
5.3: Buccal Fat Pad Flap
- Page ID
- 15456

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
BUCCAL FAT PAD FLAP
Johan Fagan
The buccal fat pad flap is an axial flap and may be used to fill small-to-medium sized soft tissue and bony defects in the palate, superior and inferior alveoli and buccal mucosa. It is often encountered as it bulges into the surgical field during surgery in the pterygomandibular region.
Relevant Anatomy
Buccal fat pad
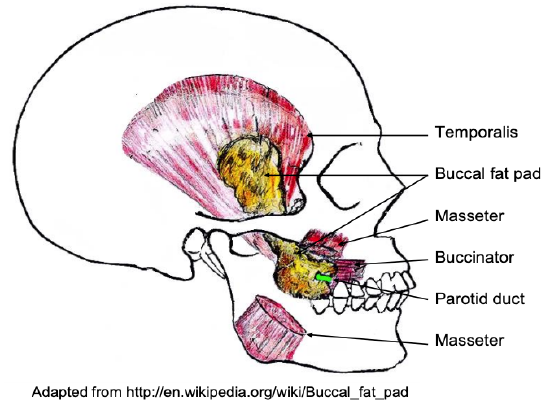
Figure 1: Buccal fat pad
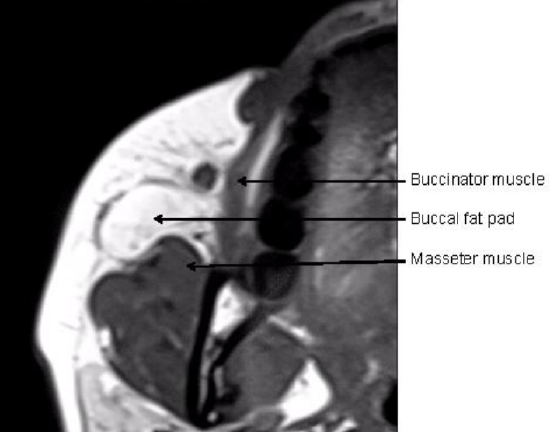
Figure 2: MRI (axial view) illustrating the anatomical relationship of the buccal fat pad to masseter and buccinator muscles
The buccal fat pad (Figure 1) is an encapsulated, mass of specialized fatty tissue, the volume of which varies throughout life. It is distinct from subcutaneous fat (Figure 2). It fills the deep tissue spaces and acts as gliding pads when masticatory and mimetic muscles contract, and cushions important structures from forces generated by muscle contraction.
The parotid duct passes along the lateral surface or penetrates the body of the fat pad before traversing the buccinator muscle and entering the oral cavity (Figure 1). It is attached by six ligaments to the maxilla, posterior zygoma, inner and outer rims of the infraorbital fissure, temporalis tendon, and buccinator membrane.
The buccal fat pad has a body and four processes. The body is located behind the zygomatic arch. The body is divided into 3 lobes – anterior, intermediate and posterior, in accordance with the structure of the lobar envelopes, the ligaments and the feeding vessels. The anterior lobe is located below the zygoma, and extends to the front of the buccinator, maxilla and the deep space of the quadrate muscle of the upper lip and zygomaticus major muscle. The canine muscle originates from the infraorbital foramen and passes through the medial part of the anterior lobe. The parotid duct passes through the posterior part, and the anterior facial vein passes through the anteroinferior margin. The anterior lobe also envelopes the infra-orbital vessels and nerve, and together enters the infraorbital canal. The branches of the facial nerve lie on the outer surface of its capsule. The intermediate lobe is situated in and around the posterior lobe, lateral maxilla and anterior lobe. It is a membrane-like structure with thin fatty tissue in adults, but is a prominent mass in children. The posterior lobe is situated in the masticatory and neighboring spaces. It extends up to the inferior orbital fissure and surrounds the temporalis muscle, and extends down to the superior rim of the mandibular body, and back to the anterior rim of the temporalis tendon and ramus. In doing so it forms the buccal, pterygopalatine and temporal processes.
Four processes (buccal, pterygoid, superficial and deep temporal) extend from the body into surrounding spaces such as the pterygomandibular and infratemporal fossae.
Blood supply
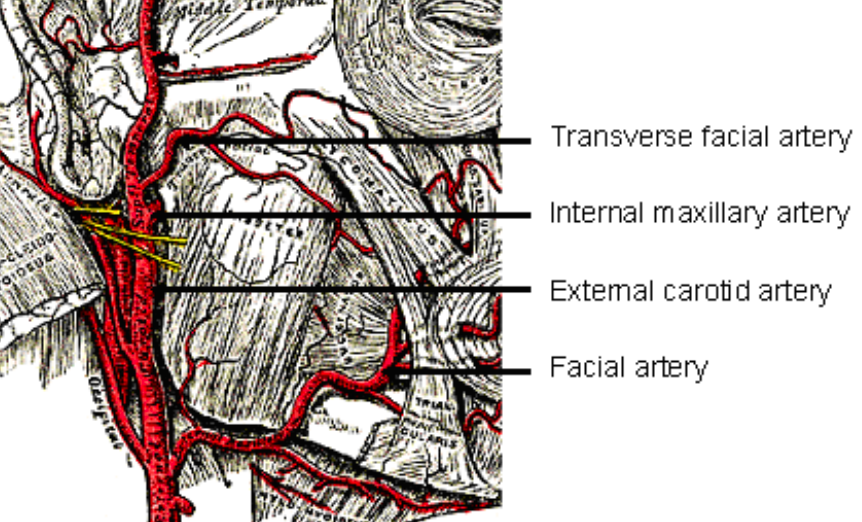
Figure 3: Blood supply to buccal fat pad
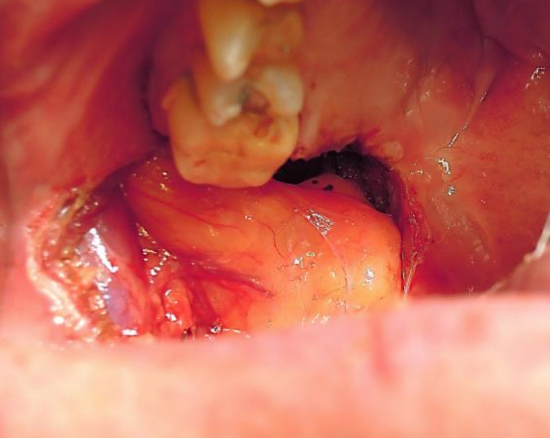
Figure 4: Note the clearly visible vascular supply to the flap
The buccal fat pad flap is an axial flap. The facial, transverse facial and internal maxillary arteries and their anastomosing branches enter the fat to form a sub-capsular vascular plexus (Figures 3, 4).
Indications

