
4.1: Endoscopic Transorbital Surgery - Medial Orbital (Precaruncular) Approach
- Page ID
- 15447

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
ENDOSCOPIC TRANSORBITAL SURGERY: MEDIAL ORBITAL (PRECARUNCULAR) APPROACH
Darlene Lubbe
The precaruncular approach is indicated for the following clinical situations:
- Ligation of anterior and posterior ethmoidal arteries
- Multiportal surgery for optic nerve decompression. The precaruncular portal is especially useful to retract herniating fat and muscle laterally to allow for both posterior orbital and optic nerve decompression
- Minimally invasive surgery for removal of medial orbital lesions – cavernous hemangiomas, pseudotumors and to biopsy medially located lesions
- Access to lacrimal sac
- To address blow-out fractures of the medial orbit and to reconstruct the medial orbital wall
- Access to lateral aspect of ipsilateral sphenoid sinus
- Access to contralateral sphenoid sinus for Sternberg canal defects
- Access to medial cavernous sinus
- Access to ipsilateral anterior cranial fossa / cribriform area / olfactory fossa
- Drainage of medially located subperiosteal abscesses secondary to complicated sinusitis
Precaruncular approach compared to Lynch-Howarth incision
Access to the ethmoidal arteries is required to ligate the vessels with nasoethmoid traumatic fractures or to assist with hemostasis prior to resection of the sinonasal tumors. The Lynch-Howarth incision has been the gold standard to approach these arteries, with the frontoethmoidal suture line said to be the optimal way of finding these arteries. However, this external approach should be replaced by the precaruncular approach to access these arteries for the following reasons:
Lynch-Howarth incision
- External facial incision that can cause cosmetically unacceptable scars
- Dissection through skin, subcutaneous tissue, orbicularis oculi muscle is required with suturing of the incision
- Bleeding can be encountered from the angular vessels
Precaruncular approach
- Provides access to
- Ethmoidal arteries
- Medial orbit
- Lamina papyracea
- Ethmoid and sphenoid sinuses
- Optic nerve
- Medial cavernous sinus
- Direct access without breaching facial skin
- Easy, quick, direct access without dissecting uninvolved tissue (skin, muscle, lacrimal system, sinuses)
- No suturing of skin incision required
Surgical Anatomy
It is important to understand the anatomy of the medial canthus, lacrimal system and the attachments of the medial orbital wall structures to the bony orbit prior to utilizing this medial portal.
Medial canthus
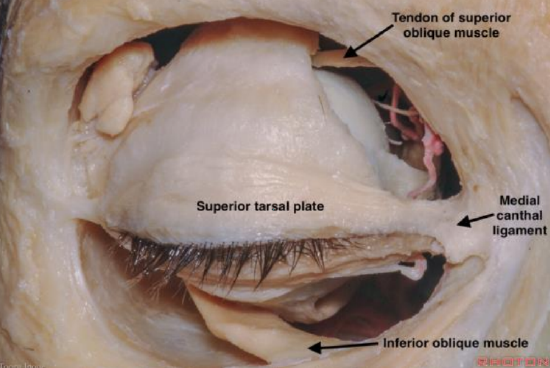
Figure 1: Right eye medial canthus
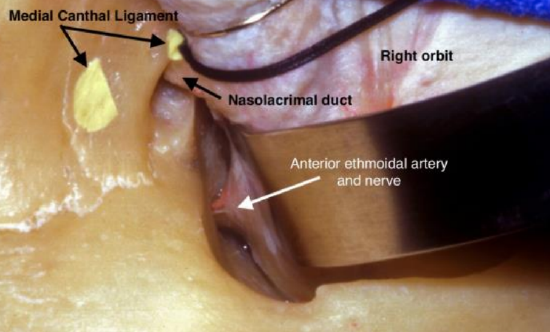
Figure 2: Right eye as seen from above with retractor retracting orbit laterally to show the anterior ethmoidal artery
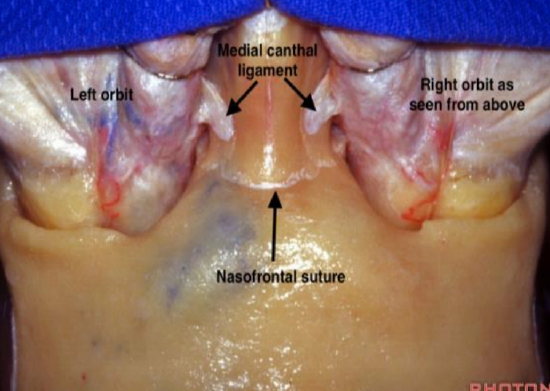
Figure 3: Medial canthal ligaments demonstrated from above
The medial canthus is where the upper and lower eyelids meet. It includes the canthal tendon and lacrimal canaliculi. The canaliculi and tendon are superficial to the area of dissection and should be preserved if the dissection is done within the correct surgical plane (Figures 1-3).
