
4.4: Juvenile Nasopharyngeal Angiofibroma Surgery
- Page ID
- 15450

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
JUVENILE NASOPHARYNGEAL ANGIOFIBROMA SURGERY
Derek Rogers, Christopher Hartnick, Johan Fagan
Juvenile nasopharyngeal angiofibroma (JNA) is a rare tumor representing only about 0.05% of head and neck tumors.1 The most common presentation is a prepubescent or adolescent male with severe, recurrent epistaxis and nasal obstruction. The epistaxis may even require a blood transfusion. Since JNAs occur exclusively in males, a hormonal theory has been implicated.
As these tumors are quite rare, many patients may have been treated conservatively by a primary care provider before being referred to an otolaryngologist. Patients may have undergone a trial of nasal steroids and antihistamines or been mistaken for having simple anterior epistaxis. An adolescent male with recurrent epistaxis and chronic nasal obstruction is highly suspicious for a JNA. The epistaxis and nasal obstruction progressively worsen. Unilateral nasal obstruction may progress to bilateral obstruction as the tumor grows to fill the nasopharynx. Other common symptoms include headache, facial swelling, unilateral rhinorrhea, hyposmia, and ipsilateral conductive hearing loss due to Eustachian tube dysfunction.
JNAs originate from the sphenopalatine artery near the sphenopalatine foramen, an anatomic area usually readily accessible via endoscopic technique. Hence most of these tumors are now removed via an endoscopic approach by surgeons skilled in endoscopic surgery working in properly equipped centers. Compared to open approaches, the endoscopic approach results in less intraoperative blood loss, fewer complications, lower rates of recurrence, and shorter hospital stays.2 Due to the vascularity of these tumors, preoperative embolization of major feeding vessels by interventional radiology leads to significantly less blood loss and facilitates endoscopic resection.3
Traditionally, several open approaches are employed, including lateral rhinotomy, midfacial degloving, transmaxillary (Caldwell-Luc), transpalatal, Le Fort 1 and infratemporal fossa approaches. Extensive tumors, such as those with lateral infratemporal fossa involvement or significant optic canal or intracranial extension may necessitate an open or a combined open and endoscopic approach. Radiotherapy and anti-androgen therapy are reserved for tumors deemed inoperable.4
Pertinent Anatomy
It is essential that a surgeon be familiar with the detailed vascular anatomy of the maxillary artery and its terminal branches, and that of the maxilla, paranasal sinuses, pterygoplatine fossa, orbit and anterior skull base. Studying a cadaver skull and having it available in the operating room is of great value.
Vascular anatomy

Figure 1: Internal maxillary artery entering pterygopalatine fossa through pterygomaxillary fissure (mandible removed)

Figure 2: Branches of internal maxillary artery; blue shading denotes 2nd part of internal maxillary artery before it enters pterygopalatine fossa
JNAs typically arise from the sphenopalatine artery, which is a terminal branch of the internal maxillary artery. The internal maxillary artery branches off the external carotid artery (Figures 1, 2). The sphenopalatine artery usually contains two or more branches. Larger tumors can however have arterial supply from the ascending pharyngeal, contralateral internal maxillary artery, and be supplied by the cavernous portion of the internal carotid artery at the lateral wall of sphenoid sinus.
Bony anatomy (Figures 3, 4)

Figure 3: Total maxillectomy defect illustrating the relations of the pterygopalatine fossa (Red)

Figure 4: Close-up of Figure 3

Figure 5: Endoscopic view of posterior wall of (R) maxillary antrum through a large middle meatal antrostomy: sphenopalatine artery is located directly posterior to crista ethmoidalis; posterior nasal artery is superior to sphenopalatine arter

Figure 6: Internal maxillary artery (red arrow) traverses the pterygomaxillary fissure to enter the pterygopalatine fossa

