
5.15: Supraclavicular Flap for Head and Neck Reconstruction
- Page ID
- 53287

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
SUPRACLAVICULAR FLAP FOR HEAD & NECK RECONSTRUCTION
Marie-Renée Atallah, Mohammad Alfalasi, Tareck Ayad
The supraclavicular flap is a perforant pedicled fasciocutaneous flap with a reliable axial pattern, based on the supraclavicular artery. It is centered over the shoulder joint, extending from the supraclavicular region up to the lateral surface of the upper arm, overlying the deltoid muscle. It is well suited to restore lining and volume of head and neck defects, while preserving good function and acceptable cosmetic outcomes.
The supraclavicular flap was first described by Lamberty in 1979 21. However, because of a high incidence of distal flap necrosis, its use was limited at that time. In 1997, Pallua and Machens 3 described a modification of the flap, which was successfully used to reconstruct eight cases of neck contractures. They later published anatomical studies which helped the flap to regain respectability. Its use and indications have increased since then.
Surgical anatomy
Arterial vascular anatomy
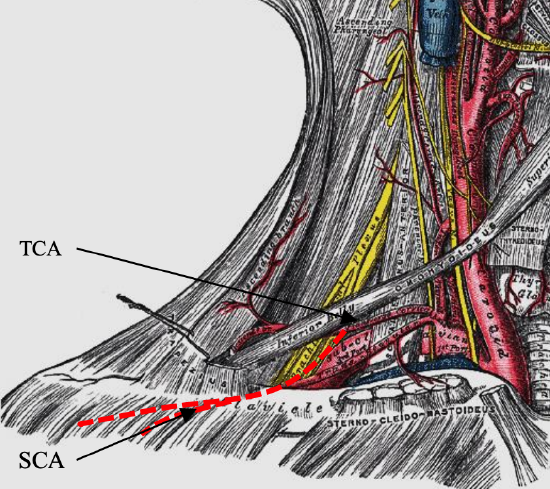
Figure 1: Typical anatomy of transverse cervical (TCA) and supraclavicular artery (SCA)
Transverse cervical artery (Figure 1): The transverse cervical artery branches off the thyro-cervical trunk in 60-95% of cases1,5. In the remaining cases, it originates from the first part of the subclavian artery. It courses along the base of the posterior neck and travels deep to the lateral part of the inferior belly of the omohyoid muscle. The diameter of the transverse cervical artery ranges from 2.5-3.5 mm5. It supplies the trapezius muscle and the skin over the shoulder through direct cutaneous branches located cephalad to the clavicular insertion of the muscle2.
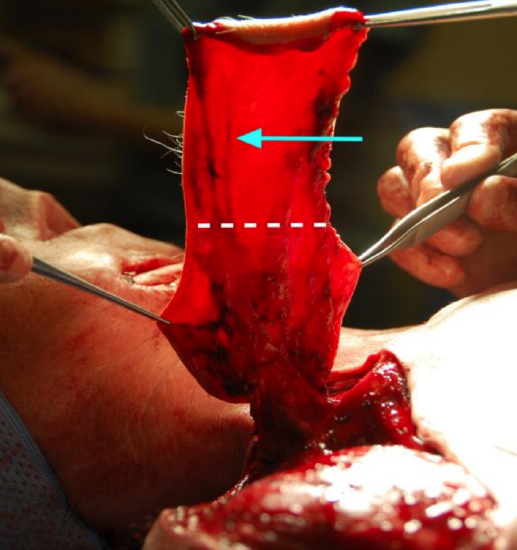
Figure 2: After the supraclavicular artery (arrow) exits from the deep fascia (area under the dotted line), it runs in a superficial plane

