
1.10: Vasoactive Drugs II - Heart Failure
- Page ID
- 10631

Congestive Heart Failure& its Pharmacological Management
The physiological framework for understanding CHF: The Pressure-Volume Loop of the LV
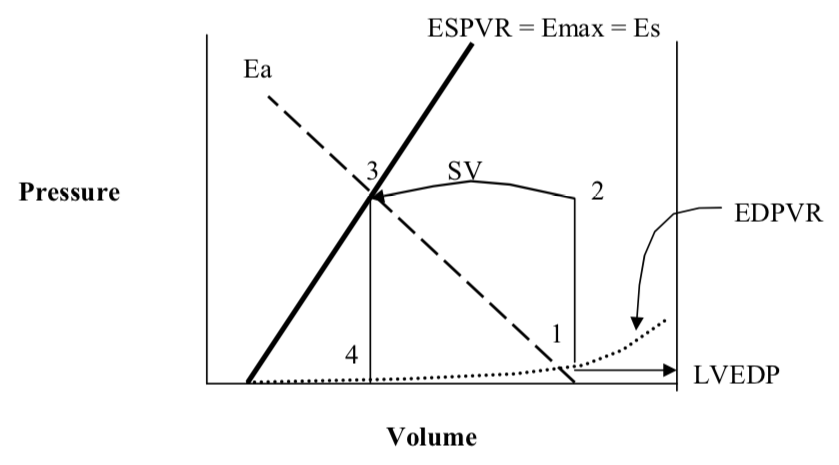
Key:
1 = End diastole, just prior to LV contraction. The pressure at 1 is known as the left ventricular end diastolic pressure (LVEDP)
(1 to 2 = isovolemic contraction)
2 = Opening of the aortic valve and beginning of ejection into the aorta
(2 to 3 is the volume ejected from the LV into the aorta which is the stroke volume (SV))
3 = End systole. The pressure at 3 is known as the end-systolic pressure (ESP). The aortic valve shuts just after 3.
(3 to 4 is isovolumic relaxation)
4 = Beginning of passive diastolic filling.
4 to 1 is diastolic filling along the dotted curve. This dotted curve is the end-diastolic pressure volume relation (EDPVR).
ESPVR = End-systolic pressure volume relation. This also called Emax or Es which stand for maximal elastance or elastance at end-systole, respectively. This characterizes the strength of the LV irrespective of the systolic load it faces.
Ea = Effective arterial elastance. This is characterizes the arterial tree and the load it presents to the LV during systole. Ea is primarily determined by arterial resistance but arterial compliance effects it too.
Ea and ESPVR “Couple” to exactly determine the stroke volume.
What is meant by “congestive heart failure” (CHF)?
Congestive heart failure simply means that the pulmonary blood volume is expanded and, therefore, the pulmonary circulation is congested with blood. The congestion arises because of elevated left ventricular end-diastolic pressure (LVEDP). An elevated LVEDP is a hallmark of uncompensated congestive heart failure. Common symptoms include shortness of breath, fatigue, orthopnea and paroxysmal nocturnal dyspnea (PND). Once a patient is treated for CHF they may become asymptomatic. This is termed compensated CHF and does NOT imply that the underlying disease process has gone away! It is entirely reasonable and even common for patients who are well medically managed to have a markedly reduced ejection fraction (EF) yet be capable of most normal activities. This handout pertains primarily to LEFT ventricular failure. Although RIGHT ventricular failure occurs, it is less common and not the focus of this handout.
How long do people live if they have congestive heart failure?
For all comers, the mortality is 50% in five years. However, if a patient is symptomatic, despite treatment, one-year mortality can approach 50%. Approximately five million people have congestive heart failure (CHF) in the United States at any given time. The great majority of these patients have primarily left ventricular failure.
There are FIVE main physiologic ways to get CHF
- Decrease the strength of the LV and thereby decrease its ejection – this causes the LVEDP to rise (CHF). This is characterized by a reduction in the slope of the ESPVR line.
Acute causes include: myocardial ischemia, myocardial infarction, sepsis syndrome, myocardial contusions, excess beta blockers or excess calcium channel blockers.
Chronic causes include: dilated cardiomyopathy due to certain viral illnesses, multiple myocardial infarctions or large territory myocardial infarctions, excessive alcohol consumption and certain chemotherapeutic agents such as adriamycin. Prolonged pressure overload (hypertension and aortic stenosis) also causes a weak heart after initially causing hypertrophy. With continued overload, the compensation of hypertrophy progresses to a failing myocardium (a low ESPVR) - Provide much too much venous return (and hence filling) to the LV– this causes the LVEDP to rise (CHF).