As the medial canthus is difficult to reconstruct, great care should be taken to avoid injury to these structures.
Lacrimal system

Figure 4: Lacrimal dilator, probes and irrigation

Figure 5: Probing and syringing of lacrimal system
The lacrimal canaliculi run in a plane superficial to the plane of dissection of the precaruncular approach. The surgeon can cannulate the canaliculi after dilating the superior and inferior puncta to ensure that these structures are not injured during the surgery. If familiar with dacryocystorhinostomy (DCR) surgery, this is usually unnecessary (Figures 4 & 5) (Chapter on DCR).
The lacrimal sac and nasolacrimal duct lie below the frontoethmoidal suture line (Figure 2) and dissection of this area is unnecessary if doing an anterior and posterior ethmoidal artery ligation, accessing the medial orbit for orbital tumors, decompressive surgery or during multiportal surgery.
Attachments of medial orbital structures to bony orbit
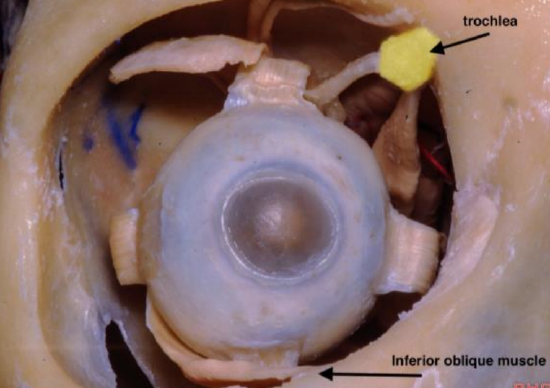
Figure 6: Right eye showing the medial portal located between the trochlea and the insertion of the inferior oblique muscle
The medial (precaruncular) portal is located between the attachment of the trochlea to the superior-medial wall of the orbit and the attachment of the inferior oblique muscle to the inferior orbit (Figures 1 & 6).
It is important to remember that because these structures attach to the periorbital fascia, dissecting in the subperiosteal plane (between bone and periorbital fascia) is essential to avoid damage to these structures. It is usually unnecessary to dissect close to these structures unless an extended approach is required where the medial portal is combined with superior or inferior portals.
The trochlea is a cartilaginous sling that acts as a pulley for the superior oblique muscle. It is located approximately 1.5 cm superior to the lacrimal caruncle1 (Figures 1, 6). The trochlear fossa is about 4 mm from the orbital margin. This is where the pulley is attached.
The inferior oblique arises from the orbital surface of the maxilla, lateral to the lacrimal groove. It is the only muscle that does not originate from the common tendinous ring (annulus of Zinn). The muscle passes laterally, posteriorly and superiorly (Figure 6) and runs between the inferior rectus and the floor of the orbit and passes just underneath the lateral rectus muscle. It inserts onto the sclera between the inferior and lateral rectus muscles. Once again, one should avoid trying to identify this muscle during a pure medial approach and always remain in a subperiosteal plane when dissecting the periorbital fascia off the bony orbital wall.
Structures encountered during the medial precaruncular approach
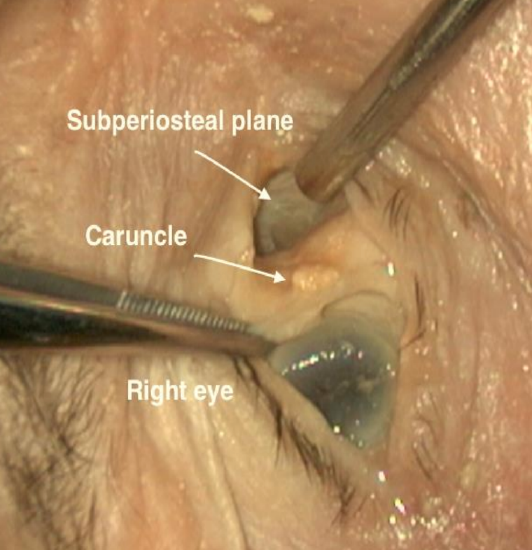
Figure 7: Caruncle of right eye
Caruncle: The caruncle is a small mound of tissue that located at the medial aspect of the eye (Figure 7). Its function is most likely related to directing the flow of tears to the lacrimal puncti.

Figure 8: Horner’s muscle identified in the right eye. The anterior ethmoidal artery lies 12 mm posterior to this muscle
Horner’s muscle: This is a small muscle that can be identified in the most anterior part of the medial orbit. It is one of the first structures encountered once the incision is made through the conjunctiva between the caruncle and the medial canthal skin (Figure 8). Its function is not quite clear, but it most likely also assists with drainage of tears through the lacrimal system.