Figure 3: The supraclavicular artery generally divides into numerous branches over the deltoid muscle (white star) at the junction of the middle and lateral thirds of the clavicle
Supraclavicular artery (Figure 1): The supraclavicular artery generally originates from the transverse cervical artery 5,12. Infrequently it arises from the suprascapular artery 1,4,5. The supraclavicular artery has a diameter between 1-1.5 mm 5, 7, 14. In 70-90% of cases its origin is in the area of mid-third of the clavicle 5,18. In the remaining cases, it branches in the area of the lateral third of the clavicle. The supraclavicular artery then travels perpendicularly from the transverse cervical artery and pierces the deep fascia of the deltoid muscle 30 mm distally 5,14. Before reaching this point, it can give off one or two small branches 5. After its exit from the deep fascia, it runs in a superficial plane (Figure 2) and continues its course over the acromioclavicular joint, at the junction of the middle and lateral thirds of the clavicle. At this level, the artery generally divides into numerous branches over the deltoid muscle (Figure 3). These branches develop multiple anastomoses with the vascular network of the thoracoacromial artery 14, the posterior circumflex humeral artery 1 and the superficial branch of the transverse cervical artery 14.
These vessels form a consistent number of perforators interconnected by direct and indirect linking vessels through the subdermal plexus. Over the deltoid muscle, the direct linking vessels support the distal supraclavicular artery and drive the blood flow from the artery to the perforators. After the insertion of the deltoid muscle, their numbers decline and the vascularization of the distal flap relies principally on indirect linking vessels and recurrent flow. Thereby, beyond this point, the vascularization follows a random pattern and a higher incidence of necrosis is seen 14. Accordingly, as described by Pallua and Noah 22, the angiosome extends from the supraclavicular region to the ventral surface of the deltoid muscle and ranges up to 10 cm in width and 22 cm in length.
Skin landmarks

