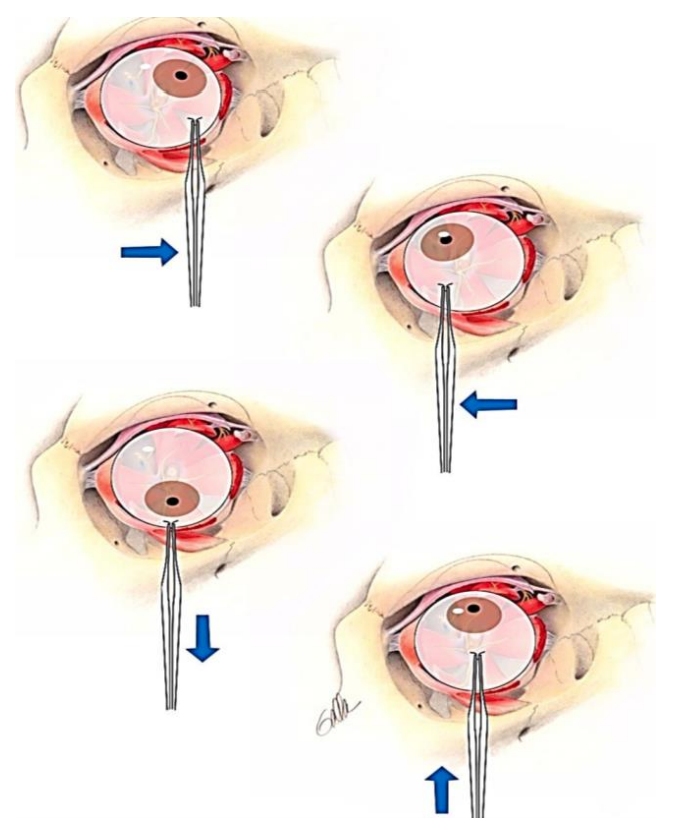
Figure 33: Forced duction testing
In a patient unable to cooperate with the physical examination, forced duction or traction testing (Figure 33) can be used to determine the presence of mechanical restriction of ocular motility.
The bulbar conjunctiva is anesthetized topically, and the conjunctiva is grasped near the limbus with toothed forceps. The globe is then moved into the direction in which the mechanical restriction is suspected.
Fractures of the orbital apex or optic canal are not common. In cases of traumatic optic neuropathy, magnetic resonance imaging (MRI) should be employed prior to decompression. (See chapter: Endoscopic transnasal optic nerve decompression)
Isolated Nasal Fractures
More than 1/3 of facial fractures affect the nasal complex17. Examine the external nose and nasal cavity thoroughly. Nasal fractures can be present without causing nasal deformity or airway obstruction.
Epistaxis can be controlled in several ways. Initial management may involve pinching the cartilaginous nasal walls against the nasal septum for 15 minutes. If this fails, then the nose is suctioned and oxymetazoline is sprayed into the nose for vasoconstriction and the cartilaginous nose is again pinched for 15 minutes. If this fails, one may elect to insert absorbable or non-absorbable packing in the nasal cavities. Absorbable nasal packing is preferred because it avoids traumatizing the fragile nasal mucosa.
It is important to perform an endonasal examination to rule out a septal hematoma as it must be evacuated to prevent a septal abscess or septal necrosis18. Drainage is performed by incising the septal mucoperichondrium. Silastic splints are placed endonasally to oppose the mucoperichondrial flaps against the septal cartilage.

Figure 34: Undisplaced nasal fracture that can simply be observed
Nasal fractures are reduced only if the patient has aesthetic or functional complaints. It is the authors’ opinion that radiographic examination is unnecessary in clinically undisplaced nasal fractures (Figure 34). Such patients are simply reminded to avoid contact sports while the nasal bones heal.
Because initial soft tissue swelling may mask a displaced bony fracture, it is prudent to re-examine such a patient once the soft tissue swelling has subsided. Timely reduction of fractures is important as delays make manipulation of fractured bone fragments very challenging and may lead to malunion. Although it may be possible to achieve a closed reduction up to 3 weeks after injury, it is preferable to perform the reduction within 10-14 days.

