
5.13: Latissimus Dorsi Flap for Head and Neck Reconstruction
- Page ID
- 53284

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
LATISSIMUS DORSI FLAP FOR HEAD AND NECK RECONSTRUCTION
Patrik Pipkorn, Ryan Jackson, Bruce Haughey

Figure 1: Large pedicled latissimus dorsi flap
The latissimus dorsi is the largest muscle in the body by surface area. It can be as large as 20 x 40 cm, enabling latissimus dorsi flaps to cover very large defects (Figure 1).
The flap can be harvested as a pedicled or free flap and as a muscular or myocutaneous flap with an overlying skin paddle. It can also be harvested along with any other flap based on the subscapular vascular system as a chimeric or subscapular “megaflap”. Despite its size it can be harvested without significant donor site morbidity.
The muscle is normally about 1 cm thick. Because it atrophies significantly if it is not reinnervated, it is a popular option for scalp reconstruction and for other defects in the head and neck area including reconstruction of skull base and total glossectomy defects.
Benefits
- Easy flap to learn to harvest
- Large thin muscle that can cover very large defects
- Long (5-15 cm) vascular pedicle if dissected up to the subscapular artery
- The subscapular artery has a diameter of 2-5 mm
- Minimal long-term donor site morbidity
- Can be harvested as a muscle flap or with a skin paddle
- Can be harvested as a chimeric flap (multiple otherwise independent flaps that each have an independent vascular supply with all pedicles linked to a common source vessel) along with other flaps based on a singular subscapular artery
Caveats
- Donor site is close to head and neck area making two team harvest difficult, though not impossible
- Because the donor site is on the back, it makes positioning more tedious
- Large wound and potential dead space after harvest has high risk of a seroma
Surgical anatomy
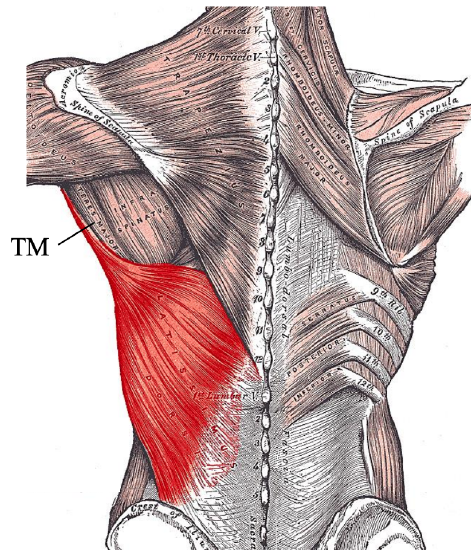
Figure 2: Posterior view of Latissimus dorsi muscle and Teres major (TM)
The latissimus dorsi mainly adducts and medially rotates the arm. It also rotates the shoulder inferiorly and posteriorly. It is a thin, flat muscle measuring about 20 x 40 cm (Figure 2). The muscle forms the posterior axillary fold together with the teres major muscle (Figure 2). It originates from the posterior iliac crest, the thoracolumbar fascia and spinous processes of T7- L5. Some muscle fibers may also originate from the lower ribs.
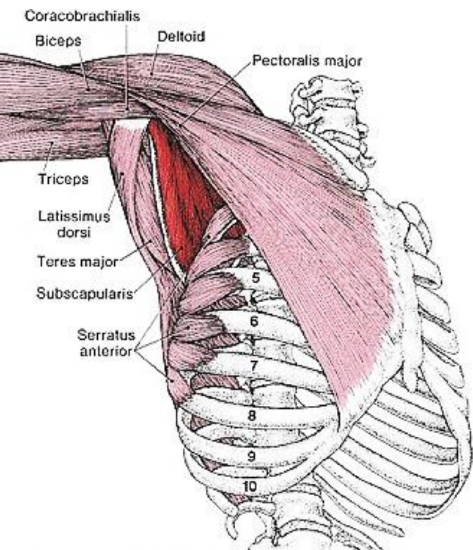
Figure 3: Anterolateral view of latissimus dorsi, teres major, serratus anterior, and pectoralis major
The muscle fibers run in a superolateral direction and insert into the floor of the intertubercular groove of the humerus between the teres major and pectoralis major muscles (Figure 3).
Some fibers also variably originate from the tip of the scapula where they intersperse with fibers of the teres major. Superomedially it lies deep to the trapezius muscle as the trapezius attaches all the way down to T12. Inferiorly it covers the serratus anterior and external oblique abdominis muscles (Figure 3).
Innervation
The latissimus dorsi is innervated by the thoracodorsal nerve. It is derived from the 6th, 7th and 8th cervical nerve roots and arises from the posterior cord of the brachial plexus. The nerve runs with the thoracodorsal vascular pedicle. It only innervates the latissimus dorsi, so no other muscles are affected despite its transection when harvesting the flap.
Vascular anatomy
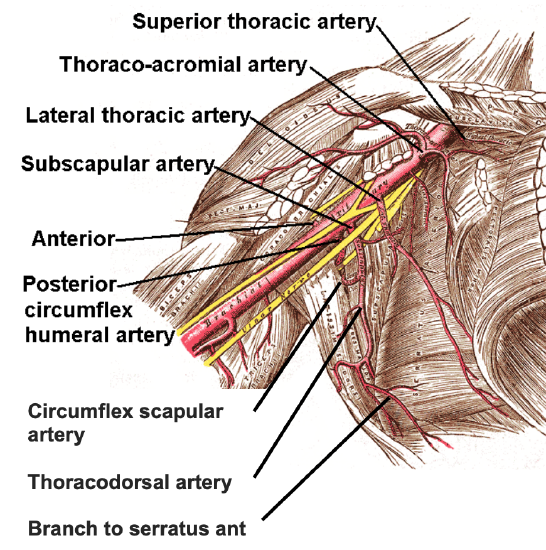
Figure 4: Anterolateral view of vascular anatomy; the subscapular artery is the largest of 3 branches of the third segment of the axillary artery
The thoracodorsal artery is the main blood supply to the latissimus dorsi; it is a terminal branch of the subscapular system (Figure 4). A sound understanding of the subscapular artery system is therefore important for a microvascular surgeon when harvesting flaps from the back. The subscapular artery is a very versatile system that supplies many flaps that can be harvested alone or as chimeric flaps with different tissues based on a single pedicle.