Figure 4: The origin of the supraclavicular artery is located in a triangle bounded inferiorly by the clavicle (white line), medially by the posterior border of the sternocleidomastoid muscle (red line) and laterally by the external jugular vein (blue line)
The origin of the supraclavicular artery where it branches off the transverse cervical artery, is located in a triangle bounded inferiorly by the clavicle, medially by the posterior border of the sternocleidomastoid muscle and laterally by the external jugular vein 3 (Figure 4). It is found approximately 2.5-4 cm above the clavicle 7 and on average 2 cm posterior to the sternocleidomastoid muscle 22 and 6.5-10 cm from the sternoclavicular joint 5,7,18,22.
Venous anatomy
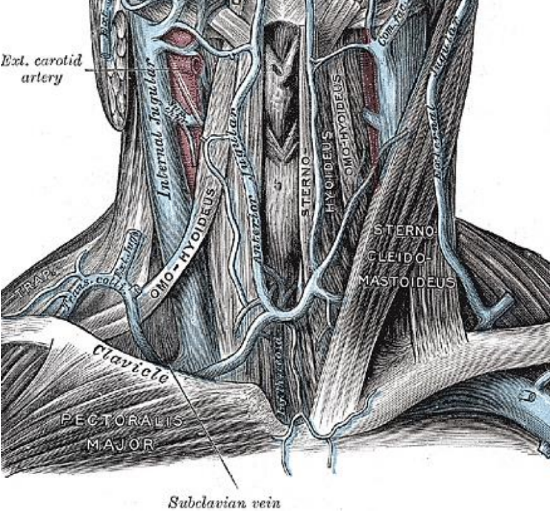
Figure 5: Transverse cervical vein
Two venae comitantes usually accompany the supraclavicular artery. They usually drain into the transverse cervical vein (Figure 5). One of the two veins may drain alternatively into the external jugular vein. They provide venous drainage to the skin proximal to the deltoid origin.
Distal to the deltoid’s origin, the skin is drained by the subdermal veins, which in turn drain into either the cephalic vein or the comitant vein of the brachial artery 14. There is also a secondary venous drainage for the skin over the deltoid via the perforating veins to the circumflex humeral veins.
Nerve anatomy
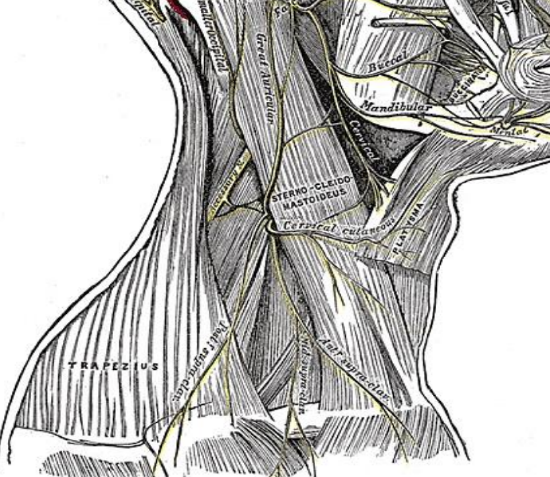
Figure 6: Medial, intermediate and lateral supraclavicular nerves
The 3rd and 4th cervical nerves merge and then arborise into 3 to 5 branches, forming the supraclavicular nerves 22 (Figure 6). These branches provide sensation to the region of the flap over the shoulder. They also supply the skin of the lateral neck and upper chest. The major cutaneous nerve root from the supraclavicular nerves pierces the deep fascia centrally with respect to the sternocleidomastoid muscle 15. As this nerve root advances toward the pedicle, it gives two cutaneous branches, an anterior and a lateral branch. The anterior branch is located 1-2 cm anterior to the vascular pedicle and can sometimes be seen during flap harvest.
Properties of supraclavicular flap
Raising a supraclavicular flap is a simple and quick procedure, usually done in less than an hour, and is a relatively easy to learn procedure. The flap is a good asset for the surgeon, as it is versatile and can correct multiple types of defects.
The flap is highly reliable and since the procedure is shorter than free flap reconstruction and does not require expertise in microsurgery, the supraclavicular flap is beneficial for high risks patients who can’t sustain long operative time.
The supraclavicular flap is an excellent choice for reconstruction of skin defects in the lower face and neck because of a good texture and color match with the skin of the neck and lower face. It also has great pliability which makes it suitable for reconstruction of areas with high mobility, such as the neck and oral cavity. Also, since the skin in the supraclavicular area is generally hairless, it is an appropriate for mucosal defects. The skin has a thin dermis and little fat, which accounts for the flap's thinness which makes it appropriate for reconstruction of contour sensitive areas such as the anterior neck and for pharyngeal defects in which a bulky flap may impair swallowing.
It can easily reach distant sites, such as the oropharynx, due to its long pedicle and broad arc of rotation. It can also be used for large defects, since the flap can reach a considerable size, with maximum dimensions of approximately 10 x 20 cm.
Indications
Historically the flap was used to reconstruct a variety of defects in the neck and lower third of the face, especially with release of scar contractures following burns, trauma or injuries with acid or Lye 3,16. It is a good option for such defects because of its excellent color match and the skin properties being similar to the surrounding skin. The flap can also be used for head and neck oncologic reconstruction such as defects of the oral cavity, oropharynx, hypopharynx, and tracheostoma, and following parotid and pharyngoesophageal resection 4,12,13,17,20. It has also been reported for reconstruction of the pinna 20,23 and lateral skull base 23. More recently the flap has been successfully used to reconstruct defects following excision of massive arteriovenous malformations of the lower face 8 and in Noma patients 24. It can be used as a primary choice of reconstruction but can also safely be used as a salvage procedure either after radiotherapy or after another flap failure.
Contraindications
The only absolute contraindication is when integrity of the pedicle has been compromised. This can occur in cases of radical neck dissection or neck dissection including Level V where the transverse cervical artery has been ligated. Other surgery that may damage the pedicle are shoulder surgery and excision of skin cancers in the shoulder area. It was previously stated that previous radiotherapy for the neck was a contraindication. It has now however been demonstrated that the flap can be safely used even in the context of previous radiotherapy. If doubt exists concerning the integrity of the pedicle, it can be assessed using preoperative angiography.
Preoperative investigation
Although not routinely required, computed tomography angiography can be performed to assess the integrity of the vascular pedicle or when there is doubt about the supraclavicular artery anatomy.
Surgical technique
The supraclavicular flap can be employed as a rotation flap, tunneled flap, supercharged flap or as a free microvascular transfer flap. If a neck dissection is performed, then vessels to the distal external jugular vein and the transverse cervical artery need to be preserved.
Supraclavicular rotation flap
- Position the patient in a supine position with the head turned to the contralateral side
- Clean the entire neck and shoulder with an antiseptic solution
- Drape the patient to leave the neck, anterior chest and shoulder regions exposed

Figure 7: The origin of the supraclavicular artery is located in a triangle bounded inferiorly by the clavicle (white line), medially by the posterior border of the sternocleidomastoid muscle (red line) and laterally by the external jugular vein (blue line). The large “X” indicates the exact location of the supraclavicular artery, as identified by the Doppler

