
5.14: Submental Artery Island Flap Technique for Head and Neck Reconstruction
- Page ID
- 53286

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
SUBMENTAL ARTERY ISLAND FLAP FOR HEAD & NECK RECONSTRUCTION
Johan Fagan, Tareck Ayad, Mohammad Alfalasi

Figure 1: Submental island flap
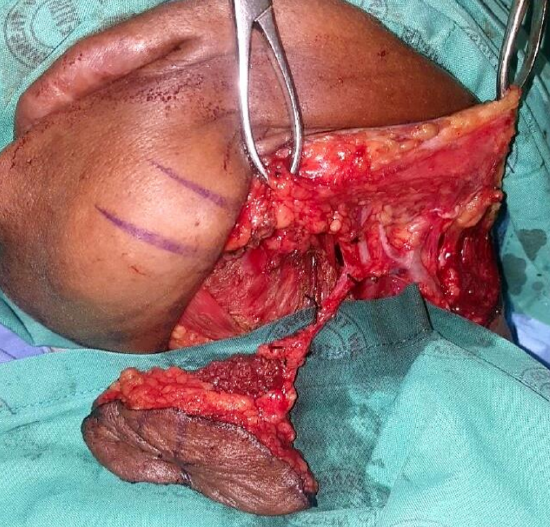
Figure 2a: Submental island flap including the anterior belly of digastric
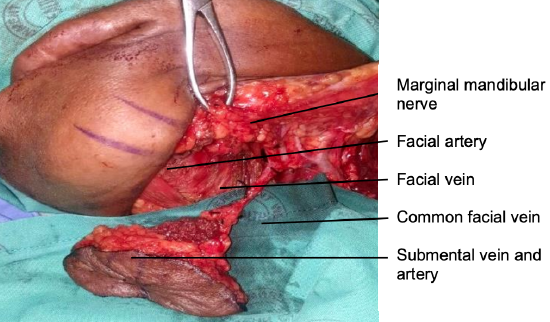
Figure 2b: Anatomy of veins, arteries and marginal mandibular nerve
The submental artery island flap (SIF) is an axial fasciocutaneous flap that includes skin, subcutaneous tissue, platysma, and fat and is pedicled on the submental artery and veins (Figures 1, 2).
The vascular pedicle has a length of up to 8 cm. It may be used for facial, oral cavity, oro- and hypopharyngeal soft tissue defects. If it is further dissected to its origin from the facial artery, the pedicle can be lengthened by an additional 1-2 cm to reach the lateral canthus and zygomatic arch.
Regional flaps like the SIF have distinct advantages over free tissue transfer flaps for selected soft tissue defects in the head and neck such as reduced operating time, donor site morbidity, level of surgical expertise required, and cost. Other regional flaps that may be considered for the oral cavity and pharynx include the buccinator, nasolabial, temporalis muscle, pectoralis major, and supraclavicular flaps.
Surgical anatomy
Submental island
The submental artery supplies a large skin paddle of as much as 10 x 16 cm, extending from one angle of the mandible to the other. The flap comprises skin, subcutaneous fat, platysma muscle, submental fat, and lymph nodes; the anterior belly of digastric and mylohyoid muscles may also be included. The entire flap can be pedicled on one submental artery because of crossover perfusion between the left and right submental arteries. The maximum anteroposterior dimension of the skin island is limited by the ability to achieve primary closure; this in turn depends on skin laxity and age.
Facial artery (Figures 2, 3, 4)
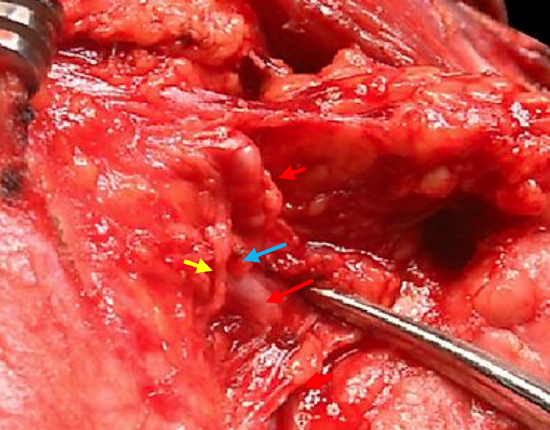
Figure 3: The right submandibular gland has been dissected in a subcapsular plane; the marginal mandibular nerve (yellow arrow) is seen crossing the facial artery (red arrows) and divided vein (blue arrow)
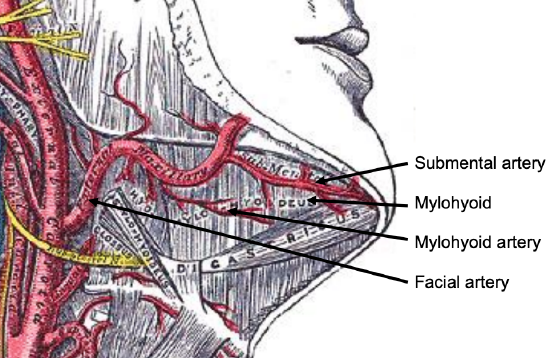