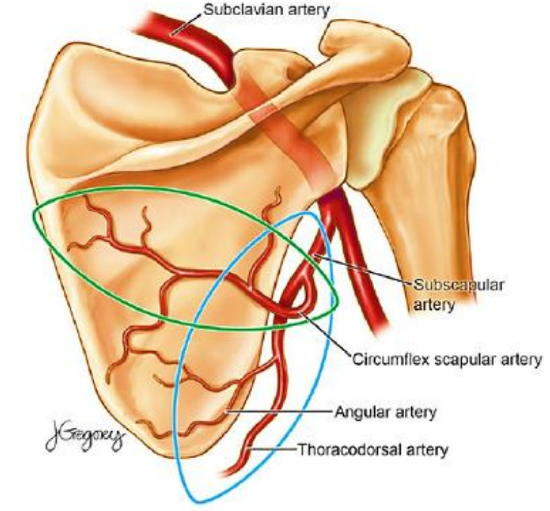
Figure 5: Subscapular artery and its branches depicted from posteriorly
The subscapular artery is a branch of the 3rd segment of the axillary artery after the axillary artery has crossed the pectoralis minor. The branching patterns of the subscapular system varies considerably. The subscapular artery divides into the circumflex scapular (CSA) and thoracodorsal arteries (Figure 4). The CSA continues from deep to superficial in the triangular space between the teres major, teres minor, the long head of the triceps and the lateral border of the scapula. After passing through this triangular space, the CSA divides into a horizontal and a vertical terminal branch, both which can be used for cutaneous flaps (Figure 5).
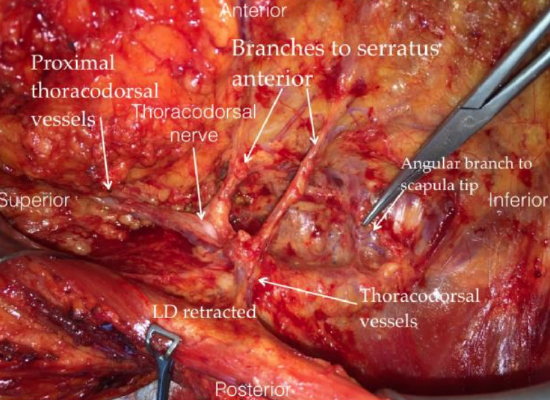
Figure 6: Right anterolateral view with latissimus dorsi (LD) retracted to demonstrate thoracodorsal vessels, nerve and branches to serratus anterior
The thoracodorsal artery continues deep to the teres major and latissimus dorsi muscle along the thoracic wall (Figure 4). There is some variability of the branching pattern but most often a separate branch, the angular branch, arises from the thoracodorsal artery and supplies the tip of the scapula (Figures 5, 6). Before entering the latissimus dorsi muscle a 2nd branch, the branch to serratus anterior muscle, branches off (Figures 4, 6).
Blood supply to latissimus dorsi muscle
The thoracodorsal artery provides the main blood supply to the latissimus dorsi. The thoracodorsal artery and vein course superiorly along the thoracic wall on the deep surface of the latissimus dorsi towards the axilla. The artery is 1.5 - 4 mm in diameter and the vein is usually 2.5 - 4.5mm in diameter. The muscular pedicle can be between 6-16 cm in length with an average length of 9 cm. It enters the muscle on its deep surface about 8-10 cm distal to its origin of the subscapular artery (Figure 6). To gain extra length, the artery can be dissected all the way to the axillary artery.
Just after the thoracodorsal artery enters the muscle it divides into two branches, one horizontal and one vertical enabling two different skin paddles to be harvested with the flap. The highest density of perforators is about 2 cm posterior to the anterior edge of the muscle, just after the artery enters the muscle. As with a pectoralis major flap these perforators are small and are not routinely dissected when harvesting the flap. To ensure incorporation of perforators into the flap, a Doppler can be used, although it is not essential to do so. Designing a larger skin paddle also makes the flap more reliable as the chance of incorporating perforator vessels increases.
The muscle also receives blood supply from segmental perforating vessels from thoracic and lumbar intercostal arteries. These arteries are small and enter the muscle on its deep surface close to the spine. They supply the medial and inferior extensions of the muscle. Since these vessels are transected during flap harvest, the blood supply to the distal 1/3 of the muscle may be unreliable.
Informed consent
Preoperative discussion should include the risk of hematomas and seromas and developing an unsightly scar. Patients must be counseled about the risk of flap failure. Shoulder strength might be slightly affected, though not noticeably in most patients unless combined with other flaps that may affect shoulder strength e.g. pectoralis major or scapular flaps.
Positioning and draping
The classic way to position a patient for any of the flaps based on the subscapular system is to expose the full back of the patient by placing the patient in a lateral decubitus position with an axillary roll. This however makes it necessary to rotate the patient between the ablative and the flap harvesting stages, which requires repositioning and redraping, and adds considerable time and effort to the surgery.