Figure 8: Patient with plate extrusion following total mandible reconstruction with a fibula flap and radiation therapy. The bone was viable. A supraclavicular flap was used for coverage of the soft tissue defect following removal of the plate. The base of the flap can reach the neck incision. The hatched part of the flap was included to allow primary closure without a dog ear deformity and was meant to be sacrificed after flap inset
- Draw the superficial landmarks for the supraclavicular artery i.e. clavicle, external jugular vein and posterior border of sternocleidomastoid (Figure 7)
- Use a Doppler probe to identify the supraclavicular artery in the triangle previously drawn, and mark its exact location on the skin (Figure 7)
- Use the finger pinch test to evaluate the elasticity of the soft tissue in the shoulder area to determine how much skin can be elevated and still allow primary closure
- Draw the skin island in an elliptical or fusiform design over the supraclavicular and shoulder / upper arm (Figure 8)
- Include the point where the supraclavicular artery pedicle was identified
- The base of the flap can be connected with the neck incision if needed (Figure 8)
- Design the size of the flap according to the defect to reconstruct; maximum size is approx. 12 cm wide x 21 cm long
- The insertion of the deltoid marks the farthest point that the flap can extend without concern for distal necrosis
- The flap can however be made longer if supercharged or pre-expanded
- Do not infiltrate the skin along the incision lines with a vasoconstrictor, as vasoconstriction might complicate assessment of flap perfusion

Figure 9: With the skin island flap delineated, the incision is taken down to the level of the deep fascia

Figure 10: At the junction of the middle and lateral thirds of the clavicle, the supraclavicular artery generally divides into numerous branches over the deltoid muscle (white star)
- With the skin island flap delineated, incise the skin down to the level of deep fascia (Figure 9)
- Elevate the flap by dissecting from distal-to-proximal in a subfascial plane over the deltoid muscle (Figure 10); although some authors prefer to dissect from medial-to-lateral 3, 17
- Elevate the flap using sharp (scalpel) dissection or needle monopolar electrocautery; when dissecting the proximal third of the flap, switch to bipolar electrocautery and cold dissection to avoid inadvertent injury to the supraclavicular artery
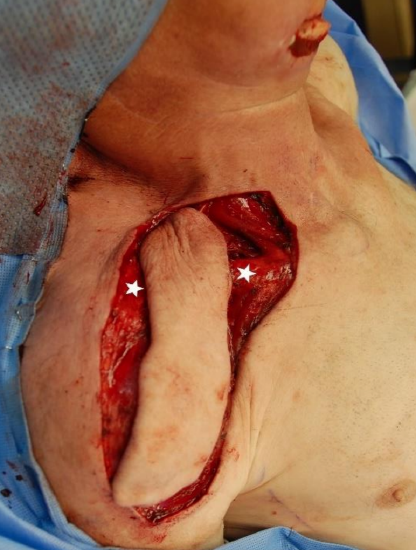
Figure 11: Over the clavicle, the flap is elevated over the periosteum of the clavicle (white stars)
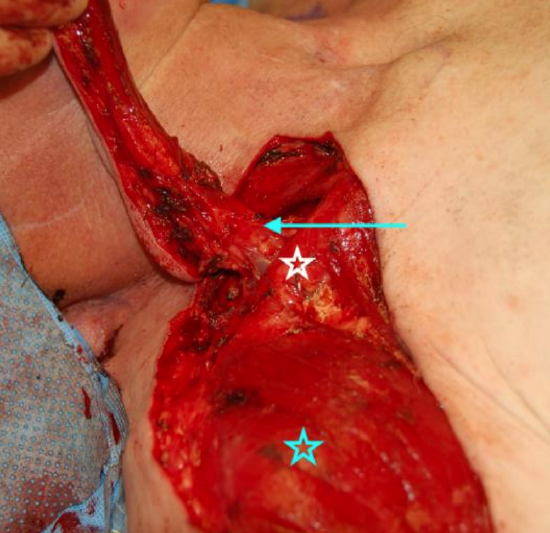
Figure 12: A moderate amount of fat (arrow) can be kept around the expected location of the supraclavicular artery to protect it from inadvertent damage and tension. The blue star is on the deltoid and the white star on the clavicle
- Elevate the flap over the periosteum of the clavicle (Figure 11)
- The pedicle does not need to be skeletonized unless extra mobility of the flap is required; a moderate amount of fat can be kept around the expected location of the supraclavicular artery to protect it from inadvertent damage and tension (Figure 12)
- If the pedicle needs to be skeletonized it can be precisely located with the help of a Doppler. The pedicle is then skeletonized and its attachments released