Figure 35: Asch septum-straightening forceps and Boies nasal fracture elevator
Reduction of nasal fractures can often be accomplished via a closed approach. This is typically be performed under local anasthesia and insertion of nasal pledgets soaked in vasoconstrictor e.g. oxymetazoline or cocaine. An Asch septum-straightening forceps or Boies nasal fracture elevator is used to reduce the fracture (Figure 35). The Boies elevator is inserted endonasally on the depressed side first with the dominant hand and the surgeon’s nondominant hand is placed on the nose for stability. The fracture is then reduced into place. The same process is performed on the contralateral side to reduce the fractured fragment. Adhesive strips and a splint are placed over the nasal dorsum and are removed after 5-10 days. In patients with extensive fractures, open septal fractures, or persistent deformities following closed reduction, open reduction can be considered.
Le Fort Fractures (Figure 36)
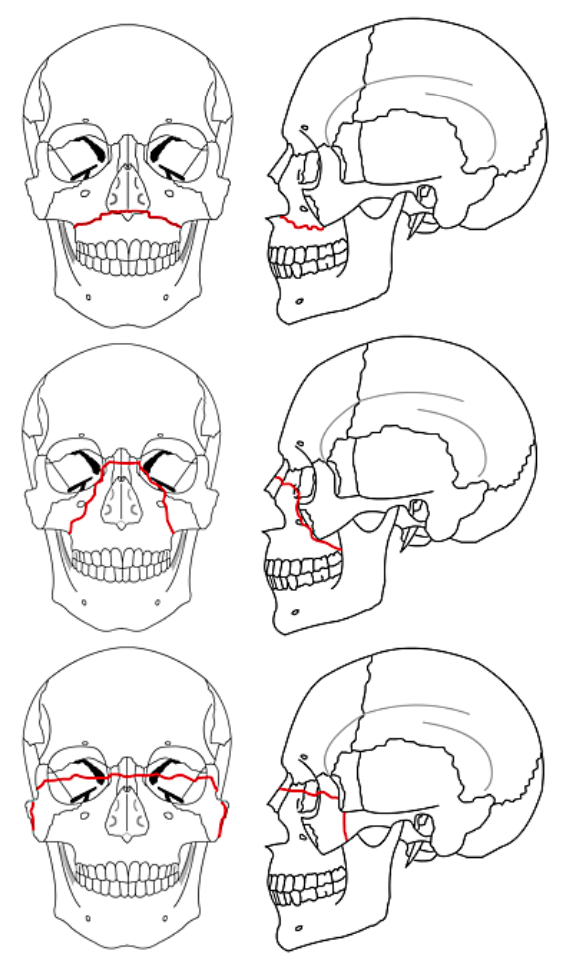
Figure 36: Le Fort I (Top); Le Fort II (Center); Le Fort III (Bottom) (Wikipedia)
Le Fort fractures typically occur in conjunction with other midface fractures. If only one side of the face is involved, it is termed a “hemi” Le Fort fracture. Le Fort I fractures traverse the maxillary alveolus through the pyriform sinus and may involve the pterygoid plates. Le Fort II fractures extend from the maxilla into the orbit in a pyramidal configuration. Le Fort III fractures are complete craniofacial dissociation.
Although these fracture patterns are useful descriptors to communicate between providers, craniomaxillofacial surgeons should describe each fracture in detail on each side of the face, also including fractures of the frontal bone and mandible. Miniplate systems (1.5-2.0 mm with 4-6 mm screws) are ideal for fixation of lower midface fractures.
Zygomaticomaxillary complex fractures

Figure 37: Fracture of zygomaticomaxillary complex with impingement of coronoid process of mandible
Zygomaticomaxillary complex fractures involve the zygomatic arch, in addition to disruption of its articulations with the frontal, sphenoid, maxillary and temporal bones. Axial CT scans readily identify such fractures (Figure 37).
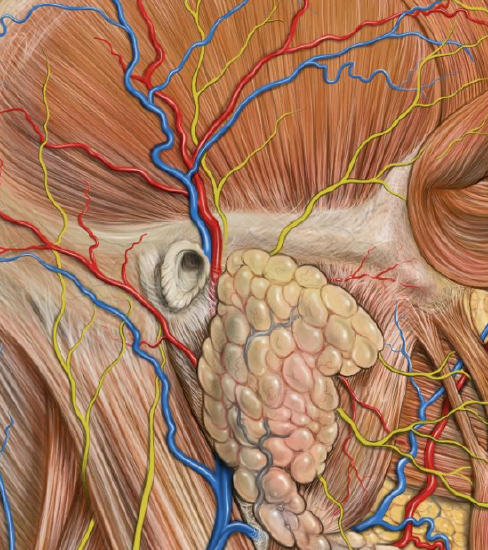
Figure 38: Frontal branch of facial nerve
These fractures are reduced using approaches highlighted earlier. Plating can be challenging in this region because of the proximity of the frontal branch of the facial nerve to the zygoma (Figure 38).