Figure 7: Positioning to permit simultaneous cancer resection and harvesting of latissimus dorsi flap (Courtesy Jason Rich)
However, as the surgical incision is made on the lateral back and at no time during the surgery exposure is necessary beyond the midline, it is possible to put the patient in a 30-45 degree angle with the patient’s contralateral side supported with a deflatable beanbag (Figure 7). Once the patient is properly secured to the bed, the bed can be rotated back by about 15-20 degrees permitting adequate exposure for both the ablative and reconstructive surgeons. This positioning technique saves considerable time and circumvents one of the major drawbacks of harvesting flaps from the back, namely, time-consuming repositioning, reprepping and redraping.
Key points for this positioning technique
- Once the patient is intubated and all the necessary intravenous and arterial lines, urinary catheter, and ECG leads have been placed, place the patient on a bean bag (Figure 7)
- Rotate the patient about 30-45 degrees to facilitate exposure of the back which will be used for the harvest (Figure 7)
- Deflate the bean bag to make a firm and stable base to hold the patient in position
- Expose the back up to the spinous processes
- Take care to pad any firm spots to minimize risks of pressure necrosis

Figure 8: The knee is kept slightly bent and a pillow is placed to minimize any pressure on bony prominences
- Place a pillow between the knees, which should be slightly bent (Figure 8)

Figure 9: The lower arm is bent slightly and is padded well. Note that patient is well secured to the bed (Courtesy Jason Rich)
- Gently bend the contralateral arm with padding placed between the arm and the chest; a formal axillary roll is not required (Figure 9)
- Properly secure the patient to the bed with belts and tape so that the bed can be tilted, and the patient remains secure (Figure 9)
- Before prepping, perform a “tilt test” to make sure the patient is secure
Flap design
- Decide whether a skin paddle is required to reconstruct the surgical defect
- If a skin paddle is needed, it must be located over the latissimus dorsi muscle
- In general, a width of 10 cm can easily be harvested, still allowing the defect to be closed primarily; a simple “pinch test” will give one some indication
- A larger skin paddle tends to be more reliable as more perforators entering from the deep surface are incorporated
The latissimus dorsi flap may be employed either as a free microvascular transfer flap or a pedicled flap.
Surgical steps
In the following presentation, a muscleonly free flap is raised.