Figure 13: Subperiosteal dissection on the anterior surf
- Another technique to protect the pedicle is to perform a subperiosteal dissection on the anterior surface of the clavicle (Figure 13)
- Once the pedicle has been located, incise the skin island proximally
- With the flap completely elevated, trim the distal tip of the flap until proper bleeding is noted
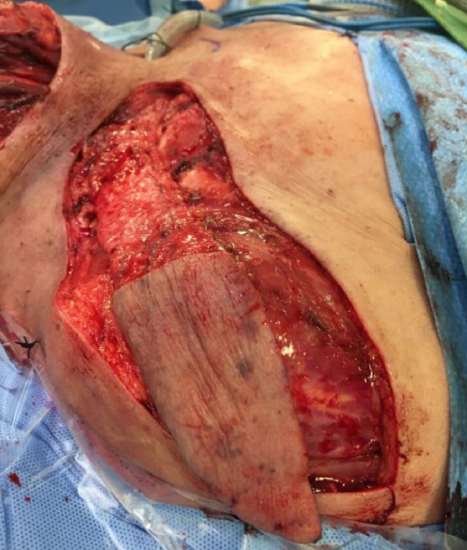
Figure 14: If the supraclavicular flap is tunneled, the proximal part should be deepithelialized

Figure 15: For intraoral reconstruction, the deepithelialized area can be large; care must be taken to preserve part of the dermis to protect the subdermal venous plexus
- If the flap is to be tunneled (Figure 14) or used to reconstruct a mucosal lining (Figure 15), the proximal portion is deepithelialized. Care must be taken to preserve part of the dermis to protect the subdermal venous plexus
- Rotate the flap to inset it into the defect

Figure 16: Extensive skin squamous cell carcinoma requiring wide local excision and functional neck dissection (Courtesy Dr Jackie Bibeau-Poirier)

Figure 17: The skin defect cannot be closed primarily. We elected to perform a supraclavicular flap to optimize color match and contour

Figure 18: Insetting flap following 1800 rotation. The donor site has been closed primarily
- The flap can tolerate 1800 rotation at its origin from the transverse cervical artery (Figures 16, 17, 18)
- Shape the flap to fit the defect and suture it into place; the last part of the flap to incorporate in the defect is the distal extremity, as it will be trimmed and discarded if not needed
- Take care not to stretch or kink the pedicle; keeping some fat around it helps to protect the pedicle
- Most donor sites can be closed primarily in a double layer fashion, using Vicryl 2-0 and staples (Figure 18); extensive undermining in a subcutaneous plane, anteriorly over the pectoralis major muscle and posteriorly over the trapezius muscle, is generally needed to close the donor site primarily
- Flaps that are wider than 10 cm are difficult to close without excessive tension. Options for closure in this case are split-thickness skin graft or a local flap harvested from the dorsal region 5,16
- A suction drain is usually left in the donor site
- The skin island is monitored with coloration, refill and temperature for the first 72 hours
Tunneled flap
The same technique is generally used for tunneled flaps, with the added steps of deepithelialization of the flap and creation of a subcutaneous tunnel for its transposition. Tunneling has the advantage of providing superior aesthetic results. As the flap is thin, compression is rarely an issue. However, care should be taken to create a wide tunnel for the pedicle to avoid compromising the blood flow to the distal flap. Therefore, tunnel flaps are not recommended in previous radiated necks or with scar tissue.
Supercharged flap
The supraclavicular flap can be supercharged if a larger size is needed. The technique has been described using mostly the posterior circumflex artery. According to Vinh et al. 5, the anterior humeral artery, lateral thoracic artery perforator or the thoracoacromial artery perforator can be appropriate for supercharging.
Free flap
The application of the supraclavicular flap as a free flap has previously been described. Since the diameter of the supraclavicular artery is relatively small, its reliability is variable and we recommend using other options before reconstruction as a free flap is considered.
Complications
Superficial distal necrosis: Superficial distal necrosis occurs in 4%-22% of cases 2,5,16-19. Principal causes are excessive tension on the pedicle and inappropriately long flaps. Excessive tension may result from tight closure, tunneling under scar or irradiated tissue, compressive dressings, postoperative neck edema or any other factors that may impair vascularization of the tip of the flap. Avoiding these may prevent distal flap necrosis. In most instances, the necrotic zones will reepithelialize naturally and no intervention is necessary.
Total flap necrosis: This is a dreaded complication, resulting from trauma to the supraclavicular artery during flap harvest. The incidence of total flap necrosis varies between 2-6% 5,9,19, 20. Small and tortuous arteries which are more difficult to locate are risk factors for inadvertent injury to the pedicle. The modified supraclavicular island flap, in which fascia and fat are left surrounding the vascular pedicle may be helpful to prevent total flap necrosis.
Incisional dehiscence: Incisional donor site dehiscence occurs as a result of insufficient undermining when closing the donor site or use of an excessively large flap which results in excessive wound tension. The dehiscence is usually minor and resolve with local wound care. Vacuum assisted closure and skin graft are effective when the dehiscence is more significant.
Hematoma: This is a rare complication. It is important to recognize it promptly as it may prolong healing.
Seroma: Seromas develop in 0-15% 9 of cases and are generally treated with aspiration and wound care.
Shoulder dysfunction: There is minimal morbidity on the shoulder after the procedure. Few patients complain of shoulder pain after supraclavicular flap surgery and most of them respond well to antiinflammatories and physiotherapy. Around 14-22% 4,12,15,16 of patients describe referred sensation to the shoulder with sensate stimulus of the flap such as touching the flap or swallowing when the flap is used for mucosal lining. No paraesthesia or numbness over the shoulder area has been reported. Since the flap includes only skin, fat and fascia, upper limb movement is preserved 2,5,9. When a limitation is present, it is generally temporary 2,9 and results from excessive tension on the closure causing a sensation of tightness over the shoulder area. Herr et al. 9 prospectively studied the shoulder function of 10 patients following supraclavicular flap with objective parameters. They showed that muscle strength was good to excellent in 90% of patients and that the limitations present were mostly range of motion, especially external rotation. Nonetheless, most patients are satisfied with the shoulder function 9,16 and appearance 5,16,20.
Clinical Cases
Case 1: A patient following total laryngectomy and partial pharyngectomy for hypopharyngeal cancer (Figures 19-23)