Figure 7: Axial cut at level of infraorbital nerve and orbital floor

Figure 8: Axial cut at level of infraorbital foramen and pterygoid plates

Figure 9: Coronal cut immediately behind the maxillary sinus through the orbital apex, pterygoid plates and pterygopalatine fossa
JNAs typically arise from the lateral nasal wall at the sphenopalatine foramen and generally involve the pterygopalatine fossa. The sphenopalatine foramen is located along the lateral nasal wall immediately posterior to the crista ethmoidalis and opens into the middle and superior meati (Figures 3-5). The pterygopalatine fossa is located immediately behind the thin posterior wall of the maxillary sinus (Figures 3, 4). It serves as a gateway to the nasal and oral cavities, infratemporal fossa, orbit, pharynx, and middle cranial fossa through eight foramina.5 It communicates laterally with the infratemporal fossa via the pterygomaxillary fissure, and medially with the nasal cavity via the sphenopalatine foramen (Figures 3, 4). Immediately posterior are the pterygoid plates (Figures 3-9). Figures 7 & 8 show axial views of the anatomy of the pterygopalatine fossa, pterygomaxillary fissure, and maxillary sinus.
Figures 3, 4 & 9 demonstrate the coronal anatomy immediately posterior to the maxillary sinus in which the internal maxillary artery and its branches as well as the sphenopalatine ganglion and its branches are encountered within the pterygopalatine fossa. It also illustrates how a JNA may extend superiorly though the inferior orbital fissure into the orbit, medially into the nasal cavity and sphenoid, and laterally into the infratemporal fossa.
Nerves

Figure 10: V2, pterygopalatine ganglion and infraorbital nerve (pterygopalatine fossa in red)
The maxillary division of trigeminal (V2) enters the pterygopalatine fossa via for amen rotundum (Figures 7, 10). The infraorbital nerve is a terminal branch of V2 and runs in the floor of the orbit/roof of the antrum to exit the infraorbital foramen.
Preoperative Evaluation
Clinical Evaluation

Figure 11: View of right nasal cavity showing large, vascular mass
A thorough history and physical are performed. The history should focus on the aforementioned nasal symptoms as well as any orbital symptoms. The initial head and neck physical examination notes any proptosis, vision changes, facial swelling, or otitis media with effusion. Fiberoptic nasopharyngoscopy is performed which typically reveals a vascular mass emanating from the posterior aspect of the middle and/or superior meatus, possibly filling the nasopharynx (Figure 11). The mass must not be biopsied due to the risk of causing significant epistaxis and as it may represent an encephalocoele or other nasal mass with an intracranial component.
Radiologic Evaluation

Figure 12a: CT scan: Widening of the sphenopalatine foramen and nasal cavity

Figure 12b: CT scan: Anterior bowing of posterior wall of maxillary sinus (HolmanMiller sign) and nasal mass
CT and MRI scans with contrast should be obtained to evaluate the extent of the tumor. CT scan helps delineate the bony anatomy (Figures 12a, b). JNAs usually cause widening of the sphenopalatine foramen and may cause anterior bowing of the posterior wall of the maxillary sinus, also known as the Holman-Miller sign (Figure 12b).