Mandible fractures
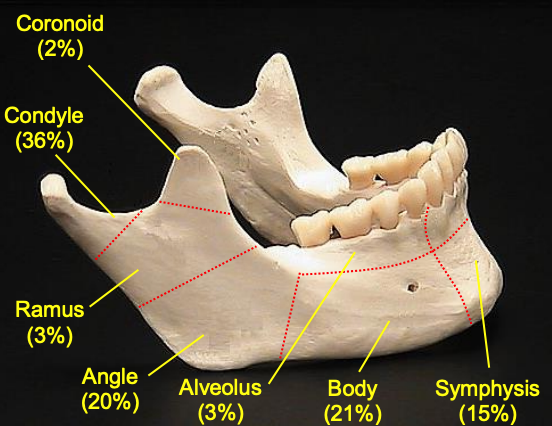
Figure 39: Mandible fracture frequencies. (From Cheney ML. Facial Surgery 1st Ed)
Mandibular fractures are the second most prevalent type of facial fracture19 and most commonly involve the condylar region, followed by the body and angle (Figure 39).
Fractures can be described as greenstick, simple, or compound. Greenstick fractures entail injury to only one surface of the bone and are common in the pediatric population because of the flexibility of the young skeleton. A simple fracture is a fracture not involving the intraoral mucosa. Compound fractures, also known as open fractures, involve exposure of bone by violations of soft tissue. Comminuted fractures have multiple fragments of bone disassociated from one another.
Open reduction and internal fixation of mandible fractures can be straightforward as with parasymphyseal fractures, or very challenging as in subcondylar fractures. Consequently, complication rates following mandible fracture repair are significant. A recent series of >500 mandible fractures revealed an overall complication rate of 26% with hardware failure being the most common20. The authors found that antibiotic use did not decrease infection rates, but that patients with systemic medical conditions and smokers had higher risks of postoperative complications.
Substantial variations exist in treatment of mandibular fractures around the globe. Otolaryngologists, plastic surgeons, and oromaxillofacial surgeons all operate on the mandible and come from different training backgrounds, which likely accounts for some of the variations in treatment. Nonetheless there are several aspects of treatment that ought to be practiced universally.
The 1st step is to determine if the patient’s dentition is adequate for placement of maxillo-mandibular fixation (MMF). In the edentulous patient, open reduction and internal fixation (ORIF) is necessary for repair of displaced mandible fractures, whereas in the dentate mandible, if teeth are present on both the mesial and distal aspects of the fracture line, ORIF or closed reduction are both reasonable options.
Closed reduction is an option for non- or minimally-displaced simple fractures that can undergo MMF. A comorbid condition that may preclude ORIF e.g. a medically unstable patient, is also an indication for closed reduction. Closed reduction is accomplished with placement of arch bars and the application of dental wiring to achieve MMF. The MMF is released 6 weeks later and fracture stability is assessed. If the patient remains in occlusion, then he/she should be placed on a soft diet and arch bars should be removed 2 weeks later. Postoperative panorex examination can be helpful to assess bony alignment and occlusion.
Mandibular symphysis, parasymphysis, and body
- Expose the fractures via a transoral incisions.
- Typically, an incision is made in the sublabial mucosa of the lower lip approximately 1 cm from the labial sulcus
- Sharp dissection is continued through periosteum
- A periosteal elevator is used to expose the fracture sites
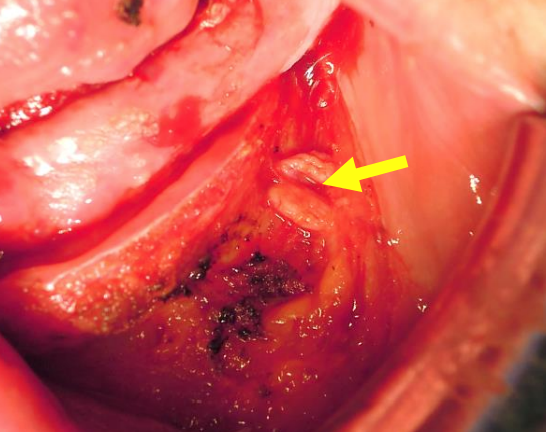
Figure 40: Mandible exposed via intraoral approach; note mental nerve exiting the left mental foramen
- The mental nerve is at risk during this dissection as it exits the mandible between the 1st and 2nd premolar teeth (Figure 40)
- Blunt dissection can be used to free the nerve from surrounding soft tissue; this permits greater exposure of the labial surface of the mandible
- Open reduction and internal fixation of symphyseal and parasymphyseal fractures can be accomplished using lag screws, a lag screw and plate, plate and arch bar, or two plates
- Fractures medial to the mental foramina can be treated using placement of two lag screws
- A lag screw with plate should be used when placement of only one lag screw is possible
- These fractures can also be stabilized using two miniplates - one at the superior border of the mandible inferior to the tooth roots, and one at the inferior border of the mandible. Two screws should be present on either side of the fracture
- Complex anterior fractures often require placement of a load-bearing reconstruction plate
- Simple fractures of the mandibular body in patients who are not candidates for ORIF can sometimes be treated with closed reduction, although ORIF is preferred, and can be achieved using lag screws, one Champy plate (in certain circumstances), two plates, or one large reconstruction plate (in special circumstances).