Figure 10: The patient is prepped with the arm free draped (Courtesy Jason Rich)

Figure 11: A sleeve is placed over the distal arm and hand. This sleeve can be secured to the drapes during the resection stage to ensure it does not fall off the table. Expose the back from the spinous processes medially, to the iliac bone below

Figure 12: Start by feeling for the posterior axillary fold (teres major and latissimus dorsi)
- Prep the back up to the spine and include ipsilateral arm (Figure 10)
- Put a stocking over the arm and secure it to the drapes; being able to move the arm greatly increases the exposure when dissecting the pedicle into the axilla (Figure 11)
- Identify the anterior edge of the latissimus dorsi
- This is done by identifying the posterior axillary fold (Figure 12)
- The posterior axillary fold consists of teres major and the latissimus dorsi

Figure 13: When a skin paddle is not needed, a lazy S incision is placed along the anterior border of latissimus dorsi. The position where the thoracodorsal artery pierces the muscle from the deep aspect is marked (X) as well as the vertical and horizontal branches (dotted lines)

Figure 14: Incise skin and subcutaneous tissue all the way down to the latissimus muscle
- Design a lazy-S shaped incision a few centimeters behind the anterior edge of the muscle (Figure 13)
- Incise the skin and subcutaneous tissue (Figure 14)
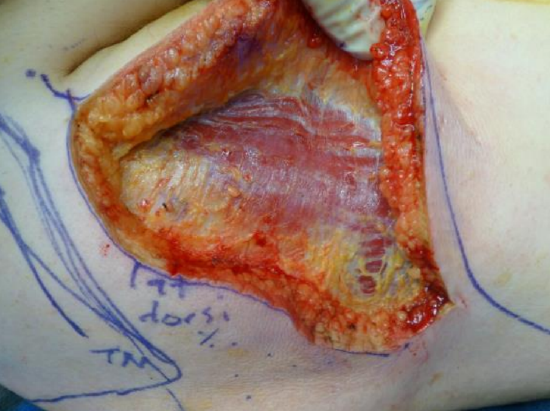
Figure 15: Latissimus muscle exposed
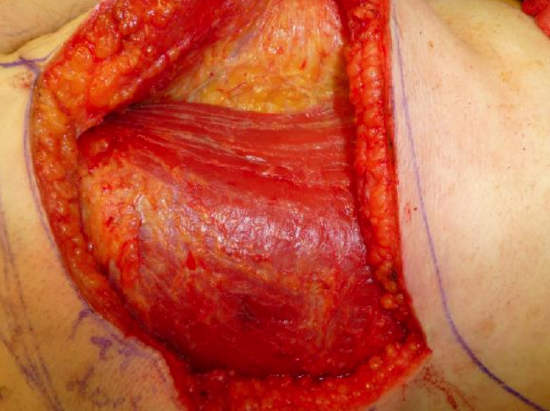
Figure 16: Identify anterior border of latissimus dorsi
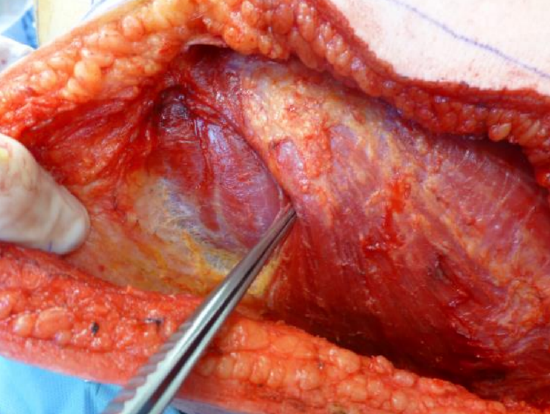
Figure 17: Continue dissecting superiorly and identify the posterosuperior border. This border is much more tedious to find as fibers intersperse with teres major muscles and some fibers attach to the scapula
- Extend the incision down to the muscle (Figure 15)
- Raise the anterior flap until the anterior edge of the latissimus dorsi muscle is identified (Figure 16)
- Now raise the flap posteriorly