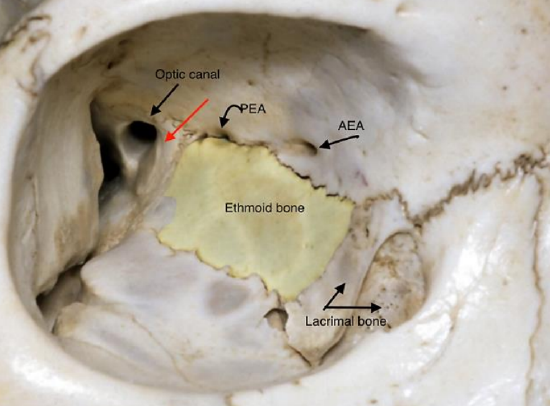
Figure 9: Right eye showing the frontoethmoidal suture line above the ethmoid bone (yellow) with the anterior ethmoidal artery (AEA) and the posterior ethmoidal artery (PEA) close to this suture line. Red arrow = bone of sphenoid body
Frontoethmoidal suture line: This is only clearly visible in 50% of patients2 and is therefore not a great landmark for the ethmoidal arteries. If visible, the ethmoidal vessels and nerves are found within the suture line or just above it (Figure 9).
If it is not clearly identifiable, then the nasion should be used as a landmark for the ethmoidal vessels as the ethmoidal arteries are at the same level as the nasion2.
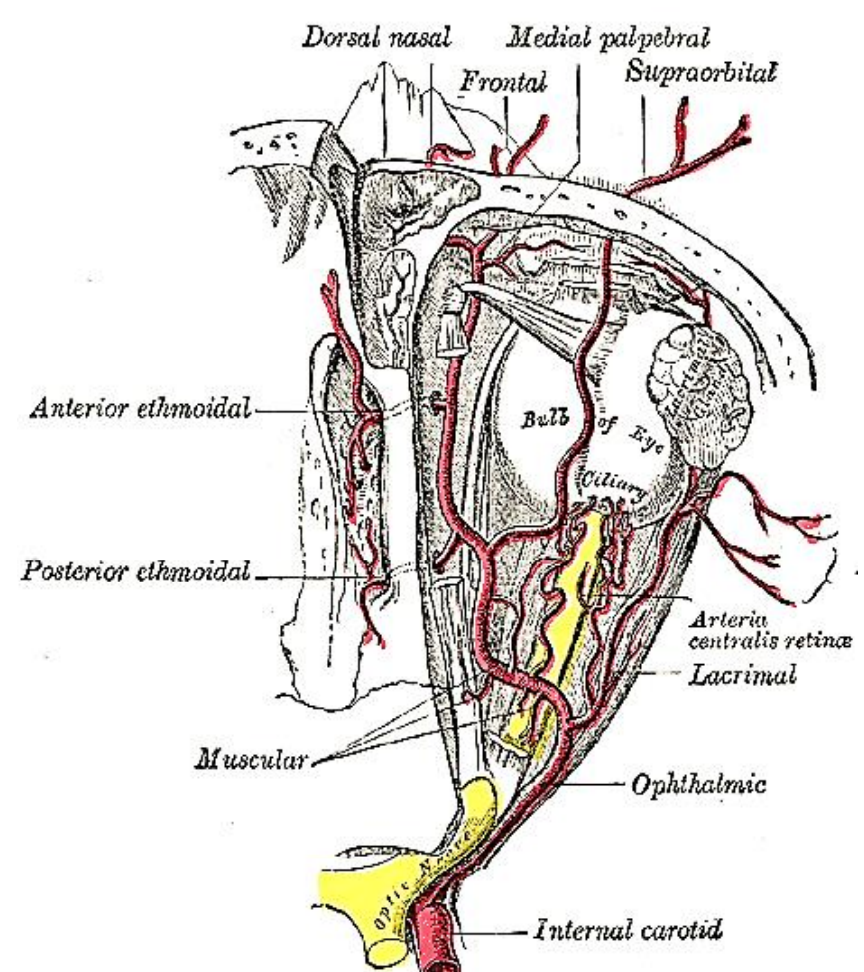
Figure 10: Ophthalmic artery gives rise to anterior and posterior ethmoidal arteries
Anterior and posterior ethmoidal arteries: These are branches of the ophthalmic artery and are therefore branches of the internal carotid artery system (Figure 10). The arteries run from the orbit to the nasal cavity (lateral-to-medial).
There are numerous ways to find the arteries using their relationships to other structures:
- The arteries are at the level of the nasion 2 or nasofrontal suture line (Figures 2,3,9)
- Close to (within or above) the frontoethmoidal suture line, which is only clearly visible in 50% (Figure 9)
- 12 mm posterior to Horner’s muscle 2
- “24-12-6 rule”: The anterior ethmoidal artery can be found 24 mm from the anterior lacrimal crest; the posterior ethmoidal foramen is 12 mm posterior to this; and the optic canal 6 mm posterior to the posterior ethmoidal artery.
Note: When the precaruncular approach is used to ligate the ethmoidal vessels, the lacrimal crest does not have to be exposed.