Figure 13a: MRI: No orbital or intracranial extension

Figure 13b: MRI: Extension to medial infratemporal fossa
MRI provides essential information regarding soft tissue structures including the tumor, orbital structures, and intracranial components (Figures 13a, b). It also permits a distinction to be made between retained sinus secretions and mucosal edema vs. tumor.
Staging systems
Several staging systems have been proposed based on the radiologic appearance of JNAs. Two commonly used systems were developed by Fisch 6 (Table 1) and Radkowski7 (Table 2). More recently a staging system was proposed based primarily on prognostic factors for endoscopic resection (Table 3). 8
| Stage | Description of Tumor Involvement |
| I | Limited to nasopharynx, bone destruction negligible or limited to sphenopalatine foramen |
| II | Invades pterygopalatine fossa or maxillary, ethmoid, or sphenoid sinus with bone destruction |
| III | Invades infratemporal fossa or orbital region IIIA: No intracranial involvement IIIB: Extradural, parasellar involvement |
| IV | Invades dura IVA: Without cavernous sinus, pituitary, or optic chiasm involvement IVB: With the above |
Table 1: Fisch Staging for JNA
| Stage | Description of Tumor Involvement |
| I | IA: Limited to nose or nasopharynx IB: Same as above but involving ≥ 1 sinus |
| II | IIA: Minimal extension through sphenopalatine foramen and into medial pterygomaxillary fossa IIB: Full occupation of pterygomaxillary fossa displacing posterior wall of maxillary sinus forward, orbit erosion, displacement of maxillary artery branches IIC: Involvement of infratemporal fossa or cheek, or posterior to pterygoid plates |
| III | Erosion of skull base IIIA: Minimal intracranial involvement IIIB: Extensive intracranial involvement or any cavernous sinus extension |
Table 2: Radkowski Staging for JNA
| Stage | Description of Tumor Involvement |
| I | Nasal cavity, medial pterygopalatine fossa |
| II | Paranasal sinuses, lateral pterygopalatine fossa, no residual vascularity |
| III | Skull base erosion, orbit, infratemporal fossa, no residual vascularity |
| IV | Skull base erosion, orbit, infratemporal fossa, with residual vascularity |
| V | Intracranial extension, residual vascularity Medial (M): Medial cavernous sinus Lateral (L): Middle cranial fossa |
Table 3: University of Pittsburgh Medical Center (UPMC) Staging for JNA
Angiography

Figure 14a: JNA (circled) supplied by internal maxillary and ascending pharyngeal arteries

Figure 14b: JNA following embolization with persistent supply from ascending pharyngeal artery
Angiography is both diagnostic and therapeutic; it is performed 24-72 hours before surgery to determine the precise blood supply to the tumor and to embolize feeding vessels. Flooding the tumor with small particles is preferred, as coiling major vessels proximally precludes subsequent embolization should the tumor recur. By thrombosing the tumor with microparticles, smaller supply vessels from e.g. the internal carotid artery system also thrombose; hence bleeding from the internal carotid artery generally does not present a problem when delivering tumor from the sphenoid sinus. It is important that the surgeon discusses the outcome of the embolization with the interventional radiologist to determine how successful the embolization had been, and what vessels need to be surgically ligated or clipped (Figures 14a, b).
