
3.1: Frenolotomy and Frenulectomy for Ankyloglossia (Tongue Tie)
- Page ID
- 15440

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
FRENULOTOMY AND FRENULECTOMY FOR ANKYLOGLOSSIA (TONGUE TIE)
Ndivhuwo Diale, Shazia Peer, Jessica McGuire
Frenulotomy (also referred to as frenotomy) and frenulectomy (frenectomy) are surgical procedures used to correct ankyloglossia, a congenital condition in which the lingual frenulum is too short, causing restricted tongue movement. It is commonly called a tongue tie and it affects 4-11% of neonates1.
Frenulotomy refers to an incision in the frenulum that frees the tongue from the floor of the mouth. Frenulectomy refers to complete excision of the frenulum. It is more invasive and may be difficult to perform on small children; however, the results are more predictable, and the recurrence rate is lower.
Anatomy
The tongue is attached to the floor of the mouth by the lingual frenulum. The frenulum’s appearance varies considerably between individuals. Microdissection of cadavers shows that it is a dynamic, layered structure formed by oral mucosa and the underlying floor of mouth fascia, which is mobilized into a midline fold with tongue elevation and/or retraction2.
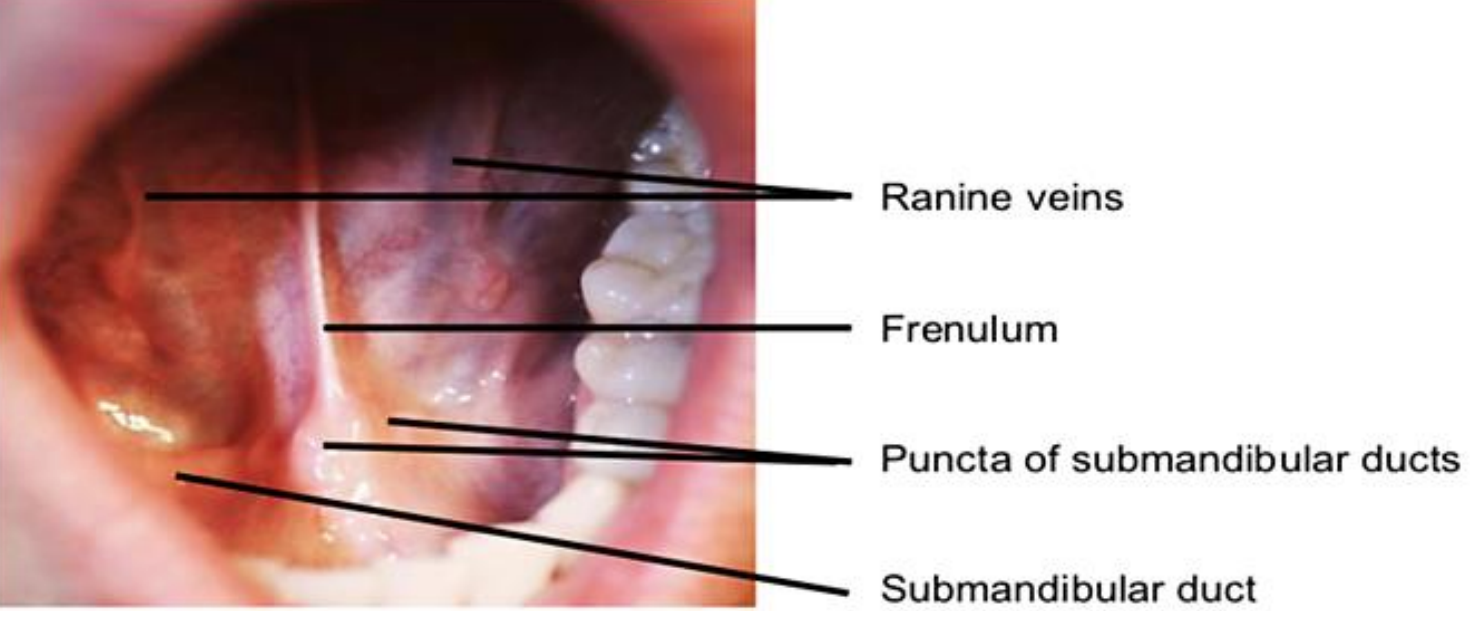
Figure 1: Floor of the mouth and ventral surface of the tongue
The base of the frenulum contains a "V" shaped hump of tissue in the floor of the mouth which houses the two Wharton’s ducts on either side. The sublingual salivary glands empty through tiny ducts on either side of Wharton's ducts. Superficial veins running through the base of the frenulum are known as ranine veins (Figure 1).
Classification of ankyloglossia (Table 1)
| Type 1 | Most extreme form, 100% of the tongue is attached to the lingual frenulum and is tethered to the floor of the mouth anteriorly | 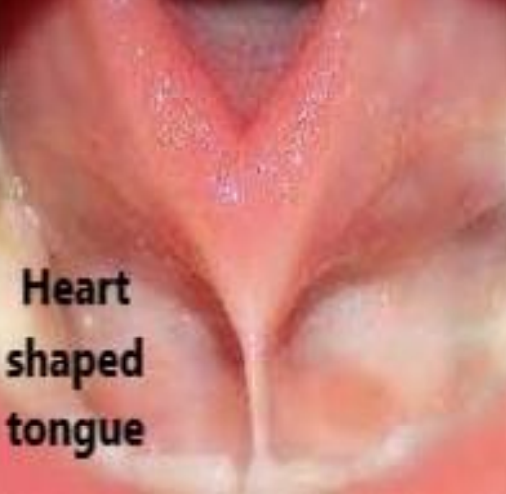 |
| Type 2 | 75% of the tongue is tethered with restricted elevation and extension of the tongue |  |
| Type 3 | 50% of the tongue is tethered. Tongue appears normal, but mobility is limited. |  |
| Type 4 | Limited tongue mobility due to a posterior, fibrous limitation of the most distal portion of the lingual frenulum |  |
Table 1: Modified grading system developed by Coryllos et al9. Type 2-4 images obtained from Yoon et al10
Currently, there are no established criteria or grading systems to classify ankyloglossia.