Figure 4: Submental, facial and mylohyoid arteries, and mylohoid muscle and anterior belly of digastric
The facial artery emerges from behind the posterior belly of the digastric muscle, and courses along the posterior surface of the submandibular salivary gland, giving off a variable number of branches to the gland along its course. The submental artery branches from the facial artery 3-15 mm below the mandible, just above where the facial artery emerges above the submandibular gland1, 2. The entire facial artery can be mobilized from the submandibular gland by dividing small branches to the gland along its course, and can be mobilized even more proximally by dividing the posterior belly of the digastric. Above the gland it is joined by the facial vein, both of which are crossed by the marginal mandibular nerve (Figures 2b, 3).
Submental artery (Figures 2 - 6)
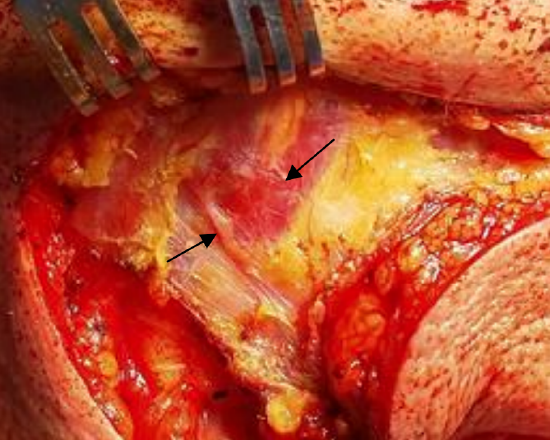
Figure 5: Perforator (arrow) crossing superficial to anterior belly of right digastric
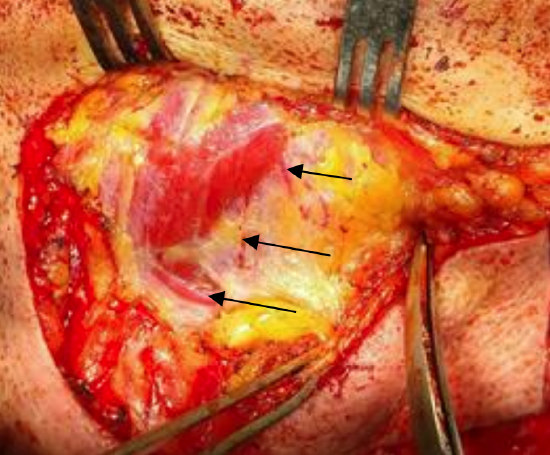
Figure 6: Perforators (arrows) crossing deep to anterior belly of right digastric
The submental artery has a diameter of 1-2 mm at its origin from the facial artery. It runs between the submandibular gland and the inferomedial margin of the mandible keeping deep to platysma but superficial to the mylohyoid muscle, where it gives off branches to the gland. Rarely, it passes through the submandibular gland2. It then runs either deep (>70%) or superficial to the anterior belly of digastric to enter the submental triangle. Here it gives off perforators to the subdermal plexus which perfuses platysma and skin. The positions of these perforators that perfuse the submental island are variable; usually there are 2 major perforators on either side of the anterior belly of digastric. The submental artery is about 6 cm long, and anastomoses with the contralateral artery in about 90% of cases2. It also anastomoses with the sublingual artery (which runs deep to the mylohyoid muscle) via a branch that pierces the mylohyoid muscle.
Marginal mandibular nerve (Figure 2)
This is a terminal branch of the inferior division of the facial nerve and crosses superficial to the facial vein and artery (Figures 2b, 3). It runs deep to platysma just below the border of mandible. Because it supplies the muscles of the lower lip (depressor anguli oris), injury results in loss of depression of the lower lip.