Should interventional angiography not be available, then surgery must be planned in such a way as to gain proximal vascular control of the internal maxillary artery and/or external carotid artery prior to attempting resection.
General surgical principles
- JNAs may be resected by endoscopic, open or combined (endoscopic & open) techniques
- The surgical approach is dependent on
- Tumor location and extent
- Pattern of vascular supply
- Effectiveness of embolization
- Facial skeletal maturity
- Experience of the surgical team
- Carefully plan surgical approach(es) according to the imaging studies
- In expert hands and with effective preoperative embolization, most JNAs can be removed endoscopically with reduced morbidity
- Complete all bone work and ensure good access to the tumor before attempting resection, because once bleeding is encountered, the surgery may become very difficult and hazardous, and hemostasis may only be possible after completing the tumor resection
- In young patients, avoid excessive soft tissue and bone dissection of the midface to minimize the risk of causing growth abnormalities 9
Anesthesia considerations
- Patients are placed supine in reverse Trendelenburg position
- Oral RAE® endotracheal tube permits unobstructed access to the nose
- Hypotensive general anesthesia
- Type and crossmatch 2 units of blood as rapid blood loss can occur; consider banking 2 units of autologous blood one week before surgery
- Intraoperative blood salvage (autologous blood transfusion/cell salvage/cell saver technique) can be employed to recover blood lost during surgery which is reinfused into the patient
Endoscopic resection
Indications
- Tumors involving nasal cavity, paranasal sinuses, and nasopharynx
- Tumors with only medial infratemporal fossa involvement or extradural parasellar involvement with limited intracranial extension
- Facilitation of open approaches
Relative contraindications
Lateral infratemporal fossa involvement, extensive parasellar extension, encasement of the optic nerve, intradural spread, or cavernous sinus involvement. Note that cavernous sinus involvement is often overestimated on MRI scan due to hypervascularity of the tumor bed.
Intraoperative considerations
- Self-cleaning endoscope such as EndoScrub®
- Suction bipolar electrocautery, suction Freer elevator, suction Blakesley forceps or Kerrison rongeur, and hemoclip applier
- Intraoperative image guidance (if available)
Procedure
- Inject Lidocaine with epinephrine into the greater palatine foramina, septum, uncinate and middle turbinate on the side with the tumor
- Pack both nasal cavities for 10 minutes with cottonoid pledgets soaked in oxymetazoline
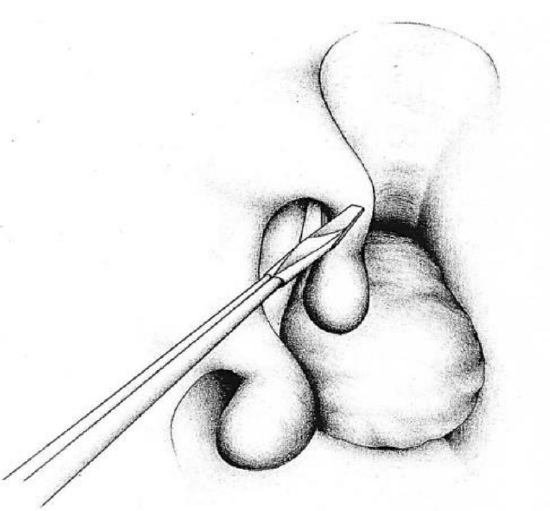
Figure 15: The middle turbinate is amputated to provide access to the tumor
- On the side with the tumor, amputate the inferior aspect of the middle turbinate with scissors (Figure 15)
- The tumor may initially need to be partially debulked to identify landmarks (only if well embolized)
- Perform an uncinectomy and wide middle meatal antrostomy

