
7.4: Electrolytes
- Page ID
- 21145
Learning Objectives
- Describe the functions of the following electrolytes:
- sodium
- chloride
- potassium
- phosphorus
- Describe the impact of sodium, chloride, potassium, and phosphorus imbalances
- Identify sources of sodium, chloride, potassium, and phosphorus
Electrolytes
Electrolytes are mineral salts dissolved in water, including sodium, potassium, chloride, and phosphorus. Electrolytes carry electrical charges:
- Sodium (Na+) and potassium (K+) are positively charged
- Chloride (Cl-) and phosphorus (HPO42-, hydrogen phosphate) are negatively charged
Fluids have an overall neutral charge due to the balances between electrolytes. In intracellular fluid, K+ and HPO42- are the predominant electrolytes; in extracellular fluid, Na+ and Cl- predominate.
Functions of Electrolytes
One of the major functions of electrolytes is to help regulate fluid balance. Water follows the movement of electrolytes, moving by osmosis to areas where the concentration of electrolytes is high. This allows for the controlled movement of fluids into and out of cells. Electrolytes also help nerves respond to stimuli. The movement of sodium (Na+) into the nerve cell generates an electrical impulse. The cell membrane returns to its normal electrical state through the release of potassium (K+) to the outside of the cell. In addition, electrolytes signal our muscles to contract. The movement of calcium (Ca2+) into a muscle cell stimulates the muscle to contract. The Ca2+ is pumped back out of the cell after the muscle contraction.
Although electrolytes are important for these functions, these nutrients provide other functions as well as we'll see below.
Sodium
Sodium is a major extracellular cation (positively-charged ion) that is water soluble. In contrast to many minerals, sodium absorption in the small intestine is extremely efficient and in a healthy individual, 90-95% is excreted by the kidneys, the remainder in the feces and sweat. Very little sodium is required in the diet because the kidneys actively reabsorb sodium. Kidney reabsorption of sodium is hormonally controlled, allowing for a relatively constant sodium concentration in the blood.
Functions of Sodium
Sodium is essential for maintaining fluid balance while also assisting with nutrient transport across the cell membrane. The sodium-potassium pumps in the cell's membrane continuously pump sodium ions out of the cell (Figure \(\PageIndex{1}\)) to establish a high concentration of positive ions on the outside of the cell (this is also called a chemical gradient). When glucose is transported into a cell, a different transport protein, called the sodium-glucose symporter, uses the sodium gradient to power glucose movement into the cell. Sodium and glucose both move into the cell. Water passively follows the sodium. To restore balance, the sodium-potassium pump transfers sodium back to the extracellular fluid and water follows. Every cycle of the sodium-potassium pump involves the movement of three sodium ions out of a cell, in exchange for two potassium ions into a cell (Figure \(\PageIndex{1}\)). To maintain charge neutrality on the outside of cells every positively-charged sodium ion is followed by a negatively-charged chloride ion. Every cycle of the pump costs one molecule of ATP (adenosine triphosphate). The constant work of the sodium-potassium pump maintains the solute equilibrium and consequently, water distribution between intracellular and extracellular fluids.