Several studies have suggested various guidelines based on the following criteria:
- Length of the frenulum3,4
- Upward tongue mobility (difficulty lifting the tongue to the upper dental alveolus)5,6
- Limited tongue protrusion ≤1–2 mm past the lower central incisors7
- Impaired lateral mobility of the tongue, ‘heart-shaped-tongue-appearance’ and thick fibrous cord palpated on physical examination8
The classification by Coryllos permits identification of type III and IV frenula, which can go unnoticed with macroscopic examination, by means of palpation (Table 1). For a diagnosis of ankyloglossia in neonates it is necessary to combine both functional and anatomical criteria.
Indications for surgery
There has been a surge in frenulotomies performed on neonates in recent years in an attempt to improve breastfeeding. A Cochrane review found that frenulotomy reduced mothers’ nipple pain and had for the most part, positive short-term effects on breastfeeding1.
Indications
- Difficulty feeding, poor latch in breastfeeding babies and poor weight gain
- Difficulty swallowing
- Decreased mobility of tongue
- Speech difficulties
- Significant dental problems
A frenulotomy is appropriate in patients with symptomatic type 2-4 ankyloglossia, provided that the frenulum is not fibrotic. Type 1 ankyloglossia, fibrotic frenula and revision cases would benefit from a frenulectomy.
In neonates and infants, it may be performed under local anesthesia in an outpatient setting. The author has performed this procedure in a 16-week infant. The optimum age to perform a frenulotomy in infants is unclear1 and the age limit to performing the procedure under local anesthesia is equally unclear. Consider a general anesthesia in babies much older than 16 weeks.
Frenulotomy
Surgical consent is obtained.
a. Outpatient Awake Procedure
Positioning
- The child is swaddled and restrained by an assistant
- The child is then placed flat with head in neutral position and mouth open
Local anesthesia
- Lignocaine HCl 1% m/v local anesthetic with adrenaline 1:160000 is injected on either side of the frenulum
- The dose limit is 7 mg/kg and each 1 mL contains 10 mg of lignocaine
- This is important to bear in mind for small infants
Procedure
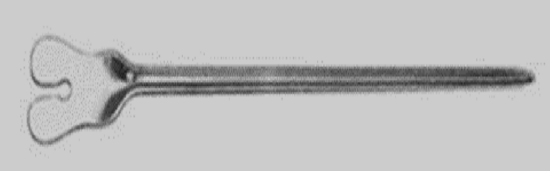
Figure 3: Example of a grooved retractor