Figure 19: Mucosal defect requires reconstruction with a flap to avoid stenosis
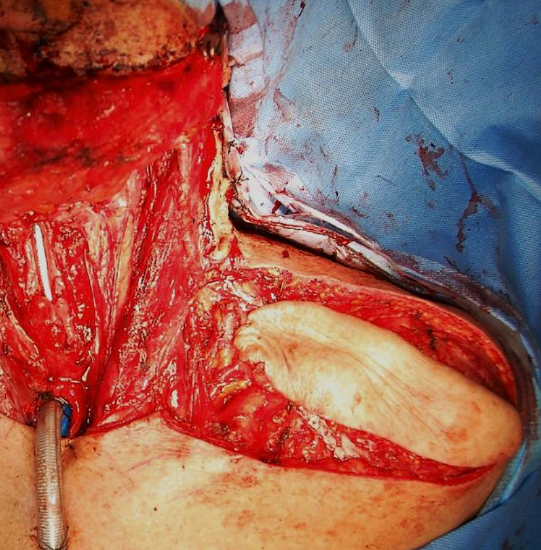
Figure 20: We elected to perform a left supraclavicular flap
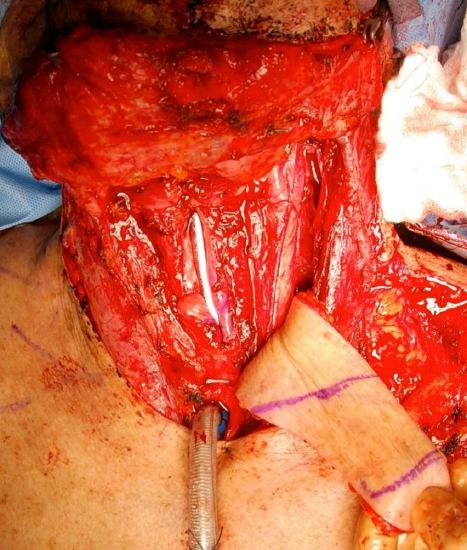
Figure 21: The skin in the central part of the flap between the purple lines was used to reconstruct the mucosal defect. The distal and proximal parts of the flap were deepithelialized and used for coverage and protection of the carotid axis
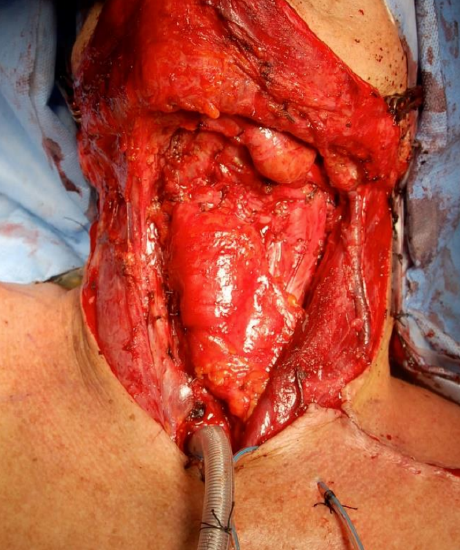
Figure 22: Flap inset