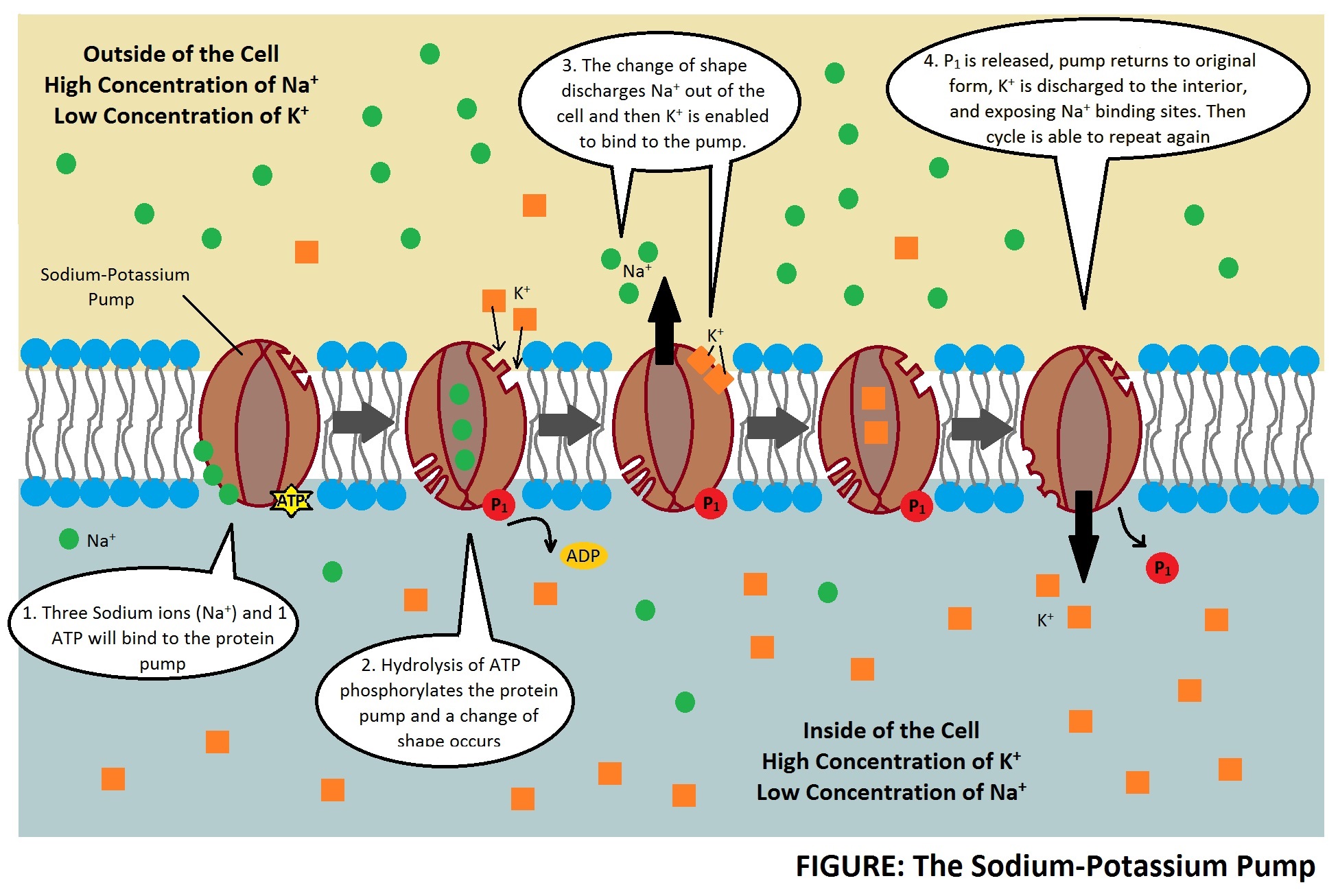 Figure \(\PageIndex{1}\): The sodium-potassium pump is the primary mechanism for cells to maintain water balance between themselves and their surrounding environment. (CC BY-SA 4.0; by Clod94 via Wikimedia Commons)
Figure \(\PageIndex{1}\): The sodium-potassium pump is the primary mechanism for cells to maintain water balance between themselves and their surrounding environment. (CC BY-SA 4.0; by Clod94 via Wikimedia Commons) The unequal movement of the positively charged sodium and potassium ions makes intracellular fluid more negatively charged than the extracellular fluid. This charge gradient is another source of energy that a cell uses to perform work related to nerve transmission and muscle contraction. Nerve impulse transmission results from the transport of sodium cations into a nerve cell, which creates a charge difference (or voltage) between the nerve cell and its extracellular environment. Similar to how a current moves along a wire, a sodium current moves along a nerve cell. Stimulating a muscle contraction also involves the movement of sodium ions as well as other ion movements. For a muscle to contract, a nerve impulse travels to a muscle. The movement of the sodium current in the nerve communicates to the muscle by releasing the neurotransmitter, acetylcholine. Acetylcholine signals sodium channels in the muscle to open and sodium rushes in, creating another current that travels along the muscle eventually culminating in contraction. In both the nerve cell and the muscle cell, the sodium that went in during a stimulus now has to be moved out by the sodium-potassium pump.