Figure 16: Intraoperative photo (right nose) following middle meatal antrostomy, showing crista ethmoidalis and posterior maxillary sinus wall
- Enlarge the middle meatal antrostomy until the posterior wall of the maxillary sinus is clearly visible (Figures 5, 16)
- Consider doing a posterior septectomy to allow better visualization and access from the opposite nasal cavity
- Perform a total ethmoidectomy and identify the sphenoid rostrum
- Completed a sphenoidotomy to ensure that tumor does not extend into the sphenoid

Figure 17: Intraoperative photo showing Kerrison rongeur used to remove posterior maxillary sinus wall

Figure 18: The posterior wall of the maxillary sinus is removed along the sphenopalatine artery

Figure 19: The tumor is dissected to its vascular pedicle

Figure 20: Sphenopalatine artery has been clipped in the pterygopalatine fossa
- Expose the sphenopalatine artery and tumor pedicle by removing the posterior wall of the maxillary sinus (Figures 17-19)
- Isolate and clip/ligate the sphenopalatine artery lateral to the tumor, even if it has been embolized (Figure 20)
- If tumor extends beyond the limits of the endoscopic instruments e.g. beyond the pterygopalatine fossa into the infratemporal fossa, then a Caldwell-Luc approach or open procedure may be needed for access
- Dissect tumor off adjacent structures; often it is adherent to septum, sphenoid rostrum, skull base, and nasopharynx
- Suction bipolar electrocautery is first used to ablate feeding vessels along the surface of the tumor; a suction Freer elevator or knife is used to release adhesions
- The tumor is dissected free until all that remains is the pedicle
- If it has not yet been done, apply hemoclips to branches of sphenopalatine artery, divide the artery, and deliver the tumor via the nasopharynx and out the mouth
- Inspect the entire mucosal area that was involved with tumor
- Biopsies may be sent to clear the margins
- Obtain meticulous hemostasis
- Apply hemostatic sinus material, such as Arista™ powder, Stammberger Sinufoam™, or Surgicel to bleeding surfaces
Postoperative Care
- The patient is admitted to the ward for overnight observation
- If intraoperative blood loss was significant, a full blood count is obtained and the patient is transfused if needed
- Oxymetazoline is used for minor epistaxis
- Nasal saline irrigations are started on the 1st postoperative day, at least twice daily, for nasal toilet
- The patient is instructed not to blow the nose
- The 1st postoperative visit is scheduled at 1 week
Complications
- Standard risks of endoscopic sinus surgery apply including pain, bleeding, infection, hyposmia, synechiae, orbital injury, loss of vision, cerebrospinal fluid leak, and intracranial injury
- Bleeding requiring transfusion
- Tumor recidivism if margins are not cleared
Key Points
- Tumor removal and postoperative recovery are greatly facilitated by preoperative embolization
- Intraoperative navigation may aid the surgeon
- Special endoscopic instruments with suction capacity are helpful to dissect these vascular tumors
- First complete all bone work to gain good access before attempting to resect tumor
- Be prepared to convert to an open approach if tumor involves the lateral infratemporal fossa or parasellar region
Open approaches
Open approaches are employed for tumors that extend to the lateral infratemporal fossa, tumors with intradural extension, and in centers that lack endoscopic expertise. Open approaches may also be used in conjunction with endoscopic resection e.g. anterior antrostomy may be employed to gain access to and clip the internal maxillary artery lateral to a large tumor or to access the infratemporal fossa. Conversely, the endoscope can be used at the conclusion of an open resection to inspect the tumor bed to ensure complete resection and to obtain haemostasis. Open approaches include the following:
- Medial maxillectomy
- Le Fort 1 osteotomy
- Transpalatal
- Maxillary swing
- Infratemporal fossa
- Facial translocation

Table 4: Access provided by different surgical approaches9
An approach or combinations of approaches is carefully selected according to the location of the tumor and its extensions (Table 4)9. Readers are referred to chapters on Total Maxillectomy, Inferior Maxillectomy, Medial Maxillectomy, and Maxillary Swing approaches for additional detail about these approaches.
Medial maxillectomy
Medial maxillectomy is suited to tumors limited to the nose, nasopharynx, sphenoid, pterygopalatine fossa, medial infratemporal fossa and medial cavernous sinus (Table 4). Unless an ethmoidectomy is required, the medial maxillectomy is more limited than that described in the chapter on medial maxillectomy.

Figure 21: Midfacial degloving approach with right medial maxillectomy

Figure 22: Lateral rhinotomy incision. Very rarely is a lip split extension required for access

Figure 23: Medial maxillectomy: typical bony removal for access to a JNA

Figure 24a: Anterior coronal CT slice demonstrating resected lateral nasal wall, and transected lacrimal sac

Figure 24b: Coronal CT through midantrum demonstrates resected lateral nasal wall including inferior turbinate, uncinate process and trimmed middle turbinate