Figure 23: Scar in an irradiated area, 6 months following surgery
Case 2: 80-year-old female with cancer of buccal mucosa, inferior alveolus and floor of mouth involving skin. Underwent hemimandibulectomy, resection of skin and neck dissection. Reconstructed with pectoralis major (intraorally) and supraclavicular artery island flaps (external skin)

Figure 24: Note cancer involving skin, and planning drawings of the pectoralis major and supraclavicular artery island flap

Figure 25: Supraclavicular artery island flap has been used to cover the skin defect, and pectoralis major for intraoral repair
Case 3: Squamous cell cancer of ear treated with superficial parotidectomy, lateral temporal bone resection and selective neck dissection.

Figure 26: Cancer destroying external ear and extending down ear canal

Figure 27: Completed superficial parotidectomy, lateral temporal bone resection and selective neck dissection

Figure 28: Supraclavicular artery island flap used to cover the lateral skull base defect
References
- Lamberty BG, Cormack GC. Misconceptions regarding the cervicohumeral flap. Br J Plast Surg. 1983 Jan;36(1):60-3
- Mathes SJ, Vasconez LO. The cervicohumeral flap. Plast Reconstr Surg. 1978 Jan;61(1):7-12
- Pallua N, Machens HG, Rennekampff O, Becker M, Berger A. The fasciocutaneous supraclavicular artery island flap for releasing postburn mentosternal contractures. Plast Reconstr Surg. 1997 Jun;99(7):1878- 84; discussion 1885-6
- Chiu ES, Liu PH, Friedlander PL. Supraclavicular artery island flap for head and neck oncologic reconstruction: indications, complications, and outcomes. Plast Reconstr Surg. 2009 Jul;124(1):115-23
- Vinh VQ, Van Anh T, Ogawa R, Hyakusoku H. Anatomical and clinical studies of the supraclavicular flap: analysis of 103 flaps used to reconstruct neck scar contractures. Plast Reconstr Surg. 2009 May; 123(5):1471-80
- DiBenedetto G, Aquinati A, Pierangeli M, Scalise A, Bertani A. From the "charretera" to the supraclavicular fascial island flap: revisitation and further evolution of a controversial flap. Plast Reconstr Surg. 2005 Jan;115(1):70-6
- Chan JW, Wong C, Ward K, SaintCyr M, Chiu ES. Three- and fourdimensional computed tomographic angiography studies of the supraclavicular artery island flap. Plast Reconstr Surg. 2010 Feb;125(2):525- 31
- Hormozi AK, Shafii MR. Supraclavicular flap: reconstructive strategy for massive facial arteriovenous malformations. J Craniofac Surg. 2011 May;22(3):931-6
- Herr MW, Bonanno A, Montalbano LA, Deschler DG, Emerick KS. Shoulder function following reconstruction with the supraclavicular artery island flap. Laryngoscope. 2014 Nov;124(11):2478-83
- Fischborn GT, Schmidt AB, Giessler GA. Prefabricated supraclavicular flap as a salvage procedure for a failed microvascular hypopharyngeal defect closure in a tetraplegic patient. Ann Plast Surg. 2011 Sep;67(3):245- 50
- Goyal N, Emerick KS, Deschler DG, Lin DT, Yarlagadda BB, Rich DL, Durand ML. Risk factors for surgical site infection after supraclavicular flap reconstruction in patients undergoing major head and neck surgery. Head Neck. 2016 Nov;38 (11):1615-20
- Giordano L, Di Santo D, Occhini A, Galli A, Bertino G, Benazzo M, Bussi M. Supraclavicular artery island flap (SCAIF): a rising opportunity for head and neck reconstruction. Eur Arch Otorhinolaryngol. 2016 Dec;273(12):4403-12