Venous anatomy (Figures 2, 7, 8)
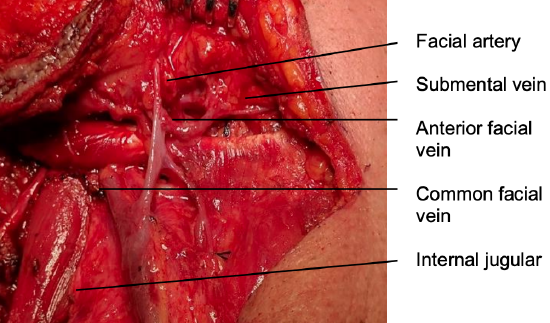
Figure 7a: Venous anatomy
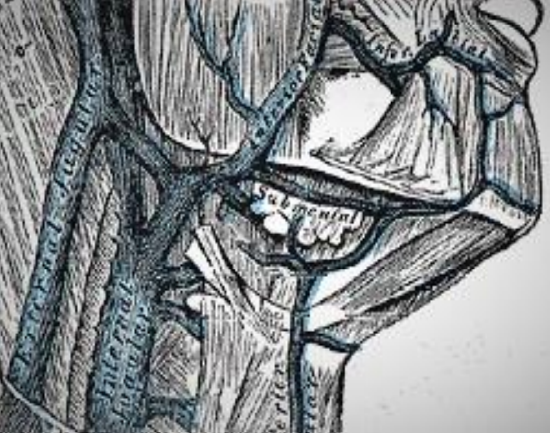
Figure 7b: Venous anatomy
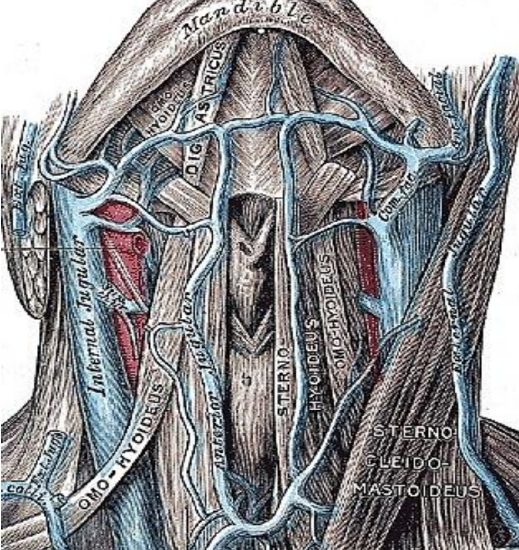
Figure 8: Venous anatomy
Venous drainage of the submental flap is via the submental vein. It measures about 2 mm in diameter2. The vein runs superficial to the anterior belly of digastric and courses parallel and generally just inferior to the submental artery to join the anterior facial vein (Figures 7a,b - 8).
Mylohyoid artery (Figure 9)
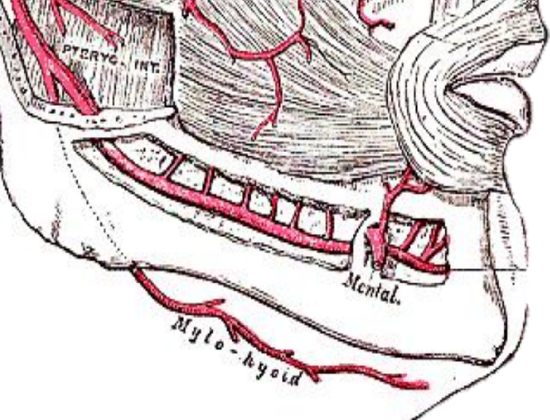
Figure 9: Mylohyoid artery is a branch of the inferior alveolar artery
The mylohyoid artery and vein are encountered when the surgeon elevates the anterior submandibular gland from the lateral surface of the mylohyoid muscle (Figure 9). It branches from the inferior alveolar artery just before it enters the mandibular foramen, crosses mylohyoid and disappears anteriorly behind the digastric. It has connections with the submental artery, and via a defect in the mylohyoid with the sublingual artery in the floor of the mouth.
Indications for submental artery island flap
- Skin defects of the lower 2/3 of the face (excellent texture and color match)
Figure 10: FOM defect suited to reconstruction with SIF
- Buccal, cheek, lateral floor of mouth and tongue resections (Figure 10)
- Oropharyngeal resections
- Hypopharyngeal resections
- Esophageal augmentation e.g. postlaryngectomy stenosis
Contraindications
- Sacrifice of facial artery or vein
- Inability to close donor site due to inadequate skin laxity
- Neck dissection requiring oncologic clearance of Level 1a, e.g. anterior floor of mouth cancers, as fat and lymph nodes of the submental triangle are included in the flap.
Relative contraindications
- Clinically palpable nodes in Level 1b
- Heavy beard growth may be problematic for intraoral reconstruction, although radiation therapy reduces hair growth
Anesthesia
Avoid muscle paralysis so that the surgeon can stimulate or monitor the marginal mandibular nerve
Surgical steps
- Expose the inferior margin of the mandible and the lower lip in the surgical field to monitor movement of the lip when the marginal mandibular nerve is mechanically or electrically stimulated