Accessory ethmoidal arteries: These are often encountered between the anterior and posterior ethmoidal arteries. They usually are very small and are easily transected during elevation of the periosteal layer.
It is important to remember that the posterior ethmoidal artery can be absent. Great care should therefore be taken before cauterizing or ligating a structure that could possibly be the optic nerve. If there is any doubt, it is safer to not cauterize the 2nd artery as any trauma to the optic nerve would lead to blindness.
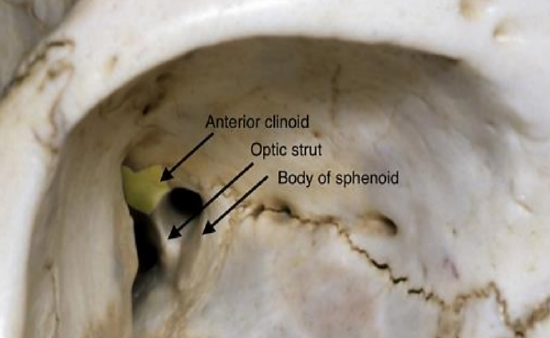
Figure 11: Right optic canal formed by the body and the lesser wing of the sphenoid See optic strut (inferiorly) and anterior clinoid (posteriorly)
Optic canal: The optic canal is found 6 mm posterior to the posterior ethmoidal artery in the most posterior-medial aspect of the bony orbit (Figure 11).
It is located within the sphenoid bone and is bound medially by the body of the sphenoid and laterally by its lesser wing (optic strut) (Figure 11).
Indications for Precaruncular Approach
Preoperative planning
The need for imaging depends on the indication for surgery. For any surgery other than ethmoidal artery ligation, preoperative imaging is mandatory. For simple ligation of the ethmoidal vessels, preoperative CT imaging is not required. If a patient has proptosis secondary to an intra- or extraconal lesion (space within the orbit outside the musculofascial cone), then preoperative CT and MRI is useful to assess the location of the lesion relative to the rectus muscles and optic nerve. Navigation is also useful to locate any pathology other than the ethmoidal arteries.
Ophthalmological examination is indicated for any patient who has orbital pathology, proptosis or visual abnormalities. It is important to document the visual acuity, visual fields if indicated, degree of proptosis and intraocular pressure prior to performing any surgery. The only indication for not performing these tests would be for ligation of the ethmoidal arteries in a patient with no orbital pathology or visual problems.
Preoperative counselling includes mentioning all the possible complications that could occur if any important structures are injured during this approach. It is important to explain to patients that this approach has been used since 2010 with very few if any complications reported in the literature. Injury of the lacrimal system can cause epiphora; injury to the ethmoidal vessels can cause an orbital hematoma or intracranial hemorrhage if there is any backflow of blood; medial rectus muscle injury will cause diplopia; and optic nerve injury will cause blindness. Entering the medial cavernous sinus can injure cranial nerves III, IV, VI and the internal carotid artery causing a stroke or death.
It needs to be stressed that the precaruncular approach is minimally invasive, requires minimal dissection of uninvolved tissue (sinuses, lamina papyracea, rectus muscles), with little pain because of the little disruption of normal tissues, requires no suturing and with early discharge from the hospital (often the same day and minimal if any morbidity.
Surgical technique
- Anesthesia and positioning
- Preoperative preparation & instruments
- Surgical steps
- Postoperative management
1. Anesthesia and positioning
- Surgery is as for routine FESS surgery with the patient supine with the head flat or flexed 15 degrees (See Chapter on FESS)
- The head is turned slightly to the side of the surgeon
- The surgeon always stands on the left of the patient (when facing the patient) for a left-handed surgeon, regardless of which eye needs to be addressed
- The author prefers total intravenous anesthesia (TIVA), but it is essential to have a slow heart rate and normotensive patient to assist with hemostasis