Figure 4: Grooved retractor manufactured from a teaspoon

Figure 5: Grooved retractor tenting the frenulum
- A grooved retractor is used to retract the tongue (Figures 3,4,5)
- A straight Crile hemostat is used to crimp the frenulum prior to release
- Sterile curved scissors are then used to release the lingual frenulum at its attachment
- The incision should be close to the ventral surface of the tongue to avoid injury to the ductal orifices
- To ensure adequate release of the frenulum, using your finger, gently massage the tongue at the deep end of the cut frenulum.
- The floor of mouth is compressed with gauze to provide hemostasis, if necessary
In the awake child, sucking and oral 50% dextrose syrup may also be used to sooth the infant.
b. General Anesthesia
Intubation
- Intermittent mask ventilation or nasal intubation is preferable for adequate access
- Oral intubation may also be performed
Positioning
- Place the child in a supine position with head extended
- Open the mouth and use the grooved retractor to retract the tongue
Surgical steps

Figure 6: Hemostat clamped parallel to tongue

Figure 7: Middle finger retracting lower lip to avoid injuring it while lingual frenulum is released

Figure 8: Diamond-shaped wound following frenulotomy

Figure 9: In revision cases, or older children, interrupted absorbable sutures can be placed to prevent the release from adhesing back down onto the floor of mouth
- Inject or apply topical pledgets soaked with 1:80000 lignocaine with adrenaline to either side of frenulum
- Use the grooved retractor to retract the ventral tongue to fully expose the lingual frenulum (Figure 5)
- Clamp a straight Crile hemostat onto frenulum parallel to the tongue at its ventral surface (Figure 6)
- Wait a few seconds, and then release the hemostat
- Use sterile iris scissors to release the lingual frenulum at its attachment (Figures 6-8)
- Make the incision close to the ventral surface of the tongue to avoid the submandibular and sublingual salivary gland ducts which open onto the floor of the mouth
- To break down deeper fibrous bands, gentle finger / peanut dissection is recommended (encountered more often in thicker frenula and revision cases)
- The genioglossus muscle is the posterior limit of the frenulum incision
- Compress the floor of mouth with gauze to provide hemostasis
- In revision cases, or with older children, interrupted absorbable sutures can be placed to prevent the release from adhesing back down onto the floor of mouth. Take care near the papilla of the submandibular ducts (Figure 9)
Complications of surgery (rare)
- Bleeding
- Infection
- Swelling
- Discomfort
- Injury to Wharton’s duct
- Scarring requiring revision
Z-Frenuloplasty
This is recommended in older children and revision cases to improve speech.
Surgical Steps
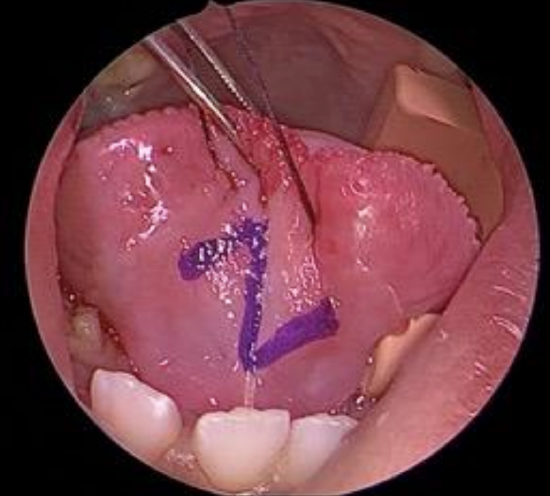
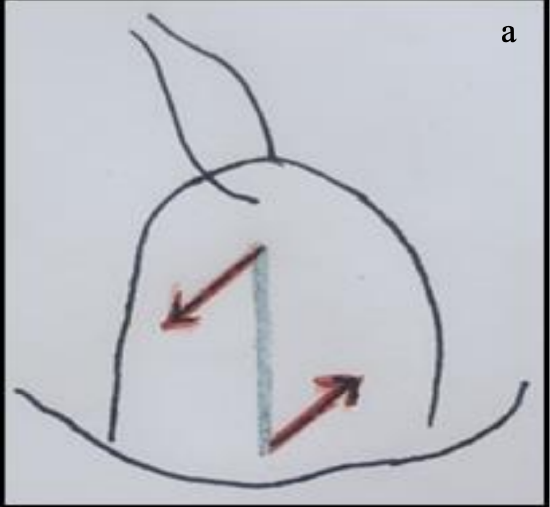
Figure 10: Incisions outlined