Figure 11: Pinching the submental skin

Figure 12: Outline of submental flap

Figure 13: Platysma exposed
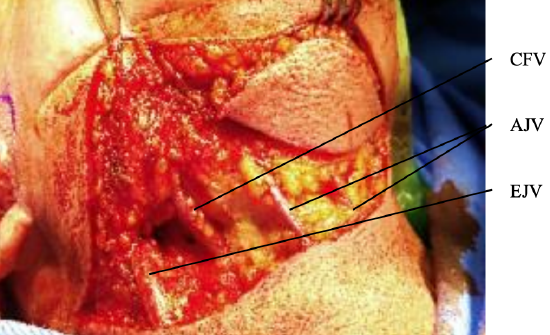
Figure 14: Incision through platysma, with anterior jugular (AJV), common (CFV) and external jugular (EJV) veins visible
- Pinch the submental skin to determine the maximum AP-dimension of the flap that can be closed (Figure 11)
- Design a skin incision along a cervical skin crease incision in the upper neck; the incision is preferably placed about 2 finger-breadths below the mandible to protect the marginal mandibular nerve (Figure 12)
- Design the flap in the submental (and submandibular) triangle to incorporate the cervical skin incision (Figure 12)
- Incise skin and fat down to platysma muscle; veins and marginal mandibular nerve are deep to platysma (Figure 13)
- Note: Unlike with neck dissections or submandibular salivary gland excision, the facial veins must be preserved
- Extend the incision through platysma, taking care not to injure the common or anterior facial veins (Figure 14)
- Transect and ligate the anterior and external jugular veins
- Identify the common and anterior facial veins as they pass over the capsule of the submandibular salivary gland (Figures 2, 7)
- Raise a subplatysmal flap over the common and anterior facial veins and the facial artery superiorly using a dissecting scissors up to the mandibular ramus
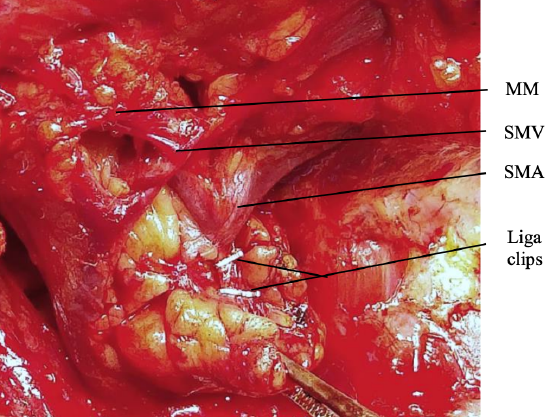
Figure 15: Marginal mandibular nerve (MM), submental vein (SMV), and submental artery (SMA), and Liga clips where branches of artery to submandibular salivary gland have been divided
- Identify the facial artery where it appears just above the posterosuperior edge of the submandibular salivary gland, just below the lower margin of the mandible (Figure 15)
- Identify the marginal mandibular nerve; using scissors or a hemostat, carefully dissect cephalad along the lateral aspect of the anterior facial vein and facial artery to where the nerve crosses laterally over these vessels (Figure 15)
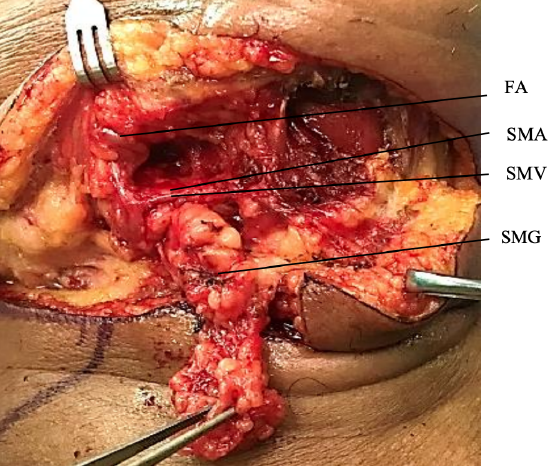
Figure 16: Facial nodes, fat and submandibular salivary gland (SMG) have been dissected from the submental vein (SMV) and artery (SMA) and facial artery (FA)