- Superiorly this edge can be a little tedious to identify where the latissimus dorsi intersperses with the fibers of the teres major muscle (Figure 17)
- Once these landmarks have been identified the entire surface of the muscle is exposed using electrocautery as there are no major structures in this area that can be injured
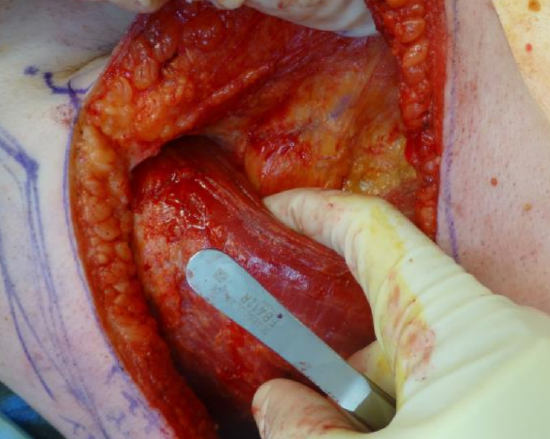
Figure 18: With blunt finger dissection you can now further identify the anterior border and start separating the muscle from the chest wall
- Dissect the latissimus dorsi muscle off the thoracic wall using blunt finger dissection (Figure 18)
- Superiorly this dissection plane consists of loose areolar tissue which makes it easy to strip the latissimus dorsi from the underlying tissues
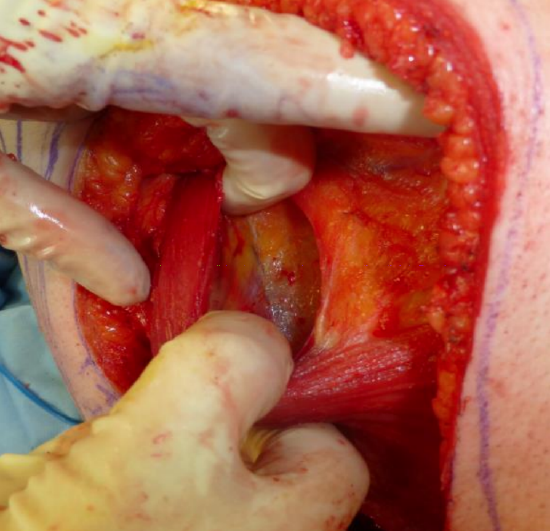
Figure 19: Identify the thoracodorsal pedicle as it pierces the deep aspect the muscle
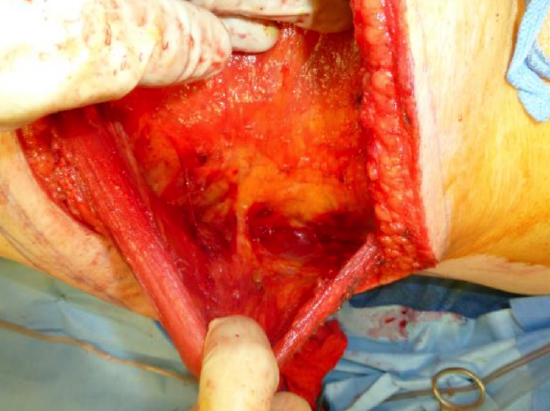
Figure 20: The remainder of the latissimus dorsi muscle is now exposed; this can be done quickly as there is nothing to hurt superficial to the muscle. The muscle is elevated off the chest wall. Inferiorly the muscle fibers intersperse with serratus and abdominal wall muscles
- By doing this maneuver, the pedicle should become visible as it enters the muscle on its deep aspect, superiorly (Figure 19)
- Having identified the pedicle, dissect the muscle off the thoracic wall in a proximal-to-distal fashion (Figure 20)
- Be sure to control small perforating vessels that enter the muscle from the thoracic wall
- The muscle does not separate as easily inferiorly as it attaches to the abdominal wall and intersperses with serratus anterior and external oblique muscle fibers
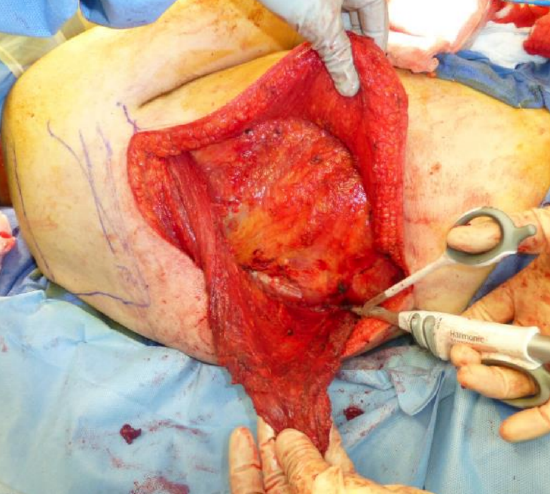
Figure 21: Start by dividing the muscle inferiorly, in this case with a harmonic scalpel, and then along the spinous processes
- Once the whole muscle is exposed as well as separated from the thoracic wall, the muscle is divided inferiorly (Figure 21)
- Once the inferomedial point is reached continue to free it medially along the spine (Figure 21)