Figure 11: Vertical incision along frenulum
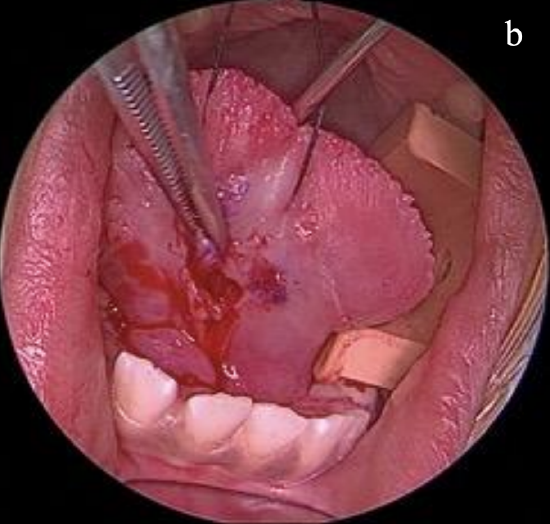
Figures 12a, b: Two incisions at 900 to vertical incision
Figures 13a, b: Two flaps are elevated

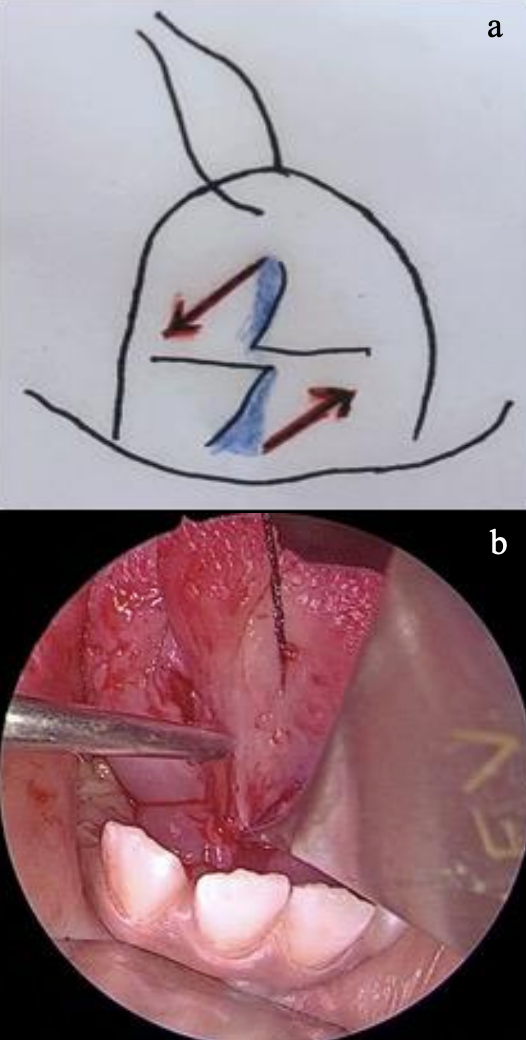
Figure 14: Transpose the 2 flaps adjacent to each other to close in the form of a Z-plasty
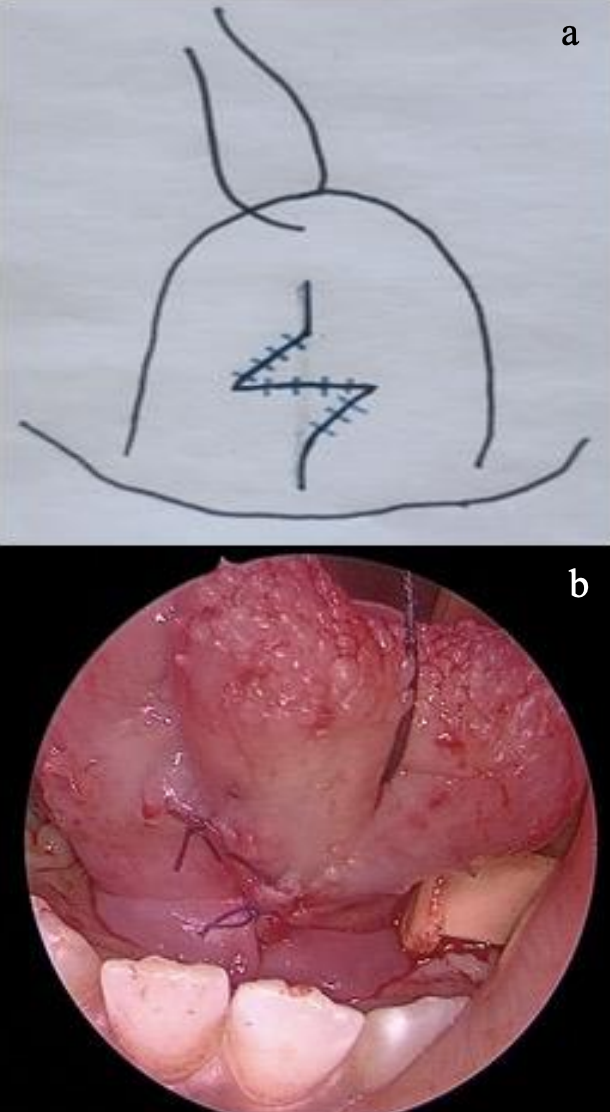
Figures 15a, b: Sutures flaps to complete the Z-plasty
- Place a silk stitch through the tongue tip to retract the tongue and hold it in place (Figure 10)
- Apply lignocaine with adrenaline injection of 1:80 000 or topical pledgets to either side of frenulum
- Draw the Z-plasty incisions (Figure 10)
- Make a vertical/longitudinal incision along the length of the frenulum (Figure 11)
- Make 2 incisions at 900 to the first vertical one (Figures 12a, b)
- Two rectangular flaps are now created and elevated (Figures 13a, b)
- Transpose the 2 flaps adjacent to each other to close in the form of a Z-plasty (Figure 14)
- Suture with interrupted 5.0 vicryl (Figures 15a, b)
References
- O'Shea JE, Foster JP, O'Donnell CP, Breathnach D, Jacobs SE, Todd DA, Davis PG. Frenotomy for tongue-tie in newborn infants. Cochrane Database of Systematic Reviews. 2017(3)
- Messner AH, Lalakea ML, Aby J, Macmahon J, Bair E. Ankyloglossia: incidence and associated feeding difficulties, Arch Otolaryngol Head Neck Surg. 126 (2000) 36–9
- Kotlow LA, Ankyloglossia (tonguetie): a diagnostic and treatment quandary, Quintessence Int. 30 (1999) 259–62
- Marmet C, Shell E, Marmet R, Neonatal frenotomy may be necessary to correct breastfeeding problems, J Hum Lact. 6 (1990) 117–21