Figure 24c: Coronal CT through posterior antrum demonstrating resected lateral nasal wall and inferior turbinate
- Soft tissue elevation is generally done by midfacial degloving approach (Figure 21); lateral rhinotomy is only required when the superior parts of the ethmoids are to be dissected (Figure 22)
- Inspect the antrum to determine the tumor extent and to plan the subsequent bony cuts
- The extent of the subsequent bony resection is tailored to the JNA
- A medial maxillectomy can now been done (Figure 23); Figures 24a-c illustrate the extent of the bone resection with the limited medial maxillectomy generally required for JNAs
- The sequence of the osteotomies is planned to reserve troublesome bleeding to the end
- Osteotomy below inferior orbital rim: A sharp osteotome/power saw/bone nibbler is used to cut along the thick inferior orbital rim just medial to the infraorbital nerve (Figures 23, 24)
- Osteotomy connecting antrostomy with nasal vestibule: A sharp osteotome is used to connect the anterior antrostomy with the floor of the nasal vestibule (Figures 23, 24)
- Osteotomy across frontal process of maxilla: This part of the dissection is often best done with a Kerrison’s rongeur or oscillating saw. There is often persistent minor bleeding from the bone that may be controlled with bone wax or cautery (Figure 23)
- Osteotomy along floor of nose: A sharp osteotome or heavy scissors is used to divide the lateral wall of the nose/medial wall of the antrum along the floor of the nasal cavity up to the posterior wall of the antrum. When doing this dissection with an osteotome, the dissection is halted when the osteotome hits up against the solid pterygoid bone (signaled by change in the sound)
- Osteotomy through lacrimal bone, and anterior ethmoids: This osteotomy is made at the level of the roof of the antrum (Figures 24b, c). The osteotomy is done by gently tapping on an osteotome or with heavy curved scissors with tips pointed inferiorly. The osteotomy stops at the posterior wall of the antrum
- Vertical posterior osteotomy through posterior end of medial wall of antrum anterior to pterygopalatine fossa: The final posterior vertical cut is made with heavy curved (Mayo) scissors as a downward continuation of the osteotomy in Point 5. It runs through the medial wall of the maxillary sinus, starting superiorly at the posterior end of the previous osteotomy, and ending at the level of the nasal floor
- The medial maxillectomy specimen is then removed by gently levering it inferiorly and laterally with the Mayo scissors while completing the posterior osteotomy, remaining lateral to and preserving middle turbinate
- An external ethmoidectomy may now safely be completed under direct vision up to cribriform plate if required
- Carefully remove the paper-thin posterior wall of the maxillary antrum to expose the JNA and the sphenopalatine and/or internal maxillary artery
- Clip/ligate/bipolar the sphenopalatine / internal maxillary artery even if it has been embolized
- Proceed with the resection using blunt and bipolar dissection; suction bipolar electrocautery is first used to ablate feeding vessels along the surface of the tumor; a suction Freer elevator or knife is used to release adhesions
- Dissect tumor off adjacent structures; often it is adherent to septum, sphenoid rostrum, skull base, and nasopharynx
- If tumor extends laterally beyond the pterygopalatine fossa into the infratemporal fossa, then remove the posterolateral antral wall for additional exposure
- Inspect the entire area that was involved with tumor; this may be aided by use of an endoscope
- Obtain meticulous hemostasis
- Apply hemostatic sinus material, such as Surgicel to bleeding surfaces
- At the conclusion of surgery, the transected lacrimal sac (Figure 24a) is slit along its longitudinal axis and the edges are sutured to the surrounding tissues or stented to avoid epiphora
Le Fort 1 osteotomy

Figure 25: Le Fort 1 osteotomy; posteriorly it passes through the pterygomaxillary fissure

Figure 26: Exposure following downfracturing of hard palate

Figure 27a: Maxilla preplated 11

Figure 27b: Maxilla down fractured to expose JNA 11

Figure 27c: JNA being delivered 11

Figure 27d: Plated osteotomy 11
Le Fort 1 osteotomy with down-fracturing of the palate is suited to tumors limited to the nose, nasopharynx, sphenoid, pterygopalatine fossa, medial infratemporal fossa and medial cavernous sinus (Figures 25, 26, Table 4). (See chapter on Inferior Maxillectomy) As with other transfacial approaches, effects on facial growth are a concern; Le Fort 1 osteotomy has been reported to result in 30% of predicted vertical growth of the anterior maxilla, though it does not affect horizontal growth and does not cause dental malocclusion. It also causes dental denervation.10 The maxilla is pre-plated with miniplates along the line of the osteotomy to ensure an accurate repair (Figure 27a).
Transpalatal approach
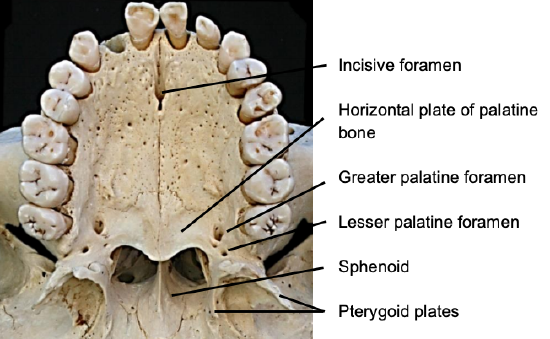
Figure 28: Anatomy of relevant to transpalatal approach
This approach can be used for JNAs confined to the nasopharynx, sphenoid and nasal cavity (Table 4). The bony anatomy of the hard palate is illustrated in Figure 28.