Figure 17: Facial nodes, fat and submandibular salivary gland have been dissected from the submental vein and artery
- Clear facial nodes and fatty tissue along the lower margin of the mandible if concern exists about metastases e.g. with cancer of the facial skin, lips, or floor of mouth and tongue, taking care to preserve the vascular pedicle and the marginal mandibular nerve (Figures 16, 17)
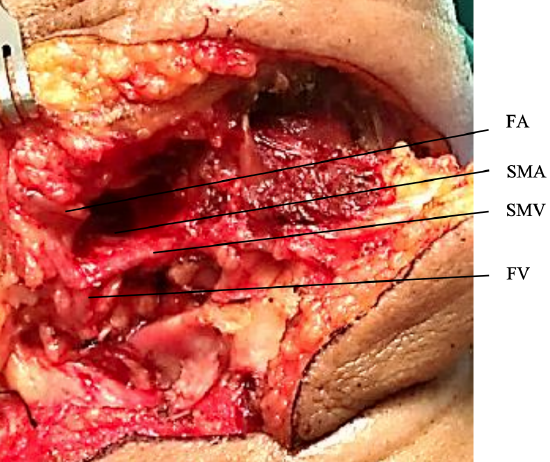
Figure 18: Submental vein (SMV), submental artery (SMA), facial artery (FA), facial vein (FV)
- Dissect the submental vascular pedicle (Figure 18)
- Identify the submental artery where it originates from the facial artery 3-15 mm below the mandible
- Identify and preserve the submental vein where it enters the facial vein
- Dissect anteriorly above the submental artery and vein as they course between the upper surface of the submandibular gland and the inner aspect of the mandible taking care not to injure the marginal mandibular nerve; the artery is generally superior to the vein
- Next dissect in a subcapsular plane over the submandibular salivary gland, and divide and ligate branches and tributaries between the submental artery and vein and the submandibular salivary gland as they are encountered (Figure 18)
- Note: If done for non-oncologic reasons, preserve a cuff of soft tissue around the vascular pedicle
- Avoid dissecting beyond the anterior belly of digastric as this would injure the perforators that supply the flap
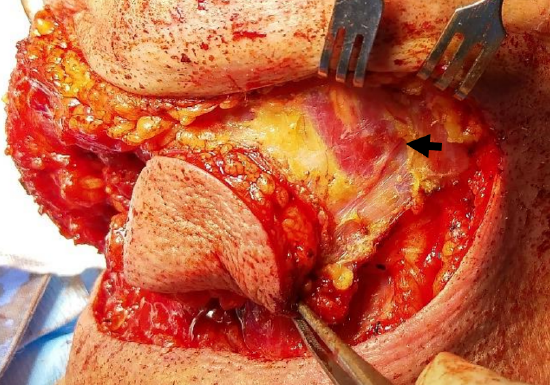
Figure 19: Skin, subcutaneous fat and platysma incised around perimeter of flap onto mylohyoid and opposite digastric; note branch of contralateral submental artery crossing digastric (arrow)
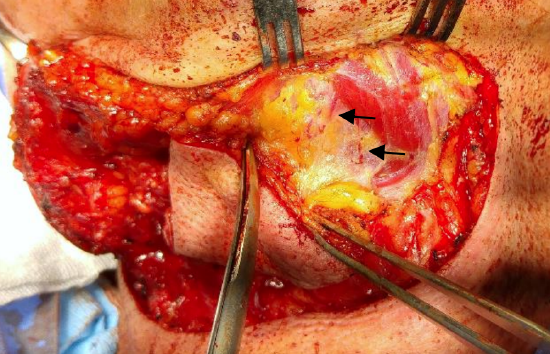
Figure 20: Skin, subcutaneous fat and platysma being elevated off opposite digastric and mylohyoid; note two branches of contralateral submental artery branches emerging from deep to anterior belly of digastric
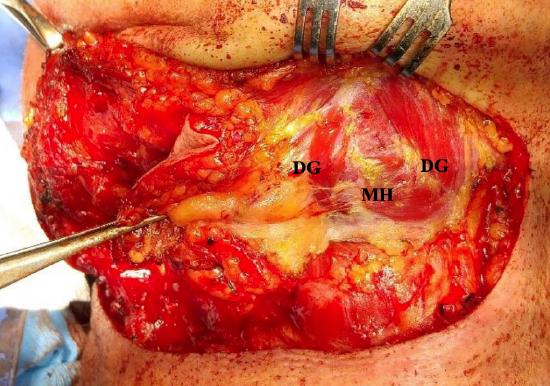
Figure 21: Flap elevated up to anterior belly of digastric (DG) which will be divided superiorly and inferiorly and be included in the flap (MH = mylohyoid)
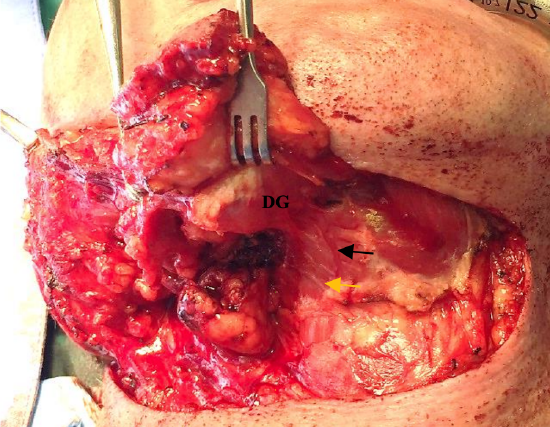
Figure 22: Anterior belly of digastric (DG) has been divided inferiorly and included in the flap, exposing the mylohoid and mylohyoid artery (black arrow) and nerve (yellow arrow)

Figure 23a: Skin cancer to be resected
Figure 23b: Completed superficial parotidectomy and mobilized flap

Figure 23c: Flap ready to be inset

Figure 24: Closed donor site
- Raising the flap (SIF)
- Incise skin, subcutaneous fat, and platysma around the perimeter of the flap onto the mylohoid and contralateral digastric muscles (Figure 19)
- Commence elevation of the flap inferiorly or on the contralateral side to the vascular pedicle
- Divide and ligate the anterior jugular veins where they enter the flap inferiorly (Figure 14)
- Elevate the flap off the contralateral digastric and mylohoid muscles up to the ipsilateral digastric (Figures 20, 21)
- On the pedicled side of the flap, divide the anterior belly of digastric from its insertion onto the lesser cornu of the hyoid bone (Figure 22)
- Include the anterior belly of digastric in the flap while reflecting the flap off the mylohyoid muscle to avoid injury to the two major perforators that run on either side to the digastric
- The mylohoid vessels and nerve now come into view; branches to the submental artery may have to be divided
- Divide the anterior belly of digastric superiorly at its insertion onto the mandible
- The flap is now mobilized and can be transferred to the recipient site on its pedicle (Figures 23a-c)
- The donor site is closed over a suction drain (Figure 24)
Variations
1. If the SIF is to include skin of the submandibular triangle, the superior flap should be raised in such a way to preserve the perforators between the submental vessels and the flap; this requires that the subplatysmal dissection is not carried beyond the upper margin of the submandibular salivary gland
2. If the submandibular gland is to be removed, then the facial artery must be preserved by dividing the few small branches passing between the artery and the gland

Figure 25a: Large defect following resection of lateral and base of tongue cancer that crossed the midline posteriorly