Figure 22: Continue up along the spinous processes until the whole muscle is released
- Continue upward along the spinous processes until the entire muscle is released. Ensure good hemostasis as you encounter the spinous perforators (Figure 22)
- Superiorly the most medial aspect of the muscle may be obscured by the inferior aspect of trapezius muscle
- If the flap is to be used as a free flap, then it is advisable to delay dividing the humeral attachment of the latissimus dorsi until very late as this takes the weight off the flap when dissecting the pedicle, thus avoiding traction injury to the vessels
- The pedicle is now easily visualized
- Commence dissection of the pedicle
- Having someone lift the arm perpendicularly to the floor greatly facilitates the axillary exposure at this stage
- Expose the thoracodorsal artery as far proximally as needed for adequate vessel length
- To maximize the length of the pedicle, the artery can be traced to the axillary artery
- Significant vessel variability exists in this region
- To obtain maximum pedicle length the serratus branch as well as the circumflex vessels generally have to be divided if they are not necessary for other components of the subscapular system of flaps

Figure 23: Free flap with vascular pedicle
- Divide the pedicle and harvest the flap once donor vessels have been prepared (Figure 23)
- Before dividing the vessels, the thoracodorsal nerve which runs with the pedicle must be divided
- Before closing the defect, assure excellent hemostasis is achieved

Figure 24: The back is closed in layers after hemostasis has been achieved. Two large suction drains are placed and are left in for about 2 weeks
- Insert 2 large suction drains left in situ for 2 weeks (Figure 24)
- Close the skin in layers
- Sutures or staples are generally removed at 2 weeks
Postoperative care
The patient is encouraged to mobilize the arm postoperatively. The drains are left in place until the output has diminished. This may take up to 1-2 weeks as the surgical wound and the potential dead space is very large, leading to a high risk of postoperative seroma formation.
Latissimus dorsi pedicled regional flap
The latissimus dorsi flap may also be employed as a pedicled flap, and can reach as high as the temporal region or even the vertex if the skin paddle is placed caudally enough. Success rates of 90-95% have been reported for pedicled latissimus dorsi flaps.
Indications for pedicled as opposed to free latissimus dorsi flaps include:
- A vessel-depleted neck where the patient’s anatomy, previous surgery and/or irradiation may not offer safe options for microvascular anastomosis
- A patient’s general health does not permit additional time and risk associated with a microvascular free flap
- Microsurgical expertise is unavailable
Surgical steps
- If the flap is to be harvested as a regional pedicled flap, then the muscle is rotated up towards the head and neck area through a tunnel that is created between the pectoralis major and pectoralis minor muscles. The humeral attachment can then be left intact unless extra length is necessary and to create a gentler bend to the pedicle
- Raise the latissimus dorsi flap using the same surgical steps as described above for a free flap
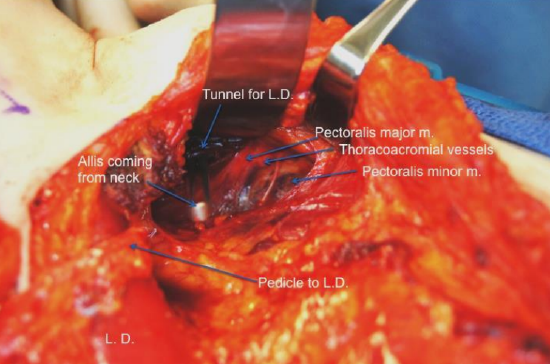
Figure 25: Tunnel between the pectoralis minor and pectoralis major muscles for the flap to be passed from the axilla into the neck (Courtesy Ralph Gilbert)
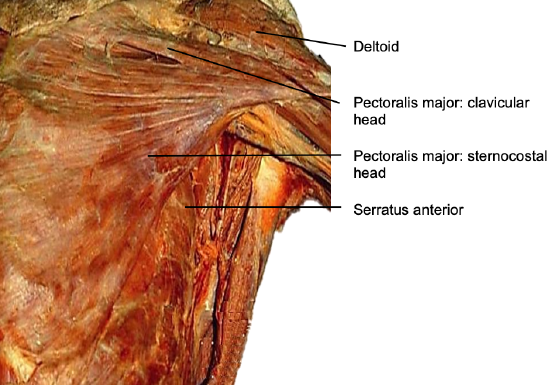
Figure 26: Pectoralis major and clavicular head
- Create a tunnel between the pectoralis minor and pectoralis major muscles for the flap to be passed from the axilla into the neck (Figure 25)
- Expose the lateral border of the pectoralis major muscle as when raising a pectoralis major flap (Figure 26)
- Separate the pectoralis major from the pectoralis minor by stripping with a finger in the loose areolar plane between the two muscles
- Cut across approximately 5 cm of the broad clavicular insertion of the pectoralis major with electrocautery to create a tunnel between the undersurface of the pectoralis major and the skin overlying the clavicle
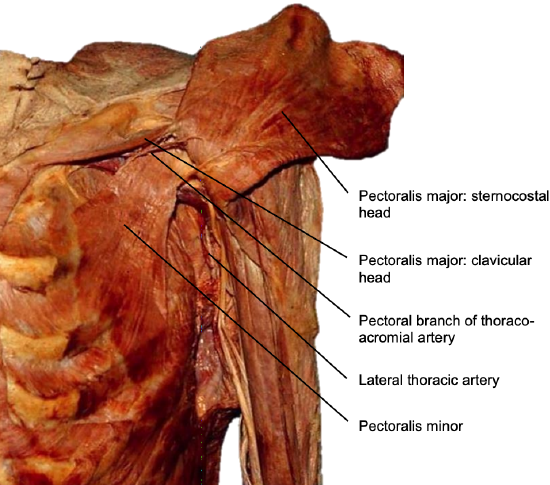
Figure 27: Deep relations of pectoralis major muscle; note pectoral branch of the thoracoacromial artery and the lateral branches to the pectoralis major from lateral thoracic vessels
- Take care to remain lateral to the pectoral branch of the thoraco-acromial artery in order to preserve the pedicle to the pectoralis major, thus keeping this flap as a later option (Figure 27)
- Lateral branches to the pectoralis major from the lateral thoracic vessels may have to be sectioned during this procedure (Figure 27)
- The remainder of the tunnel can now be created subcutaneously from the neck down towards the anterolateral aspect of the clavicle
- Dissect the pedicle of the latissimus dorsi flap towards the circumflex vessels
- Do not divide these vessels to ensure a gentle arc of the flap vessels as they are turned 180 degrees to reach the neck
- The proximal portion of the tendinous part of the humeral head, up to where the thoracodorsal vessels enter the flap, can be removed to reduce bulk that may compress the pedicle in the tunnel
- Once the flap is delivered, ensure that the flap vessels are gently curved and that the tunnel is wide enough to not exert any pressure on the pedicle
Flap variations
Different variations of the flap can be considered. The latissimus flap can be done as a chimeric flap as part of the subscapular system, in combination with tissue based on circumflex scapular vessel or serratus branches or can be raised alone. The flap can be tailored to the needs of the recipient defect. The flap can be harvested as a whole or partial muscle. The flap can be harvested as a myocutaneous flap with overlying skin. The flap can even be harvested as a bony flap with underlying 9th or 10th rib. Great care then needs to be taken to not injure underlying pleura or transect the muscular attachments to the rib that supply periostal blood supply to the harvested rib.
Clinical examples
Resurfacing of neck with pedicled latissimus dorsi flaps