Sodium is essential for nutrient absorption in the small intestine and also for nutrient reabsorption in the kidney. Amino acids, glucose, and water must make their way from the small intestine to the blood. To do so they pass through intestinal cells on their way to the blood. The transport of nutrients through intestinal cells is facilitated by the sodium-potassium pump, which by moving sodium out of the cell, creates a higher sodium concentration outside of the cell (requiring ATP).
Sodium Imbalances
Sweating is a homeostatic mechanism for maintaining body temperature, which influences fluid and electrolyte balance. Sweat is mostly water but also contains some electrolytes, mostly sodium and chloride. Under normal environmental conditions (i.e., not hot, humid days) water and sodium loss through sweat are negligible but is highly variable among individuals. It is estimated that sixty minutes of high-intensity physical activity can produce approximately one liter of sweat; however, the amount of sweat produced is highly dependent on environmental conditions. A liter of sweat typically contains between 1 and 2 grams of sodium and therefore exercising for multiple hours can result in a high amount of sodium loss in some people. Additionally, hard labor can produce substantial sodium loss through sweat. In either case, the lost sodium is easily replaced in the next snack or meal.
Hyponatremia, or a low blood-sodium level, can result from excessive sodium loss in sweat or drinking too much water. For example, hyponatremia has been seen in people engaged in strenuous physical activity who consume large amounts of water and fail to replace sodium. The excess water dilutes the sodium concentration in blood. Illnesses causing vomiting, sweating, and diarrhea may also cause hyponatremia. The symptoms of hyponatremia, also called water intoxication since it is often the root cause, include nausea, muscle cramps, confusion, dizziness, and in severe cases, seizures, coma and death. Hyponatremia is rare because healthy kidneys are capable of excreting up to one liter of excess water per hour. However, when hyponatremia occurs, the physiological events that occur include:
- Excessive sodium loss and/or water intake.
- Low sodium levels in the blood and in the fluid between cells (interstitial fluid).
- Water moves to where solutes are more concentrated (i.e., into the cells).
- Cells swell.
- Symptoms, including nausea, muscle cramps, confusion, and dizziness appear. In severe cases, coma and death can result.
Other people at risk of hyponatremia are people on a very low sodium diet due to special diets. These types of diets are used to treat kidney disease, hypertension, and heart disease. Excessive vomiting, for example, bulimia nervosa, or excessive diarrhea can also cause a loss of sodium resulting in hyponatremia.
On the other end of the spectrum is a condition know as hypernatremia (an abnormally high blood-sodium level). Hypernatremia can happen in patients with congestive heart failure or kidney disease when the kidneys are not excreting sodium effectively. Hypernatremia can result in high blood volume, edema (swelling), and high blood pressure (hypertension).
Sodium Recommendations
The National Academies of Sciences, Engineering, and Medicine set an Adequate Intake (AI) level for sodium for healthy adults at 1,500 milligrams (Table \(\PageIndex{1}\)).1 Table salt is approximately 40% sodium and 60% chloride. One teaspoon of salt contains approximately 2,300 mg sodium, so only ⅔ teaspoon of salt is needed in the diet to meet the AI for sodium. An additional DRI category, called the Chronic Disease Risk Reduction Intake (CDRR), was established for sodium. The CDRR considers evidence related to chronic disease risk. For sodium, individuals with intake levels above the CDRR should consider reducing their intake to reduce chronic disease risk.