Figure 25b: Submental flap outlined

Figure 25c: Flap being elevated with mylohyoid divided along midline raphe (arrowed)
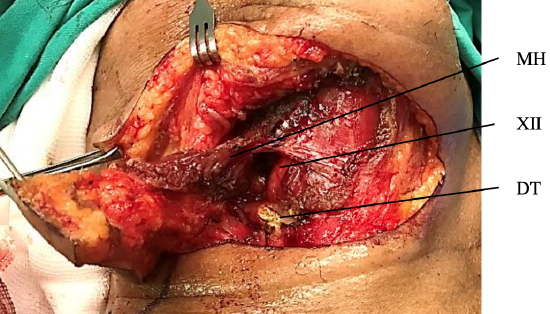
Figure 25d: Flap elevated with mylohyoid (MH) and digastric with divided digastric tendon (DT) and hypoglossal nerve (XIIn) visible
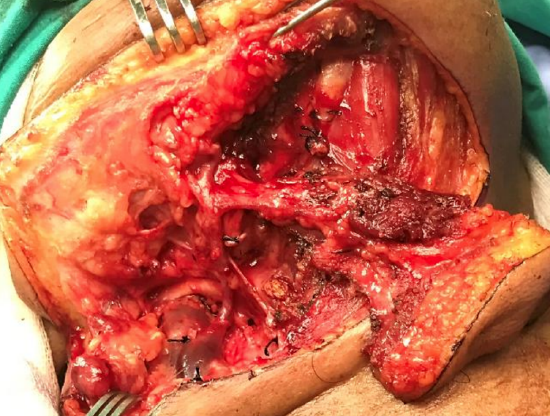
Figure 25e: Flap fully mobilized on vascular pedicle

Figure 25f: Flap delivered into mouth
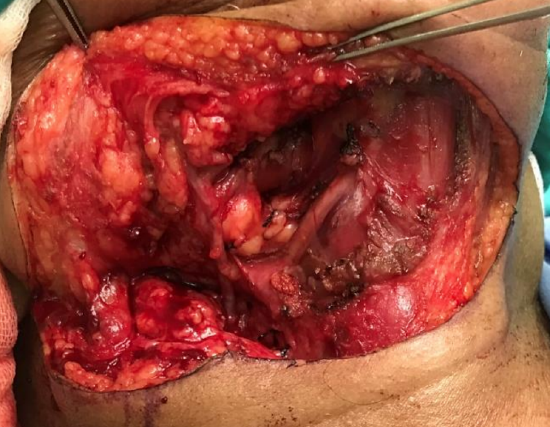
Figure 25g: View of vascular pedicle passing into mouth, divided digastric tendon, hypoglossal nerve, and cut edge of mylohyoid muscle

Figure 25h: Final reconstruction
3. Including mylohyoid muscle in the flap (Figures 25a-h) http://www.ahns.info/resources/educa...d-flapharvest/
Some favor including the mylohyoid muscle in the flap to protect the distal vessels and perforators; or to provide additional bulk; or to provide direct access for the flap to the floor of the mouth. The release of the mylohyoid medially is done with electrocautery in the midline exposing the vertical orientation of the geniohyoid muscle; keeping the vessel protected between the mylohyoid and the anterior belly of the digastric is an excellent technique to protect the vascularization of the flap
- After mylohoid has been exposed in the submental triangle, the midline raphe between the two mylohyoids is divided to expose the geniohyoid muscles
- Divide the mylohyoid from the hyoid bone with electrocautery taking care not to injure the hypoglossal nerve or ranine veins
- Reflect the flap superiorly keeping deep to mylohyoid
- Divide the mylohyoid from the mandible superiorly Figures 24a-h illustrate a patient who underwent transoral resection of a large lateral and base of tongue cancer that crossed the midline posteriorly. The defect was repaired with a submental flap that included anterior belly of digastric and the mylohyoid muscle for additional volume.
4. Designing a large skin paddle

Figure 26: Skin paddle for large flaps: For extra width, the superior incision is done right under the lower border of the mandible (red star) and the lower incision as low as the pinch test allows in the submental area. Lateral extensions are drawn 4cm below the jaw line in the submandibular areas (green arrow)
For wide flaps, the superior incision is traced right under the mandible in the submental area and the inferior incision as low as the pinch test allows (Figure 26). The scar is then hidden under the jaw line and barely visible from a front view. For lengthy defects or when in need of a long reach, the skin paddle can be extended laterally as far as needed. To avoid hurting the marginal branch the lateral extensions are made about 4 cm below the jaw line (Figure 26).
5. Gaining additional pedicle length and arc of rotation
- Facial artery
- Divide the facial artery above the origin of the submental artery
- Free the facial artery from the submandibular salivary gland by dividing all its branches to the gland
- Even more length can be achieved by dividing the posterior belly of digastric to expose the facial artery behind the muscle to its origin from the external carotid artery
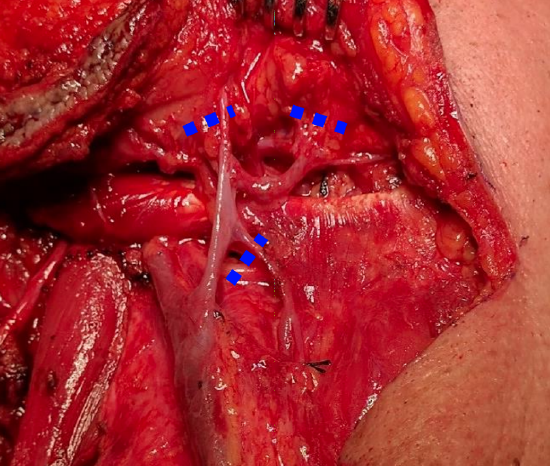
Figure 27: Gaining additional venous length and increasing arc of rotation by dividing veins at points shown
- Facial vein (Figure 27)
- Divide the vein above the submental vein
- Divide the posterior facial vein from the common facial vein
6. Reverse-flow SIF
To reach more superior defects such as the upper face or the hard palate, the flap can be based on reverse-flow through the facial artery and vein by dividing the facial artery below the submental artery and the common facial vein below the submental vein or the posterior facial vein. There is however an increased risk of flap failure because of venous valves in the facial vein that can impair venous return in reverse flow flaps. A hybrid flap (facial artery pedicled, facial vein micro-anastomosed) can be done to avoid this complication.
7. SIF free microvascular transfer flap
The SIF may be used as free microvascular transfer flap based either on the submental or the facial vessels. The limitation to rotate the submental flap higher superiorly is the vein; thus, to extend the submental flap more superiorly one must re-anastomose the submental vein with the retromandibular or temporal vein.
8. SIF with bone