- 1 Gram of IV Kefzol is given at induction because multiportal surgery is often performed – this means the eye could possibly be contaminated with nasal organisms if a transnasal approach is combined with a transorbital approach
2. Preoperative preparation and instruments
- If the endonasal route is to be used, standard packing techniques are used, using 2 mL of 1:1000 Adrenaline topically on neurosurgical patties (See Chapter on FESS)
- Clean the eye prior to draping with either normal saline or diluted Betadine solution (unless allergic to iodine). It is important to instruct the scrub nurse not to clean the eye with any products that could potentially damage the cornea or irritate the sclera (e.g. Chlorhexidine solution)

Figure 12: Injecting 1:80 000 Adrenaline with Lidocaine into the medial canthus
- Inject 0.2 mL local anesthetic (1:80,000 Adrenaline with 2% Lidocaine) at the start of surgery, between the caruncle and the skin edge of the eye (Figure 12) for hemostasis during the initial dissection of the precaruncular portal
- It is important to keep the cornea moist or to protect it with a corneal protector throughout the procedure to prevent any corneal trauma, as drying of the cornea can cause corneal ulceration or keratitis
Instrument requirements
- Camera system
- Zero-degree 4 mm standard 18 cm endoscope (sinuscope)
- Standard FESS tray
- Additional essential instruments
- Ribbon retractors / Dural retractors (on neurosurgery tray): Ensure that a variety of sizes (8 mm, 10 mm, 15 mm) of retractors are available
- Small cat’s paw retractor
- Suction Freer
- Freer elevator
- Bipolar forceps (as used with tonsillectomy)
- Ligaclip applicator
3. Surgical steps

Figure 13: Right eye; retracting the caruncle laterally to incise between the caruncle and the medial canthal skin
- Identify the caruncle of the eye, grasp it with toothed forceps and retract it laterally (Figure 13)
- Incise the conjunctiva between the caruncle and the medial canthal skin with sharp iris scissors
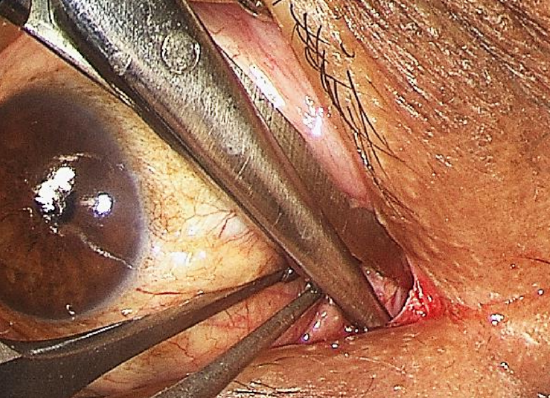
Figure 14: Right eye; precaruncular incision. Scissors inserted between caruncle and medial canthal skin, spreading tissues as soon as the bone is felt
- Aim the tip of the scissors towards the bone of the medial wall of the orbit, and dissect deep to the lacrimal canaliculi to prevent traumatizing them (Figure 14)
- Surgeons not familiar with lacrimal anatomy should ask their ophthalmology colleagues to help dilate both puncti and insert probes into the canaliculi to ensure that the dissection is deep to these structures. Damaging the canaliculi could lead to epiphora (Figures 4,5)
- Once the tip of the scissors hits the bony orbital wall, the scissors is opened to ‘spread’ the orbital tissues to identify the bony orbital wall (Figure 14)
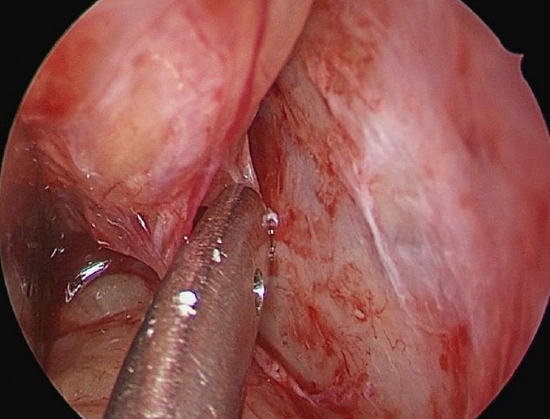
Figure 15a: Right eye; precaruncular incision with suction Freer elevator used to dissect in subperiosteal plane towards ethmoidal arteries
- Once bone is exposed, use a suction elevator, Cottle elevator or Freer’s elevator to dissect in the subperiosteal plane between bone and periorbital fascia (Figure 15a)
- As with septoplasty surgery, it is important to be in the correct plane to avoid breaching the periorbital fascia, as this would cause orbital fat to herniate into the surgical corridor and make further surgery difficult

Figure 15b: A ribbon retractor is used to retract the orbit laterally (a retractor to retract the eyelids, as seen in this picture, is not routinely required)
- Use ribbon retractors to retract the orbital contents laterally (Figure 15b). Ensure that a variety of sizes (8 mm, 10 mm, 15 mm) of ribbon retractors are available
- Take great care with the amount of traction applied to the eye by the surgical assistant, especially at the posterior aspect of the orbit where excessive pressure with the retractor can cause damage to the optic nerve or the medial rectus muscle