| Age Group | Adequate Intake (mg/day) | Tolerable Upper Intake Level (mg/day) | Chronic Disease Risk Reduction Intake (CDRR) |
|---|---|---|---|
| Infants (0–6 months) | 110 | ND | ND |
| Infants (7–12 months) | 370 | ND | ND |
| Children (1–3 years) | 800 | ND | Reduce intakes if above 1,200 mg/day |
| Children (4–8 years) | 1,000 | ND | Reduce intakes if above 1,500 mg/day |
| Children (9–13 years) | 1,200 | ND | Reduce intakes if above 1,800 mg/day |
| Adolescents (14–18 years) | 1,500 | ND | Reduce intakes if above 2,300 mg/day |
| Adults (19–50 years) | 1,500 | ND | Reduce intakes if above 2,300 mg/day |
| Adults (51–70 years) | 1,500 | ND | Reduce intakes if above 2,300 mg/day |
| Adults (> 70 years) | 1,500 | ND | Reduce intakes if above 2,300 mg/day |
| ND = not determined | |||
Sources of Sodium
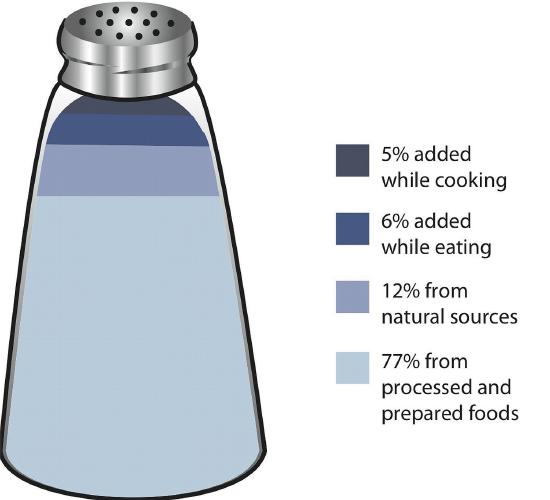
Most sodium in the typical American diet comes from processed and prepared foods, including restaurant foods (Figure \(\PageIndex{2}\)). Manufacturers add salt to foods to improve texture and flavor, and also as a preservative. The amount of salt in similar food products varies widely. Some foods, such as meat, poultry, and dairy foods, contain naturally-occurring sodium. Naturally-occurring sodium accounts for less than 12% of dietary intake in a typical diet.
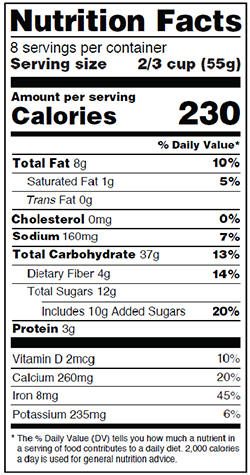
The Nutrition Facts label displays the amount of sodium (in milligrams) per serving of the food in question (Figure \(\PageIndex{3}\)). Information in the % Daily Value (% DV) section of the food label can be used to determine if the food is high in sodium (> 20% DV) or low in sodium (< 5% DV). Various claims about the sodium content in foods can also be seen on a food's label; these claims must be in accordance with Food and Drug Administration (FDA) regulations (Table \(\PageIndex{2}\)).2
| Claim | Meaning |
|---|---|
| “Light in Sodium” or “Low in Sodium” | Sodium is reduced by at least 50 percent |
| “No Salt Added” or “Unsalted” | No salt added during preparation and processing* |
| “Lightly Salted” | 50 percent less sodium than that added to similar food |
| “Sodium Free” or “Salt Free” | Contains less than 5 mg sodium per serving |
| “Very Low Salt” | Contains less than 35 mg sodium per serving |
| “Low Salt” | Contains less than 140 mg sodium per serving |
|
*Must also declare on package “This is not a sodium-free food” if food is not sodium-free. |
|
For those with hypertension or those looking for a way to decrease salt use, using a salt substitute for food preparation is one option. However, many salt substitutes still contain sodium, just in lesser amounts than table salt. Also, remember that most salt in the diet is not from table-salt use, but from processed foods. Salt substitutes often replace the sodium with potassium. People with kidney disorders often have problems getting rid of excess potassium in the diet and are advised to avoid salt substitutes containing potassium. People with liver disorders should also avoid salt substitutes containing potassium because their treatment is often accompanied by issues with potassium regulation. Alternatively, spices can be used to add flavor without using salt or salt substitutes.