Figure 28a: Bone included in the SIF through an inferior marginal mandibulectomy in the symphysis/parasymphysis area
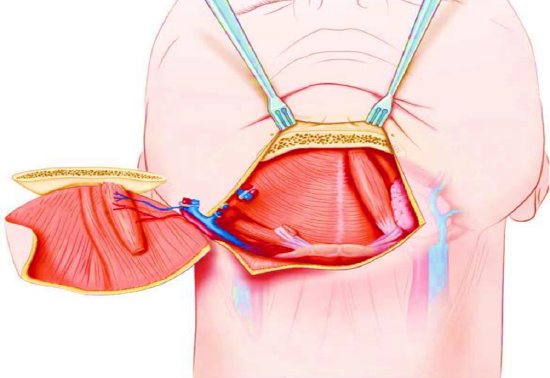
Figure 28b: Bone included in the SIF
An osteomyocutaneous SIF can be used to reconstruct small composite defects of the mandible, maxilla and orbit. A small rim of bone from the inferior part of the mandible in the symphysis and parasymphysis area is sectioned and kept attached to the flap (Figures 28a,b).
This inferior marginal mandibulectomy has little cosmetic impact on the shape of the mandible. One must consider that the freedom of motion between bone and skin will be very limited.
9. Deepithelialization
The flap can be deepithelialized to counter the problem of hair growth in men.
Clinical examples
Case 1: Figures 29a-d illustrate a patient following resection of retromolar cancer, and reconstruction of the soft tissue defect with a submental flap.
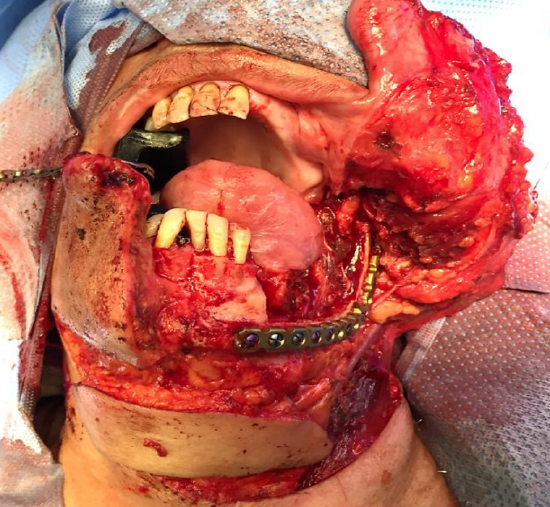
Figure 29a

Figure 29b

Figure 29c

Figure 29d: Excellent cosmetic result and hidden scar post raising of an SIF flap to reconstruct the retromolar trigone deficit
Case 2: Figures 30a-j illustrate a patient who underwent a maxillectomy, in whom the orbital rim was reconstructed with a rim of mandible that was included in the submental flap.

Figure 30a: Skin resection required

Figure 30b: Total maxillectomy defect

Figure 30c: Inferior marginal mandibulectomy
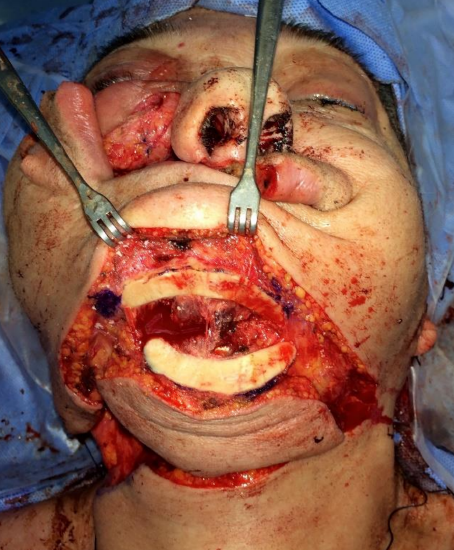
Figure 30d: Raising an SIF with inferior rim of the mandible