Figure 28: Courtesy Ralph Gilbert

Figure 29: Resurfacing of neck with pedicled latissimus dorsi flap for brachytherapy following prior irradiation
Reconstruction of total glossectomy defect with a hypoglossal to thoracodorsal neuroraphy

Figure 30: Flap design with bulk of skin overlying entry point of thoracodorsal artery
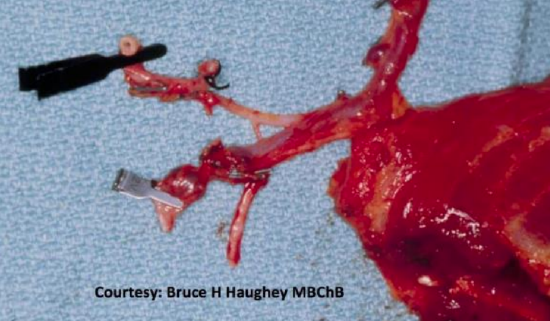
Figure 31: Flap with thoracodorsal vessels and thoracodorsal nerve
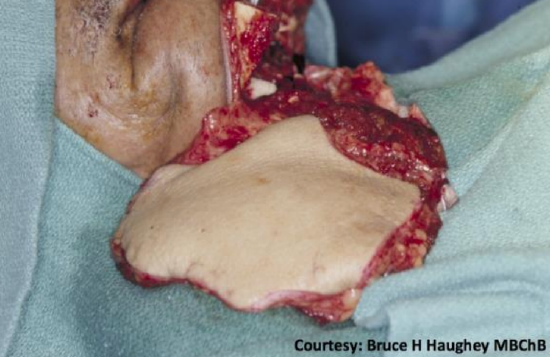
Figure 32: Flap anastomosed to facial vessels and neuroraphy performed to left hypoglossal nerve

Figure 33: De-epithelization of anterior portion and suturing of both epithelial borders help creating an anterior dome