- Hogan M, Westcott C, Griffiths M, Randomized, controlled trial of division of tongue-tie in infants with feeding problems, J Paediatr Child Health. 41 (2005) 246–50
- Masaitis NS, Kaempf JW. Developing a frenotomy policy at one medical center: a case study approach. J. Hum. Lact. 12 (1996) 229–32
- Chu MW, Bloom DC. Posterior ankyloglossia: a case report, Int J Pediatr Otorhinolaryngol. 73 (2009) 881–3
- Harris EF, Friend GW, Tolley EA. Enhanced prevalence of ankyloglossia with maternal cocaine use, Cleft Palate Craniofac J. 29 (1992) 72–6
- Coryllos E, Genna CW, Salloum AC. Congenital tongue-tie and its impact on breastfeeding. AAP section on breastfeeding. 2004; Vol. Summer http://www.aap.org/breastfeeding/files/pdf/BBM‐8‐27%20Newsletter.pdf
- Yoon AJ, Zaghi S, Ha S, Law CS, Guilleminault C, Liu SY. Ankyloglossia as a risk factor for maxillary hypoplasia and soft palate elongation: A functional–morphological study. Orthodontics & craniofacial research. 2017 Nov;20(4):237-44
Authors
Ndivhuwo Diale MBChB, MMed, FCORL
Otolaryngologist
Sefako Makgatho Health Sciences
University, Gauteng Province, South Africa
ndivhuwobele@yahoo.com
Shazia Peer MBChB, MMed, FCORL
A-Professor, Pediatric Otolaryngologist
Red Cross War Memorial Children’s Hospital, Cape Town, South Africa
shazia.peer@uct.ac.za
Jessica McGuire MBChB, MMed, FCORL
Pediatric Otolaryngology
Red Cross War Memorial Children’s Hospital, Cape Town, South Africa
jkmcguire2@gmail.com
Pediatric Section Editor
Nico Jonas MBChB, FCORL, MMed
Pediatric Otolaryngologist
Addenbrooke’s Hospital Cambridge, United Kingdom
nicojonas@gmail.com
Author and Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za