Figure 30e: Marginal mandibulectomy used to reconstruct inferior orbital rim

Figure 30f: Submental skin island used for infraorbital skin defect
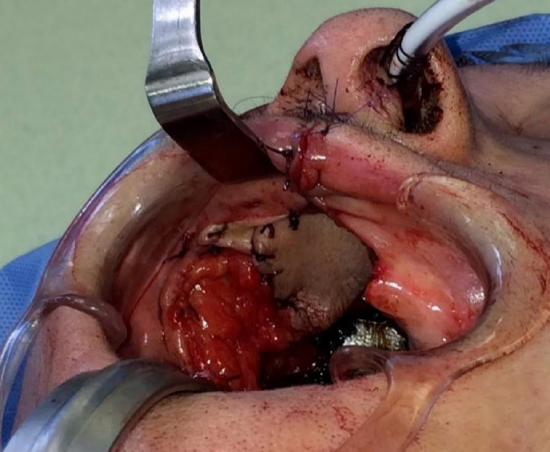
Figure 30g: Insetting the intraoral part of the flap after de-epithelialization of the middle part of the flap

Figure 30h: Completed reconstruction
Figure 30i: Inferior orbital rim 6 months after the surgery
Figure 30j: Six months after SIF reconstruction of total maxillectomy
Case 3: Figures 31a-d illustrate a patient with a through-and-through defect of the cheek following wound complications after skin cancer resection and radiation therapy. The defect was repaired with a submental artery flap.

Figure 31a: Cheek defect

Figure 31b: Flap elevated with anterior belly of digastric muscle

Figure 31c: Note de-epithelialized strip to permit flap to be used both inside the mouth and externally

Figure 31d: Flap sutured into place
Case 4: Figures 32a-c illustrate employing a submental flap to reconstruct a large buccal mucosal cancer defect to avoid subsequent fibrosis and trismus

Figure 32a: Buccal defect

Figure 32b: Flap outlined
Figure 32c: Flap inset
Case 5: Figure 33 illustrates the benefits of a submental artery island flap following resection of a large skin cancer of the cheek with parotidectomy in a patient with lupus, in terms of colour, texture and bulk.

Figure 33: Submental artery island flap prior to suturing to defect
Case 6: Buccal mucosal cancer resection defect in an elderly patient (Courtesy Zenon Yeung, Hong Kong)
Figure 34a: Cancer of buccal mucosa
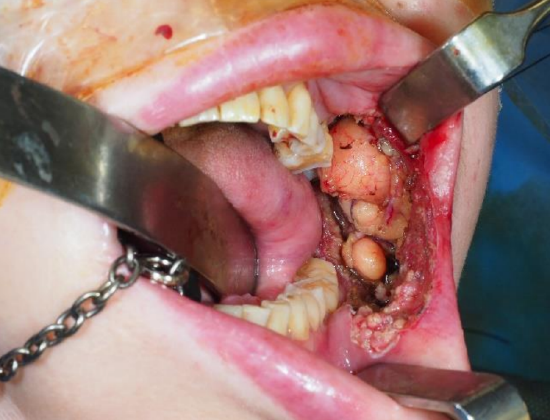
Figure 34b: Buccal defect with buccal fat visible

Figure 34c: Submental artery island flap prior to inset
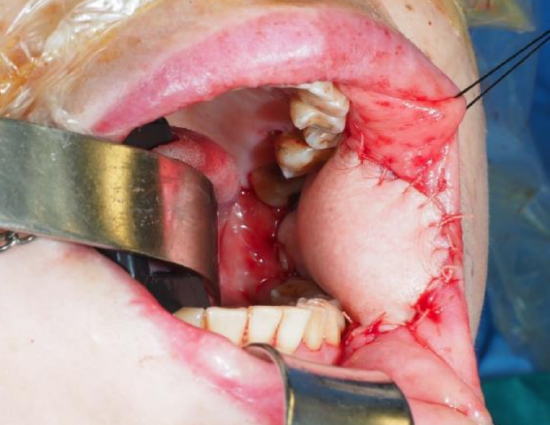
Figure 34d: Submental artery island flap sutured into defect
References
- Faltaous AA, Yetman RJ. The submental artery flap: an anatomic study. Plast Reconstr Surg. 1996 Jan;97(1):56-60; discussion 61-2
- Magden O, Edizer M, Tayfur V, Atabey A. Anatomic study of the vascularture of the submental artery flap. Plast Reconstr Surg. 2004 Dec;114(7):1719- 23
Video (American Head & Neck Society)
Other flaps described in The Open Access Atlas of Otolaryngology Head & Neck Operative Surgery
- Pectoralis major flap
- Buccinator myomucosal flap
- Buccal fat pad flap
- Nasolabial flap
- Temporalis muscle flap
- Deltopectoral flap
- Paramedian forehead flap
- Upper and lower trapezius flaps
- Cervicofacial flaps
- Supraclavicular flap
- Latissimus dorsi flap
- Local flaps for facial reconstruction
- Radial free forearm flap
- Free fibula flap
- Rectus abdominis flap
- Anterolateral free thigh flap
- Thoracodorsal artery scapular tip (TDAST) flap
- Principles and technique of microvascular anastomosis for free tissue transfer flaps in head and neck reconstructive surgery
Authors
Mohammad Alfalasi MD DES
Otolaryngology Residency Program Director
Tawam Hospital in affiliation with Johns Hopkins International
Abu Dhabi Al Ain, United Arab Emirates
mfelasi@hotmail.com
Tareck Ayad MD FRCSC
Associate Professor
Division of Otolaryngology Centre Hospitalier Universitaire de Montréal
Montreal, Canada
tareck.ayad@umontreal.ca
Author & Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za