Figure 5: The buccal fat pad can be rotated to cover a variety of defects
- Reconstruction of small to medium (<5 cm) congenital or acquired soft tissue and bony defects in the oral cavity. This includes oronasal and oroantral communications following dental extraction; surgical defects following tumor excision, excision of leukoplakia and submucous fibrosis; and primary and secondary palatal clefts (Figure 5)
- Coverage of exposed maxillary and mandibular bone or bone grafts and bone flaps
- Alternative or backup for failed buccal advancement flaps, palatal rotation and transposition flaps, tongue and nasolabial flaps, and radial free forearm flaps.
Surgical Steps
- Surgery may be done under local or general anesthesia

Figure 6: Position of fat pad relative to parotid duct
- Three approaches (Figure 6)
- Incise buccal mucosal membrane 1 cm below the opening of parotid duct (Matarasso’s method)
- Incise behind the opening of parotid duct (Stuzin’s method)
- Incise superior gingivobuccal sulcus
- Cut through the buccinator muscle with diathermy and dissect bluntly until the buccal fat pad is found
- Incise the thin capsule of the buccal fat pad
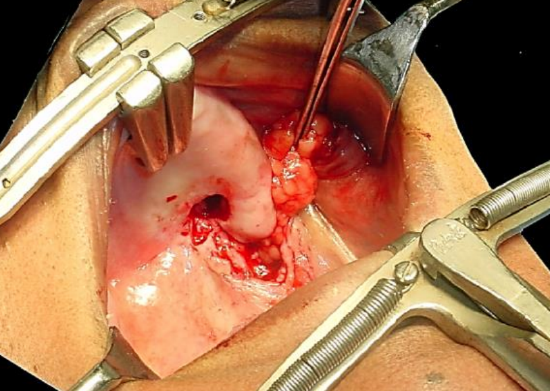
Figure 7: Careful delivery of fat pad after incising the capsule
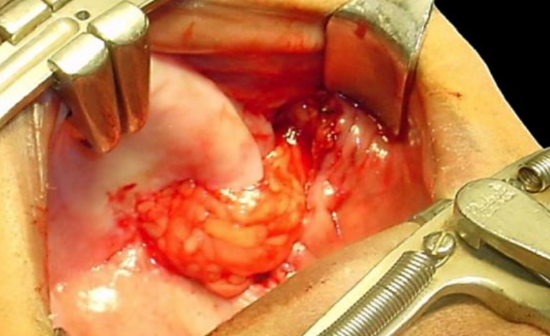
Figure 8: Flap placed over an oronasal defect
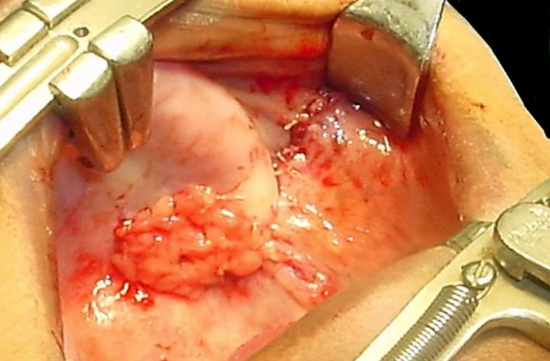
Figure 9: Flap sutured to defect, and pedicle covered with mucosa