- Insert the endoscope into the surgical portal as soon as the subperiosteal plane can be visualized – usually within 1 cm of the initial incision
- It is easier to find the exact plane using the endoscope
- The endoscope initially rests on the ribbon retractor for stability
- The author uses a standard 4 mm 18 cm sinus endoscope, but a 3 mm wide angled scope will give good visualization with a bit more space for manipulating instruments within the surgical corridor
- The rest of the procedure is performed using the endoscope
- Check the pupil for any changes in size or shape every 5 minutes while retracting as pupillary changes indicate raised intraocular pressure which can cause visual loss
- A small cat’s paw retractor can be used to retract the medial canthus medially to ‘open up’ the surgical portal between the ribbon retractor and the cat’s paw
- Continue the dissection in the subperiosteal plane, dissecting more superiorly towards the level of the nasion with the suction Freer elevator
- The first structure encountered is Horner’s muscle
- The dissection may well be more posterior to Horner’s muscle, so if it is not easily identified then proceed to find the next landmark
- Try to identify the frontoethmoidal suture line
- If this is not possible, then determine the level of the nasion – this is the level at which the ethmoidal vessels will be found
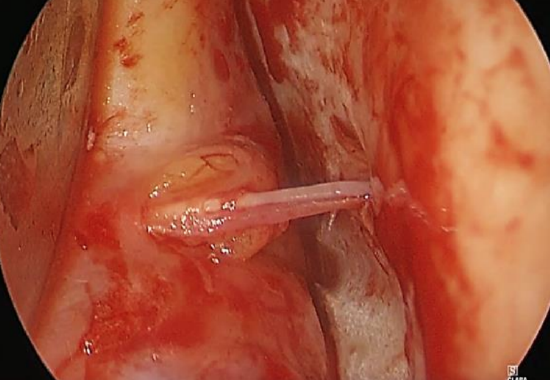
Figure 16: Right eye; anterior ethmoidal artery with a bit of fat herniating through the periorbital fascia
- Find the anterior ethmoidal artery; it is easily identified as a ‘tenting structure’ as the suction elevator elevates the periosteum off the bony orbital wall (Figure 16)
- A bit of orbital fat often herniates through the periorbital fascia where the artery exits the orbit (Video). This fat can also be used as a landmark to find the artery. In about 50% of females this fat is a constant landmark for the artery (Figure 16)
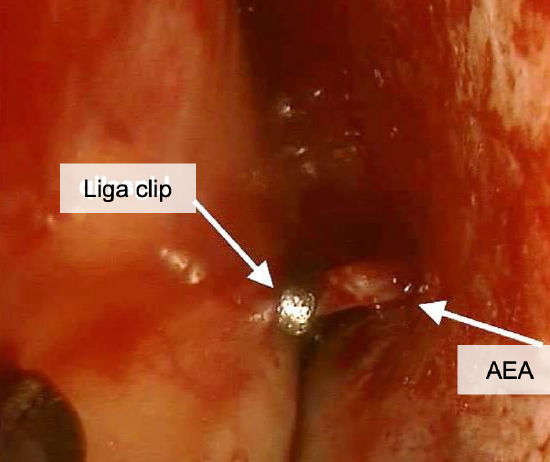
Figure 17: Right eye; anterior ethmoidal artery (AEA) has been clipped as the artery leaves the orbit
- Use a standard tonsil bipolar forceps to cauterize the anterior ethmoidal artery or apply a ligaclip (Figure 17)
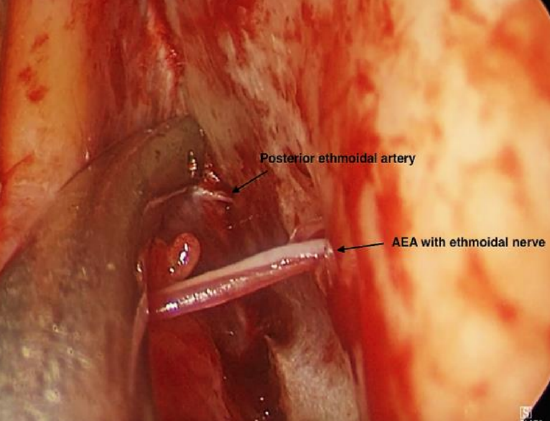
Figure 18a: Posterior ethmoidal artery 12 mm posterior to AEA
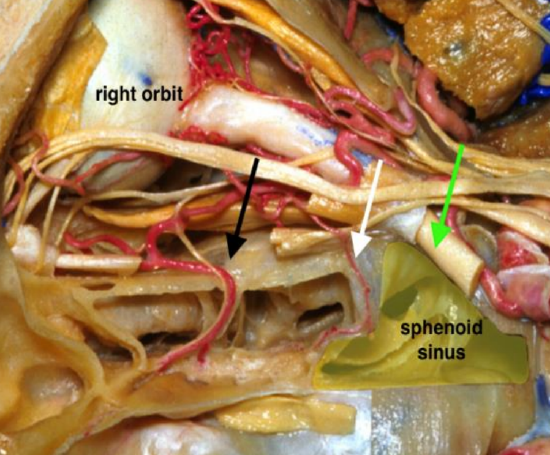
Figure 18b: Note close proximity between the AEA (black arrow), PEA (white arrow), and optic nerve in optic canal (green arrow)
- Find the posterior ethmoidal artery 12 mm behind the anterior ethmoidal artery (Video) (Figures 18ab)
- It is important to remember that there are often small accessory ethmoidal arteries and that the posterior ethmoidal artery may be absent
- It is imperative to ensure that the optic nerve is not confused for the posterior ethmoidal artery. Therefore contemplate carefully before ligating what you think is the posterior ethmoidal artery
Deciding how to proceed at this point depends on the indication for using the precaruncular approach
- If the aim of the surgery was to ligate the vessels, the surgical portal is irrigated with saline and nasal endoscopy is done to check that hemostasis has been achieved
- There is no need to suture the precaruncular incision
Precaruncular approach as extra portal during multiportal surgery for access to posterior orbit and for optic nerve decompression

Figure 19: Multiportal surgery using combined precaruncular and binostril approaches for optic nerve decompression
These procedures require retraction of the orbital contents. They may be combined with an ipsilateral endonasal approach, or a binostril approach (Figure 19, video). However, a precaruncular approach can be used on its own without an endonasal approach, thereby preserving the normal sinus anatomy.