Acute causes include: excessive volume administration or large increased in venous tone as with some vasoconstrictors. Exercise causes a large increase in venous return and if the LV cannot eject all that it receives, there is an elevation in the LVEDP (CHF).
Chronic causes include profound chronic anemia, longstanding mitral regurgitation or aortic regurgitation. Poor compliance with diuretic therapy or with high salt intake can cause a rise in the plasma volume which in turn elevates the venous return. - Alter the passive filling characteristics of the LV such that a normal filling volume is associated with a high pressure – this causes the LVEDP to rise (CHF). This is calleddiastolic CHF.
Acute causes include: myocardial ischemia
Chronic causes include: prolonged pressure overload (hypertension and aortic stenosis) which cause this problem by initially causing hypertrophy of the cardiac muscle. The thickened myocardium does not relax well. Certain infiltrative diseases like amyloidosis cause diastolic CHF. - Present an enormous load to the LV such that it cannot eject well – this causes the LVEDP to rise (CHF). This is characterized by having a severe increase in the arterial load and is shown by a steep increase in the slope of Ea, the effective arterial elastance.
Acute causes include: pheochromocytoma and catechol release, very poorly controlled hypertension.
Chronic causes include: pressure overload with aortic stenosis or long term severe hypertension5. Reduce the function of the heart with other problems:
Acute causes include: severe tachycardia or bradycardia, pericardial tamponade, acute ventricular septal defect, acute mitral regurgitation.
Regardless of the cause of CHF, certain management strategies pertain to all patients.
Salt restriction and fluid restriction are regular features of any congestive heart failure management program. Secondly, any underlying cause should be treated aggressively.
For example, hypertension is a very frequent precipitator of congestive heart failure and should be managed aggressively. Similarly, coronary artery disease should be managed with the full armamentarium available for that disease. Patients having profound anemia and who suffer from high output congestive heart failure should have their anemia and underlying pathology managed. For patients who are drinking excessive alcohol and have alcohol- induced cardiomyopathy, treating the underlying alcoholic behaviors are essential. Additional risk factor management clearly includes smoking cessation, lipid optimization, optimizing diabetes management and so on.
We will now consider how to treat CHF for the first four mechanisms outlined above.
In almost all cases of symptomatic CHF, the LVEDP is too high. This is responsible for the symptom of shortness of breath. When the pulmonary blood volume is congested with blood, the lungs become stiff and the work of breathing goes way up. There are multiple acute ways to reduce the LVEDP:
- Improve LV systolic performance (improve the ESPVR): inotropes (digoxin, milrinone, dobutamine). Digoxin is the hallmark drug for augmenting systolic performance. Although digoxin certainly helps in the symptomatic management of systolic heart failure, it does not confirm a mortality benefit.
- Improve arterial loading conditions (reduce Ea): arterial dilators such as angiotensin converting enzyme inhibitors (ACE inhibitors – lisinopril, captopril), and angiotensin receptor blockers (ARB’s – valsartan, losartan). An important feature of ACE inhibitors is their mortality benefit. All patients with CHF who do not have contraindications should be taking ACE inhibitors. For patients who cannot tolerate ACE inhibitors, angiotensin receptor blockers are very likely to be an adequate substitute and their mortality benefit is being studied presently. Other drugs that reduce Ea include hydralazine, minoxidil and nitroprusside. These drugs do not confer a mortality benefit.
- Improve the diastolic filling characteristics of the LV: All underlying causes such as myocardial ischemia should be treated.
- Reduce the blood volume and thus drop the LVEDP: diuretics (loop diuretics – furosemide, bumetanide and potassium sparing diuretics – spironolactone). Of the diuretic therapies, only spironolactone has been shown to have a mortality benefit in treating patients with CHF.
The Secondary Physiologic Response to LV Failure.
The failing LV precipitates a host of secondary neuroendocrine events which are well described in figure 23-10 from Golan.
Image removed for copyright reasons. See Fig. 23-10 in Golan.
Management of secondary neuroendocine effects.