Figure 10: Mucosalized flap approximately a month postoperatively
- Gently deliver the required volume of buccal fat tissue into oral cavity by gentle to-and-fro traction on the buccal fat, so as not to disrupt the blood supply and hence devascularize the flap (Figure 7)
- Take care not to injure the inferior buccinator branches of facial artery so as to avoid causing a hematoma
- Freshen the edges of the recipient site
- Position the buccal fat pad flap in defect and secure it with absorbable sutures (Figures 8, 9)
- Cover the flap with mucosa if feasible (Figure 9)
- Await epithelialization of the flap which usually occurs within 1 month (Figure 10)
Complications
Complications rarely occur and may include partial necrosis and excessive scarring. With large flaps used for buccal defects there is a risk of fibrosis and trismus.
Clinical examples
Case 1: Interalveolar carcinoma resected with exposed vertical ramus of mandible
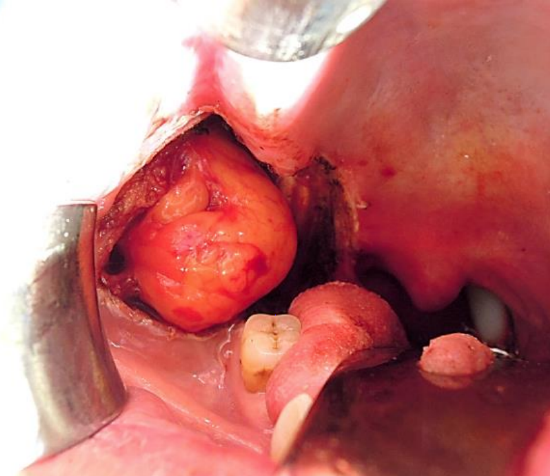
Figure 11a: Buccal fat pad adjacent to interalveolar defect
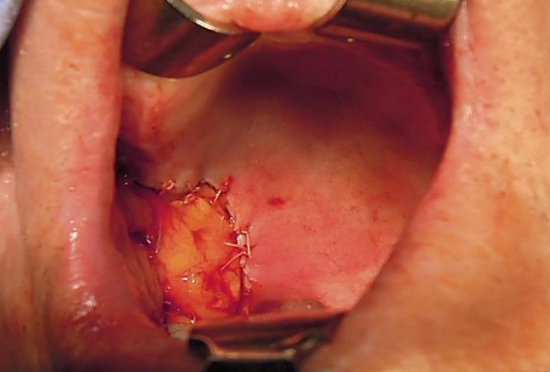
Figure 11b: Defect filled with buccal fad pad
Case 2: Mucoepidermoid carcinoma resected at junction of hard and soft palate
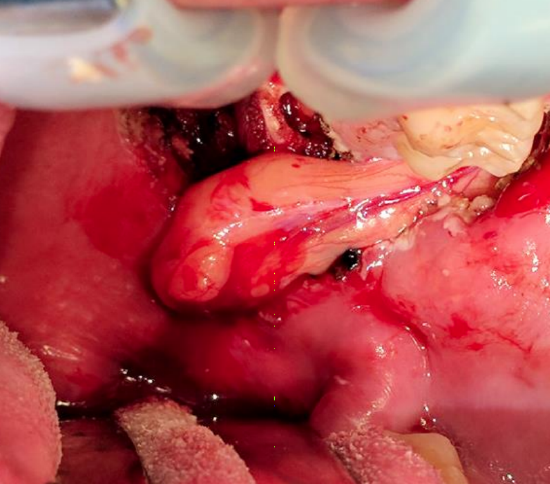
Figure 12a: Buccal fat pad adjacent to palatal defect, illustrating the vascular pedicle

Figure 12b: Defect filled with buccal fad pad; note vascular pedicle
Summary
The buccal fat pad is a simple, reliable flap for repair of small-to-medium sized oral defects. It has an excellent blood supply and causes minimal donor site morbidity.
Other flaps described in The Open Access Atlas of Otolaryngology Head & Neck Operative Surgery
- Pectoralis major flap
- Buccinator myomucosal flap
- Nasolabial flap
- Temporalis muscle flap
- Deltopectoral flap
- Paramedian forehead flap
- Upper and lower trapezius flaps
- Cervicofacial flaps
- Submental artery island flap
- Supraclavicular flap
- Latissimus dorsi flap
- Local flaps for facial reconstruction
- Radial free forearm flap
- Free fibula flap
- Rectus abdominis flap
- Anterolateral free thigh flap
- Thoracodorsal artery scapular tip (TDAST) flap
- Principles and technique of microvascular anastomosis for free tissue transfer flaps in head and neck reconstructive surgery
Author & Editor
Johan Fagan MBChB, FCS (ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za