Figure 29: Mucosal incision in hard palate (yellow line) to elevate palatal flap; bone removal to expose tumor (chequered area)
An incision is made in the mucosa of the hard palate, and the thick mucosa is stripped off the hard palate, leaving it attached to the soft palate posteriorly (Figure 29). The soft palate is freed from the posterior edge of the hard palate to access the nasopharynx. The horizontal plate of the palatine bone is removed using a strong backbiter/Kerrison’s rongeur /drill to expose the JNA (Figure 29).
Maxillary swing approach (Figure 30)
This is described in detail in the chapter on Maxillary Swing approaches.

Figure 30: Maxilla has been fully swung laterally exposing nasopharynx; maxilla remains based on soft tissues of cheek
Infratemporal fossa approach

Figure 31: JNA extending to infratemporal fossa

Figure 32: JNA protruding anteriorly from infratemporal fossa
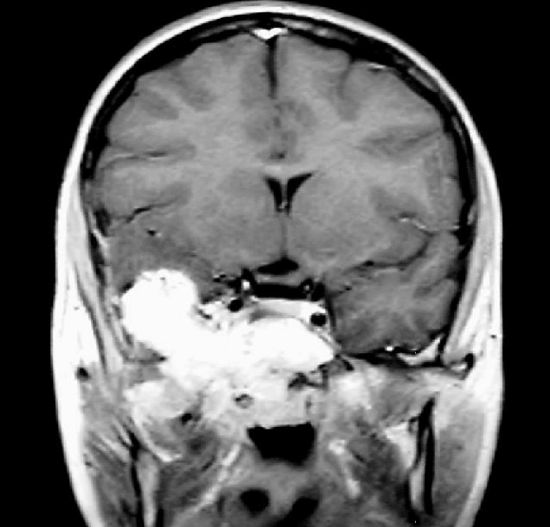
Figure 33: JNA extending to lateral cavernous sinus and middle cranial fossa

Figure 34: Infratemporal fossa is deep to zygoma (removed) and temporalis muscle

Figure 35: Internal maxillary artery is seen passing between bellies of lateral pterygoid to reach the pterygomaxillary fissure

Figure 36: View of infratemporal fossa, internal maxillary artery and pterygomaxillary fissure