It is the correction of neuroendocrine abnormalities (elevated renin, angiotensin II, and aldosterone) that is most likely responsible for prolonging the lives of patients with CHF. Remodeling is the process that the left ventricle undergoes when it is insulted either by chronic unfavorable loading conditions or chronic neuroendocrine “siege.” It involves a change in ventricular mass or dimension without a corresponding change in the number of ventricular myocytes. The functional left ventricle first begins to hypertrophy, then begins to dilate, and finally becomes fibrotic. The exact mechanisms that cause remodeling are unclear but the neuroendocrine effects seem to be responsible. It is currently thought that reducing the neuroendocrine effects of CHF is what leads to longer lives for those patients having CHF. This may explain why ACE inhibitors, ARB’s, spironolactone (blocks aldosterone) and beta-blockers (block renin production) all confer a mortality benefit.
The use of beta-blockers is, paradoxically, one of the fundamental treatments for systolic congestive heart failure. These drugs offer a definite mortality benefit.
Beta-blockers are well known to depress LV systolic function (i.e. reduce ESPVR) and thus appear counterintuitive in managing congestive heart failure. However, beta-blockers have been found to offer an important mortality benefit to patients with congestive heart failureincluding those with severely decreased LV function. It is most likely that beta-blockers interfere with the secondary neuroendocrine events (such as an activated sympathetic nervous system and elevated renin) associated with congestive heart failure. The beta-blockade should be started in all patients who do not have significant contraindications to these drugs. Presently metoprolol and carvedilol are the two drugs with a proven mortality benefit. Patients with symptomatic congestive heart failure (uncompensated CHF) are poor candidates for these drugs. However, once their symptoms are resolved (with diuretics and ACE inhibitors along with other management strategies), the introduction of beta-blockers is reasonable. Initial doses are usually low and titrated upwards, as tolerated.
Knowing that Beta-Blockers offer a mortality benefit, do physicians use beta-blockers as the data suggest?
No. For reasons that are not entirely clear, physicians often deny patients beta-blockers.
Severe Decompensated CHF.
In the case of severe, Class IV/Stage D CHF (see appendix), patients are often admitted to the hospital for IV therapy using inotropes such as Digoxin, Dobutamine or inodilators such asMilrinone or Amrinone These drugs treat symptoms of CHF, but do not offer a mortality benefit. In fact, chronic therapy with some of these drugs can actually increase mortality. They are only used as a “bridge” to more definitive therapy or until resolution of the precipitating event can be accomplished. In patients with acute severe decompensated CHF, a number of highly invasive therapies exist. Intra-aortic balloon pumping (IABP) offers a bridge to cardiac transplantation. Many patients with dilated cardiomyopathies die due to malignant dysrhythmias. Patients with dilated hearts and severely reduced ejection fraction have a survival benefit with automatic implantable cardiac defibrillators (AICD’s).
Lastly, with severely reduced ejection fractions and cardiac conduction defects, cardiac resynchronizing pacemakers offer symptomatic relief of CHF.
Appendix
The Clinical Characterization of CHF follows two schemes. One is older and based on symptoms (NYHC), the other is newer and based on disease progression (Stages A, B, C, D).
New York Heart Classifications of symptoms (NYHC I, II, III, IV)
- Class I: Patients with no limitation of activities and no symptoms from ordinary activities.
- Class II: Patients with slight, mild limitation of activity; they are comfortable with rest or with mild exertion.
- Class III: Patients with marked limitation of activity; they are comfortable only at rest.
- Class IV: Patients who should be at complete rest; confined to bed or chair; any physical activity brings on discomfort and symptoms occur at rest.
The current Staging system deals with progression of the underlying disease.
Stage A: Patients at high risk for developing heart failure are those with:
● Hypertension
● Diabetes mellitus
● Coronary artery disease (including being S/P myocardial infarction)
● History of cardiotoxic drug therapy
● History of alcohol abuse
● History of rheumatic fever
● Family history of cardiomyopathy
- Stage B: Pateints with known heart disease but who have never had symptoms of heart failure.
- Stage C: Patients with known heart disease with current or prior symptoms. Symptoms include:
● Shortness of breath
● Fatigue
● Reduced exercise tolerance
- Stage D: Presence of advanced symptoms even with optimized medical care.
Appendix
All types of CHF start with an elevated LVEDP. There are multiple ways to get an elevated LVEDP. In each case below, the dotted line shows the circumstance prior to developing symptoms of CHF. Examples are from Suga and Sagawa.
Type I is from too much venous return from any cause
Type II is from too much ‘afterload’ (Ea is too high)
Type III is from diastolic dysfunction from any cause (unfavorable EDPVR)Type IV is from a weak LV (ESPVR is too low) from any cause