- Emerick KS, Herr MA, Deschler DG. Supraclavicular flap reconstruction following total laryngectomy. Laryngoscope. 2014 Aug;124 (8):1777-82
- Ross RJ, Baillieu CE, Shayan R, Leung M, Ashton MW. The anatomical basis for improving the reliability of the supraclavicular flap. J Plast Reconstr Aesthet Surg. 2014 Feb; 67(2):198-204
- Sands TT, Martin JB, Simms E, Henderson MM, Friedlander PL, Chiu ES. Supraclavicular artery island flap innervation: anatomical studies and clinical implications. J Plast Reconstr Aesthet Surg. 2012 Jan;65(1):68-71
- Loghmani S, Eidy M, Mohammadzadeh M, Loghmani A, Raigan F. The supraclavicular flap for reconstruction of post-burn mentosternal contractures. Iran Red Crescent Med J. 2013 Apr;15(4):292-7
- Alves HR, Ishida LC, Ishida LH, Besteiro JM, Gemperli R, Faria JC, Ferreira MC. A clinical experience of the supraclavicular flap used to reconstruct head and neck defects in late-stage cancer patients. J Plast Reconstr Aesthet Surg. 2012 Oct;65 (10):1350-6
- Nthumba PM. The supraclavicular artery flap: a versatile flap for neck and orofacial reconstruction. J Oral Maxillofac Surg. 2012 Aug;70(8): 1997-2004
- Su T, Pirgousis P, Fernandes R. Versatility of supraclavicular artery island flap in head and neck reconstruction of vessel-depleted and difficult necks. J Oral Maxillofac Surg. 2013 Mar;71(3):622-7
- Sandu K, Monnier P, Pasche P. Supraclavicular flap in head and neck reconstruction: experience in 50 consecutive patients. Eur Arch Otorhinolaryngol. 2012 Apr;269(4): 1261-7
- Lamberty BG. The supra-clavicular axial patterned flap. Br J Plast Surg. 1979; 32:207-12
- Pallua N, Magnus Noah E. The tunneled supraclavicular island flap: an optimized technique for head and neck reconstruction. Plast Reconstr Surg. 2000 Mar;105(3):842-51; discussion 852-4
- Emerick KS, Herr MW, Lin DT, Santos F, Deschler DG. Supraclavicular artery island flap for reconstruction of complex parotidectomy, lateral skull base, and total auriculectomy defect. JAMA Otolaryngol Head Neck Surg. 2014 Sep;140(9): 861-6
- Hartman EH, Van Damme PA, Suominen SH. The use of the pedicled supraclavicular flap in noma reconstructive surgery. Plast Reconstr Surg. 2006 Jul;118(1):270-1
Other flaps described in The Open Access Atlas of Otolaryngology Head & Neck Operative Surgery
- Pectoralis major flap
- Buccinator myomucosal flap
- Buccal fat pad flap
- Nasolabial flap
- Temporalis muscle flap
- Deltopectoral flap
- Paramedian forehead flap
- Upper and lower trapezius flaps
- Cervicofacial flaps
- Submental artery island flap
- Latissimus dorsi flap
- Local flaps for facial reconstruction
- Radial free forearm flap
- Free fibula flap
- Rectus abdominis flap
- Anterolateral free thigh flap
- Thoracodorsal artery scapular tip (TDAST) flap
Authors
Marie-Renée Atallah MD
Resident
Otolaryngology - Head & Neck Surgery
Centre Hospitalier de l'Université de Montréal
Montreal, Canada
marie-renee.atallah@umontreal.ca
Mohammad Alfalasi MD DES
Otolaryngology Residency Program Director
Tawam Hospital in affiliation with Johns Hopkins International
Abu Dhabi Al Ain, United Arab Emirates
mfelasi@hotmail.com
Tareck Ayad MD FRCSC
Associate Professor
Division of Otolaryngology
Centre Hospitalier Universitaire de Montréal
Montreal, Canada
tareck.ayad@umontreal.ca
Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za