Indications for precaruncular approach to decompress the orbit include
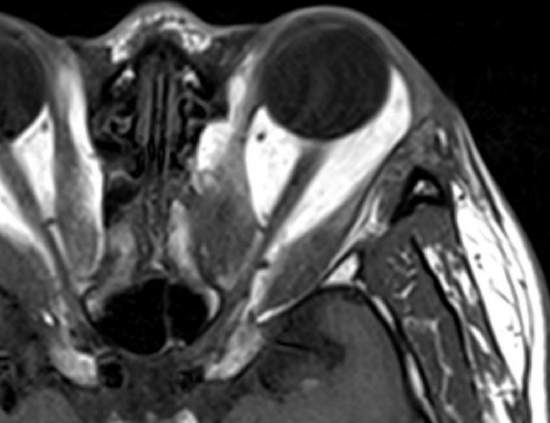
Figure 20: Previous medial decompression for thyroid eye disease with prolapse of orbital fat, making access to the posterior orbit and optic nerve difficult using a purely endonasal approach
- Thyroid orbitopathy (Figure 20)
- Severe proptosis
- Previous medial decompression has been performed and further decompression is required (Figure 20)
Optic nerve decompression involves the following steps
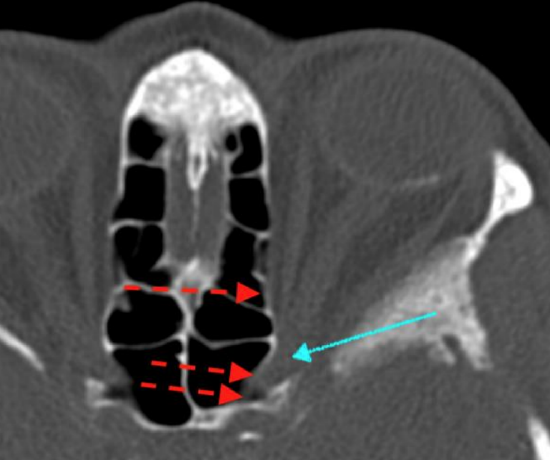
Figure 21: Optic nerve (blue arrow) within optic canal. Single red arrow shows where lamina is removed during optic nerve decompression. Double red arrow shows extent of decompression needed
- Remove the posterior 1/3 of the lamina papyracea by fracturing the lamina towards the ethmoid sinuses and away from the periorbita (Figure 21)
- Keep the nasal mucosa intact if an endonasal approach is not required
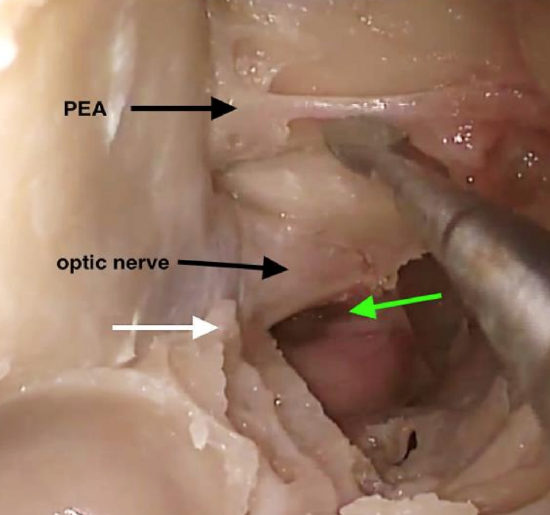
Figure 22: Right optic nerve decompression from the optic protuberance (white arrow) to the opticocarotid recess (green arrow)
- The optic canal is found just below the level of the ethmoidal arteries (Figures 11, 17ab, 22). Therefore, ensure that dissection is carried out at this level
- Once the anterior face of the sphenoid is identified, the posterior ethmoidal artery can be visualized at the angle where the superior aspect of the sphenoid sinus face meets the skull base (Figure 22)
- Decompress the optic canal for a distance of 1 cm from the optic protuberance to the opticocarotid recess (OCR) (Figure 22)
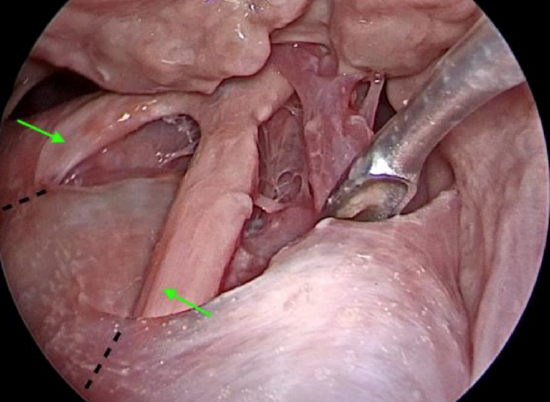
Figure 23: Optic nerves as seen from above through a lateral transorbital approach with 70-degree endoscope. Image shows the intracranial component of the optic nerves (green arrows) as it leaves the optic canal (black interrupted lines)
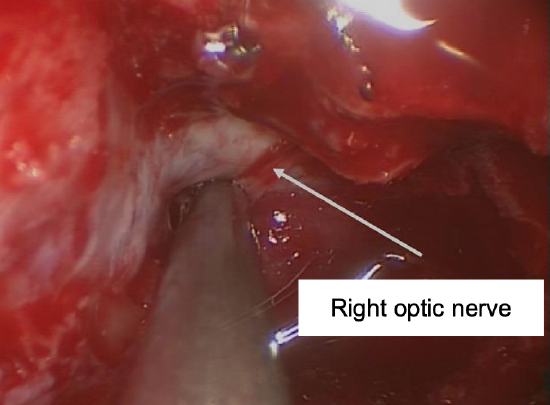
Figure 24: Right optic nerve decompression from the optic protuberance to the OCR
- Beyond the opticocarotid recess the optic nerve runs intracranially. Decompression beyond this point is unnecessary unless the optic chiasm itself needs to be decompressed (Figures 23, 24)
- It is not the author’s practice to fenestrate the optic nerve sheath during optic nerve decompression
Precaruncular approach to medial orbital tumors