Figure 37: Exposed temporalis fascia and fat pad

Figure 38: Facial nerve and fat pad

Figure 39: Mobilization of temporalis muscle and exposure of zygomatic arch

Figure 40: Flap completely elevated from temporal fossa
Significant involvement of the infratemporal fossa (Figures 31, 32), cavernous sinus, or middle cranial fossa (Figure 33) requires infratemporal fossa or subtemporal approaches, often combined with an anterior approach. In order to reach the infratemporal fossa, one has to remove the zygoma, and reflect the temporalis muscle (Figures 33-36).
- The surgery is done via a hemicoronal incision commencing in a preauricular skin crease just below the level of the zygoma and placed behind the hairline for cosmetic reasons (Figure 37)
- Extend the incision to the temporalis fascia and elevate skin and subcutaneous tissue in the plane on the temporalis fascia (Figure 37)
- Elevation in this plane is stopped anteriorly when the superficial temporal fat pad with the facial/temporal branches of the facial nerve are encountered (Figures 37, 38)
- Incise the deep layer of deep temporalis fascia in a vertical direction at this point to expose the temporalis muscle
- Dissect anteriorly in a subfascial plane, deep to the fat pad up to the lateral orbital bony rim (anterior margin of temporal fossa)
- Next incise the temporalis fascia about 1 cm below the superior temporal line and from the posterior margin of the muscle, down onto the bone (leaving a cuff of fascia on bone permits subsequent suturing of muscle back to its original position)
- Identify the superior aspect of the zygomatic arch along its full length. This may require forceful inferior retraction of the soft tissues with a Langenbeck retractor (Figure 39)
- Incise the two layers of deep temporal fascia along the superior margin of the zygoma, and free the zygoma from the insertion of the masseter muscle
- Osteotomize and remove the zygomatic arch, and preserve it in saline so that it can be plated/wired back later in the procedure
- Elevate the temporalis muscle from the bone of the temporal fossa using either diathermy or a periosteal elevator while remaining hard on the bone (Figure 40)
- Extend the dissection medial to the coronoid process of the mandible that is now readily palpable; the coronoid process of the mandible can be divided and reflected inferiorly for additional exposure
References
- Herman P, Lot G, Chapot R, Salvan D, Huy PT. Long-term follow-up of juvenile nasopharyngeal angiofibromas: analysis of re-currences. Laryngoscope 1999; 109:140-7
- Pryor SG, Moore EJ, Kasperbauer JL. Endoscopic versus traditional approaches for excision of juvenile nasopharyngeal angiofibroma. Laryngoscope 2005; 115: 1201-7
- Schroth G, Haldemann AR, Mariani L, Remonda L, Raveh J. Preoperative embolization of paragangliomas and angiofibromas. Measurement of intratumoral arteriovenous shunts. Arch Otolaryngol Head Neck Surg 1996; 122:1320-5
- Lee JT, Chen P, Safa A, Juillard G, Calcaterra TC. The role of radiation in the treatment of advanced juvenile angiofibroma. Laryngoscope 2002; 112:1213-20
- Osborn AG. Radiology of the pterygoid plates and pterygopalatine fossa. AJR Am J Roentgenol 1979; 132:389-94
- Andrews JC, Fisch U, Valavanis A, Aeppli U, Makek MS. The surgical management of extensive nasopharyngeal angiofibromas with the infratemporal fossa approach. Laryngoscope 1989; 99:429-37
- Radkowski D, McGill T, Healy GB, Ohlms L, Jones DT. Angiofibroma. Changes in staging and treatment. Arch Otolaryngol Head Neck Surg 1996; 122:122-9
- Snyderman CH, Pant H, Carrau RL, Gardner P. A new endoscopic staging system for angiofibromas. Arch Otolaryngol Head Neck Surg 2010; 136:588-94
- Fagan JJ, Snyderman CH, Carrau RL, Janecka IP. Nasopharyngeal angiofibromas: selecting a surgical approach. Head Neck. 1997 Aug;19(5):391-9
- Lowlicht RA, Jassin B, Kim M, Sasaki CT. Long-term Effects of Le Fort I Osteotomy for Resection of Juvenile Nasopharyngeal Angiofibroma on Maxillary Growth and Dental Sensation. Arch Otolaryngol Head Neck Surg. 2002;128 (8):923-7
- Avelar RL, de Santana Santos T, Antunes AA, Dourado E Filho JRL. Horizontal Maxillary Osteotomy Approach for Resection of Juvenile Nasopharyngeal Angiofibroma. J Craniofac Surg 2011;22: 1027-30
Suggested video
Author
Derek J. Rogers, MD
Pediatric Otolaryngology
Harvard Medical School
Massachusetts Eye and Ear Infirmary, Boston, MA, USA
Derek_Rogers@meei.harvard.edu
Christopher J. Hartnick, MD, MS Epi, Professor
Department of Otolaryngology Division
Director, Pediatric Otolaryngology
Harvard Medical School Massachusetts Eye and Ear Infirmary
Boston, MA, USA
Christopher_Hartnick@meei.harvard.edu
Author & Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za