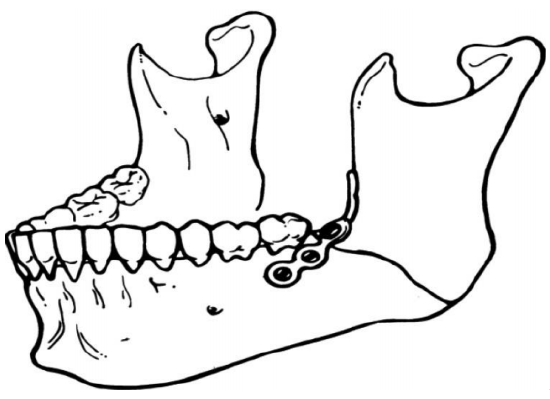
Figure 41: Champy plate21
Complex body fractures often require two plates or a reconstruction plate with at least three or four screws on each side of comminution. Wire fixation is possible in some cases of simple angle and ramus fractures when augmented with 6 weeks of postoperative MMF if plates are unavailable.
Severely comminuted mandible fractures
This requires reduction of multiple small fragments and is often best managed via a transcutaneous approach.
- Typically make a skin incision in a skin crease approximately 2 cm below the inferior margin of the mandible.
- Dissect through the platysma.
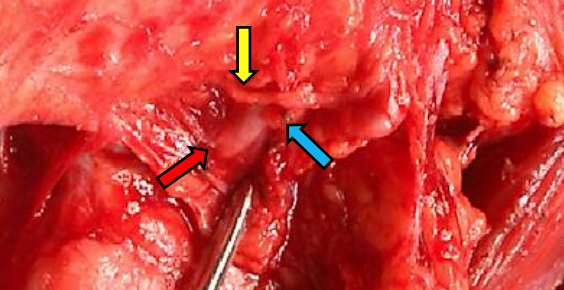
Figure 42: Transcutaneous exposure of left mandible with marginal mandibular nerve (yellow arrow) crossing facial artery (red arrow) and ligated vein (blue arrow)
- Incise and reflect the fascia overlying the submandibular gland superiorly to protect the marginal mandibular branch of the facial nerve (Figure 42)
- Identify and ligate and divide the facial artery and vein if necessary (Figure 42)
- Incise the mandibular periosteum to expose the fracture site
Mandibular ramus or subcondylar fractures
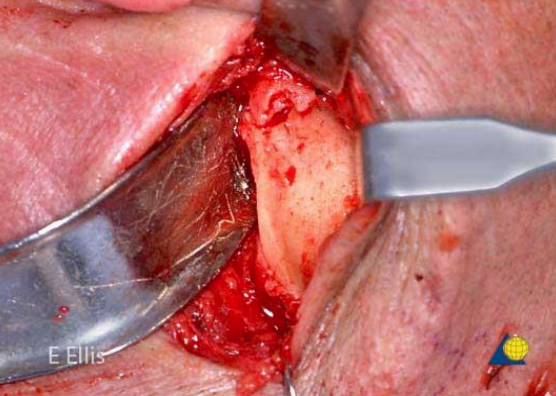
Figure 43: Retromandibular approach (left)
These can be accessed via retromandibular (rhytidectomy) approaches (Figure 43). While it permits excellent access to the posterior mandible, it does carry a great risk of damage to the facial nerve. Even slight traction on the facial nerve can cause postoperative dysfunction which can be disturbing for patients. For this reason, endoscopic approaches to the subcondylar region, although technically challenging, are also be used.