The precaruncular approach can be used to access intra- or extraconal lesions involving the medial orbit. Cavernous hemangioma is one of the most common pathologies encountered within the orbit and the precaruncular portal is the most minimally invasive approach to remove these lesions. It is important to study the imaging (CT and MRI) preoperatively and to assess the location of the lesion in relation to important orbital structures – the rectus muscles and the respective nerves that innervate them and vessels that supply them. An ophthalmological examination is essential, and all cases should be done in conjunction with an ophthalmologist.
- Incise the periorbital fascia
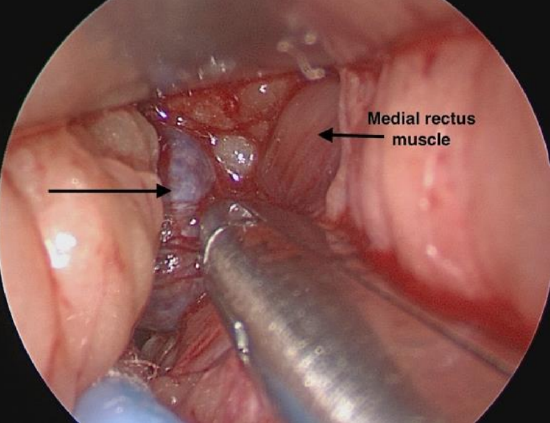
Figure 25: Right eye; precaruncular approach to intraconal cavernous hemangioma (black arrow)
- Dissect bluntly to the lesion as previously described (Figure 25)
- Neurosurgical patties can be used to help retract fat during dissection
- No reconstruction is required as the medial wall of the orbit is not breached during surgery
Postoperative management
- At conclusion of the surgery, irrigate the surgical portal with normal saline
- It is important to ensure that adequate hemostasis has been achieved and that the ethmoidal arteries have been cauterized or ligated

Figure 26: There is no need to suture the precaruncular incision. It is important to examine the pupil for asymmetry. Green threads are from neuropattie that is still in situ for hemostasis, and will be removed before end of surgery
- The surgical incision site is not sutured (Figure 26)
- It is important to check the patient’s vision and eye movements immediately after surgery
- A cold pack can be applied over the eye for a few minutes every hour in the first 24 hours to prevent bruising in the medial canthal area
- Topical chloromycetin ointment is applied in the corner of the eye for 3-5 days following surgery
References
- Shin HJ, Gil YC, Shin KJ, et al. Identification of the trochlea with reference to the lacrimal caruncle, and its significance as a landmark in orbitofacial surgery. J Plast Reconstr Aesthet Surg. 2015 Mar;68(3):351-5
- Cornelis M, Lubbe DE. Clin Otolaryngol. Pre-caruncular approach to the medial orbit and landmarks for anterior ethmoidal artery ligation: a cadaveric study. 2016 Dec;41(6):777-81
Author
Darlene Lubbe MBChB, FCORL
Associate Professor
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
doclubbe@gmail.com
Editor
Johan Fagan MBChB, FCS (ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za