Chloride
Chloride is the primary anion (negatively-charged ion) in extracellular fluid. Chloride moves easily across membranes following the sodium and potassium gradients. In addition to passively following sodium and potassium, chloride has its own protein channels that reside in cell membranes. These protein channels are especially abundant in the gastrointestinal tract, pancreas, and lungs. Chloride is the major anion in sweat and vomit. It is the anion of stomach acid, HCl.
Functions of Chloride
Chloride aids in fluid balance mainly because it follows sodium in order to maintain charge neutrality. Chloride channels also play a role in regulating fluid secretion, such as pancreatic juice into the small intestine and the flow of water into mucus. Fluid secretion and mucus are important for many of life’s processes. Chloride has several other functions in the body, most importantly in acid-base balance. Blood pH is maintained in a narrow range and the number of positively charged substances is equal to the number of negatively charged substances. Proteins, such as albumin, as well as bicarbonate ions and chloride ions, are negatively charged and aid in maintaining blood pH. Hydrochloric acid (a gastric acid composed of chlorine and hydrogen) aids in digestion and also prevents the growth of unwanted microbes in the stomach. Immune-system cells require chloride, and red blood cells use chloride anions to remove carbon dioxide from the body. Chloride also assists in the transmission of nerve impulses.
Chloride Imbalances
Low dietary intake of chloride is rare. However, low blood levels of chloride can occur with severe dehydration, diarrhea, and/or frequent vomiting. Symptoms typically are similar to those of hyponatremia and include weakness, nausea, and headache. Excess chloride in the blood is rare with no characteristic signs or symptoms.
Chloride Recommendations
The National Academies of Sciences, Engineering, and Medicine set an Adequate Intake (AI) level for chloride for healthy adults at 2,300 milligrams (Table \(\PageIndex{3}\)).3 Just ⅔ teaspoon of table salt per day is sufficient for chloride as well as sodium. The AIs for other age groups are listed in Table \(\PageIndex{3}\).
| Age Group | Adequate Intake (mg/day) |
|---|---|
| Infants (0–6 months) | 180 |
| Infants (7–12 months) | 570 |
| Children (1–3 years) | 1,500 |
| Children (4–8 years) | 1,900 |
| Children (9–13 years) | 2,300 |
| Adolescents (14–18 years) | 2,300 |
| Adults (19–50 years) | 2,300 |
| Adults (51–70 years) | 2,000 |
| Adults (> 70 years) | 1,800 |
Sources of Chloride
Most chloride in the diet comes from salt. (Salt is 60% chloride.) Other dietary sources of chloride include processed foods containing sodium chloride, as well as tomatoes, lettuce, olives, celery, rye, whole-grain foods, and seafood. Although many salt substitutes are sodium-free, they may still contain chloride.
Potassium
Potassium is the major positively-charged ion in intracellular fluid. Most potassium is lost in the urine (80-90%) and the remainder is via the feces. Ninety percent of potassium exists in intracellular fluid, with about 10 percent in extracellular fluid, and only 1 percent in blood plasma. As with sodium, potassium levels in the blood are strictly regulated. The hormone aldosterone is what primarily controls potassium levels, but other hormones (such as insulin) also play a role. When potassium levels in the blood increase, the adrenal glands release aldosterone. The aldosterone acts on the collecting ducts of kidneys, where it stimulates an increase in the number of sodium-potassium pumps. Sodium is then reabsorbed and more potassium is excreted. Because potassium is required for maintaining sodium levels, and hence fluid balance, only about 200 mg of potassium are lost from the body every day.