Figure 34: Immediate postoperative result
Myocutaneous flap for scalp defect

Figure 35: Surgical defect after recurrent cutaneous squamous cell carcinoma after failed radiation

Figure 36: Flap design

Figure 37: Muscle sutured to skin island to protect vascularity to flap
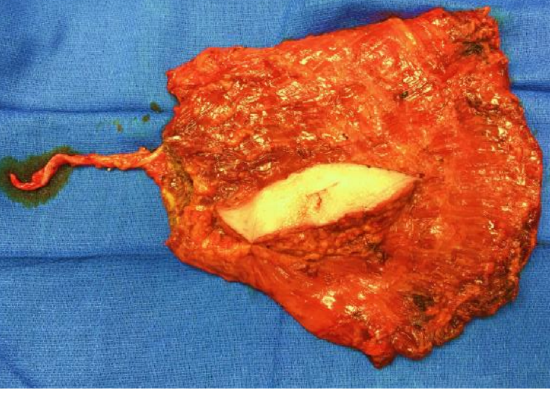
Figure 38: Flap harvested with an intraoperative monitor paddle (skin was later discarded)
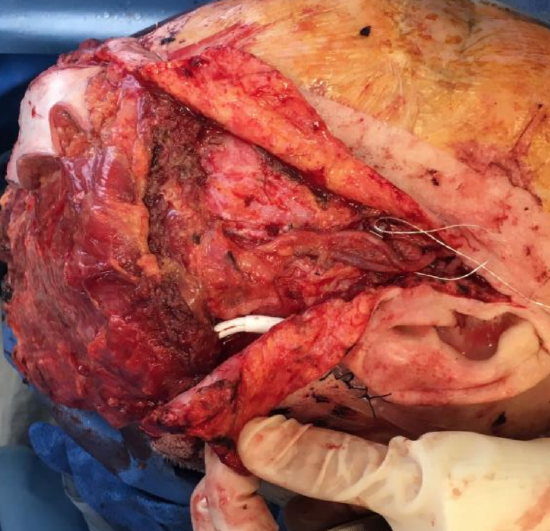
Figure 39: Vascular anastomosis to superficial temporal vessels; the facial vessels can often be used

Figure 40: Flap in place
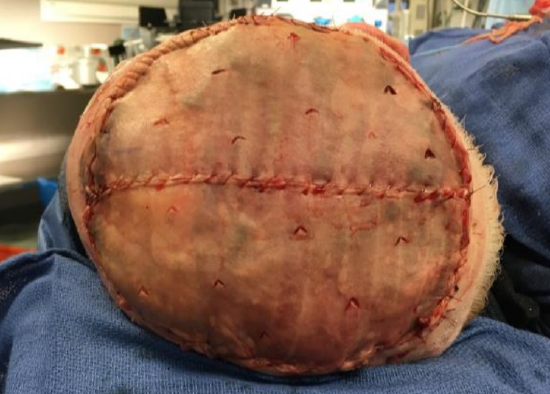
Figure 41: Split thickness skin graft covering muscle flap

Figure 42: Two months postop; note marked atrophy of the muscle, closely resembling the natural thickness of the native scalp
Other flaps described in The Open Access Atlas of Otolaryngology Head & Neck Operative Surgery
- Pectoralis major flap
- Buccinator myomucosal flap
- Buccal fat pad flap
- Nasolabial flap
- Temporalis muscle flap
- Deltopectoral flap
- Paramedian forehead flap
- Upper and lower trapezius flaps
- Cervicofacial flaps
- Submental artery island flap
- Supraclavicular flap
- Local flaps for facial reconstruction
- Radial free forearm flap
- Free fibula flap
- Rectus abdominis flap
- Anterolateral free thigh flap
- Thoracodorsal artery scapular tip (TDAST) flap
- Principles and technique of microvascular anastomosis for free tissue transfer flaps in head and neck reconstructive surgery
Authors
Patrik Pipkorn MD, Assistant Professor
Head & Neck Microvascular Reconstruction
Department of Otolaryngology, Head and Neck Surgery
Washington University
St Louis, MO, USA
patrikpipkorn@hotmail.com
Ryan Jackson MD Assistant Professor
Head & Neck Microvascular Reconstruction
Department of Otolaryngology, Head and Neck Surgery
Washington University
St Louis, MO, USA
jacksonrs@wustl.edu
Bruce Haughey MBChB, MS, FRACS FACS
Head & Neck Oncologic & Reconstructive Surgeon
Florida ENT Surgical Specialists
Florida Hospital Celebration Health
Celebration, FL USA
bruce.haughey.md@flhosp.org
Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za