Condylar process and condylar head fractures Treatment can be complex, and can entail observation, closed reduction, or ORIF based on the extent of injury5.
Useful Resource
AO Surgery: Guide to Maxillofacial Trauma: (Highly recommended)
References
- Lee K. Global Trends in Maxillofacial Fractures. Craniomaxillofacial trauma & reconstruction 2012;5:213-22
- Bisson JI, Shepherd JP, Dhutia M. Psychological sequelae of facial trauma. J Trauma 1997;43:496-500
- Manson PN. Facial bone healing and bone grafts. A review of clinical physiology. Clin Plast Surg 1994;21:331-48
- CMF. (Accessed December 17, 2013, at https://www2.aofoundation.org/wps/po...soloState=true
- Wilde F, Lorenz K, Ebner AK, et al. Intraoperative imaging with a 3D C-arm system after zygomatico-orbital complex fracture reduction. J Oral Maxillofac Surg 2013;71:894-910
- Hughes MS, Moghadamian ES, Yin LY, et al. Comparison of bulb syringe, pressurized pulsatile, and hydrosurgery debridement methods for removing bacteria from fracture implants. Orthopedics 2012;35: e1046-50
- Adalarasan S, Mohan A, Pasupathy S. Prophylactic antibiotics in maxillofacial fractures: a requisite? J Craniofac Surg 2010;21:1009-11
- Morris LM, Kellman RM. Are prophylactic antibiotics useful in the management of facial fractures? Laryn-goscope 2013
- Manson PN, Hoopes JE, Su CT. Structural pillars of the facial skeleton: an approach to the management of Le Fort fractures. Plast Reconstr Surg 1980;66:54- 62
- Cheney ML. Facial surgery: plastic and reconstructive. Baltimore: Williams & Wilkins; 1997
- Rai A, Datarkar A, Borle R, Rai M. Comparative assessment between eyelet wiring and direct interdental wiring for achieving intermaxillary fixation: a prospective randomized clinical study. J Oral Maxillofac Surg 2012;70:1914-7
- Santosh BS, Giraddi G. Transconjunc-tival preseptal approach for orbital floor and infraorbital rim fracture. J Maxillofac Oral Surg 2011;10:301-5
- Polligkeit J, Grimm M, Peters JP, et al. Assessment of indications and clinical outcome for the endoscopy-assisted combined subciliary/transantral approach in treatment of complex orbital floor fractures. J Craniomaxillofac Surg 2013;41:797-802
- Moe K. The precaruncular approach to the medial orbit. Arch Facial Plast Surg 2003;5:483-7
- Bly RA, Su D, Hannaford B, et al. Computer modeled multiportal approaches to the skull base. J Neurol Surg Part B, Skull base 2012; 73:415-23
- Lim JH, Sardesai MG, Ferreira M, Jr., Moe KS. Transorbital neuroendoscopic management of sinogenic complications involving the frontal sinus, orbit, and anterior cranial fossa. J Neurol Surg Part B, Skull base 2012;73:394-400
- Illum P, Kristensen S, Jorgensen K, et al. Role of fixation in the treatment of nasal fractures. Clin Otolaryngol Allied Sci 1983;8:191-5
- Landis BN, Borner U. Septal hematoma: always think about it! J Pediatrics 2013;163:1223
- Hwang K, You SH. Analysis of facial bone fractures: An 11-year study of 2,094 patients. Indian J Plast Surg: official publication of the Association of Plastic Surgeons of India 2010; 43:42-8
- Gutta R, Tracy K, Johnson C, et al. Out - comes of Mandible Fracture Treatment at an Academic Tertiary Hospital: A 5-Year Analysis. J Oral Maxillofac Surg 2014
- Singh RK, Pal US, Agrawal A, Singh G. Single miniplate osteosynthesis in angle fracture. Natl J Maxillofac Surg 2011;2: 47-50
Authors
Prabhat K. Bhama, M.D., M.P.H.
Staff Surgeon
Department of Otolaryngology
Alaska Native Tribal Health Consortium
Anchorage, Alaska, USA
pbhama@gmail.com
Mack L. Cheney, M.D.
Chair, Office of Global Surgery
Professor, Division of Facial Plastic and Reconstructive Surgery
Department of Otolaryngology
Harvard Medical School/Massachusetts Eye and Ear Infirmary
Boston, Massachusetts, USA
mack_cheney@meei.harvard.edu
Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za