Functions of Potassium
Potassium plays a role in fluid balance as described earlier in this section. In addition, nerve impulse transmission involves potassium. A nerve impulse moves along a nerve via the movement of sodium ions into the cell. To end the impulse, potassium ions rush out of the nerve cell, thereby decreasing the positive charge inside the nerve cell. This diminishes the stimulus. To restore the original concentrations of ions between the intracellular and extracellular fluid, the sodium-potassium pump transfers sodium ions out in exchange for potassium ions in. On completion of the restored ion concentrations, a nerve cell is now ready to receive the next impulse. Similarly, in muscle cells, potassium is involved in restoring the normal membrane potential and ending the muscle contraction. Potassium is also involved in protein synthesis, energy metabolism, and platelet function, and acts as a buffer in blood, playing a role in acid-base balance.
Imbalances of Potassium
Insufficient potassium levels in the body (hypokalemia) can be caused by a low dietary intake of potassium or by high sodium intakes, but more commonly it results from medications that increase water excretion, mainly diuretics. The signs and symptoms of hypokalemia are related to the functions of potassium in nerve cells and consequently skeletal and smooth muscle contraction. The signs and symptoms include muscle weakness and cramps, respiratory distress, and constipation. Severe potassium depletion can cause the heart to have abnormal contractions and can even be fatal. High levels of potassium in the blood, or hyperkalemia, is toxic and also affects the heart. It is a silent condition as it often displays no signs or symptoms. Extremely high levels of potassium in the blood disrupt the electrical impulses that stimulate the heart and can cause the heart to stop. Hyperkalemia is usually the result of kidney dysfunction.
Groups at risk of developing hypokalemia are individuals with renal and large intestine issues such as urine and diarrhea losses; people with uncontrolled diabetes which causes diabetic acidosis and urine losses; dehydration; prolonged diarrhea or vomiting; and, certain drugs like diuretics, steroids or laxatives. These deficiencies are due to excessive loss and not a dietary deficiency.
Potassium Recommendations
The National Academies of Sciences, Engineering, and Medicine set Adequate Intake (AI) levels for potassium as outlined in (Table \(\PageIndex{4}\)).1
| Age Group | Adequate Intake (mg/day) | Tolerable Upper Intake Level (mg/day) | Chronic Disease Risk Reduction Intake (CDRR) |
|---|---|---|---|
| Infants (0–6 months) | 400 | ND | ND |
| Infants (7–12 months) | 860 | ND | ND |
| Children (1–3 years) | 2,000 | ND | ND |
| Children (4–8 years) | 2,300 | ND | ND |
| Children (9–13 years) | 2,500 (males), 2,300 (females) | ND | ND |
| Adolescents (14–18 years) | 3,000 (males), 2,300 (females) | ND | ND |
| Adults (> 19 years) | 3,400 (males), 2,600 (females) | ND | ND |
| ND = not determined | |||
Sources of Potassium
Fruits and vegetables that contain high amounts of potassium are spinach, lettuce, broccoli, peas, tomatoes, potatoes, bananas, apples, and apricots. Whole grains and seeds, certain fish (such as salmon, cod, and flounder), and meats are also high in potassium. The Dietary Approaches to Stop Hypertension (DASH) Eating Plan that you learned about in Chapter 2 emphasizes potassium-rich foods.
Phosphorus
Phosphorus is the primary negatively-charged ion/electrolyte in the intracellular fluid. It is typically found in the form of hydrogen phosphate (HPO42-).
Functions of Phosphorus
Like other nutrients in this section, phosphorus assists with maintaining fluid balance. In addition, phosphorus plays a critical role in bone formation; regulates biochemical pathways by activating or deactivating enzymes; is found in ATP (adenosine triphosphate), DNA (deoxyribonucleic acid), and RNA (ribonucleic acid); and is a component of cell membranes (as phospholipids) and lipoproteins.
Imbalances of Phosphorus
Deficiencies of phosphorus are rare but can occur with vitamin D deficiency or over-secretion of parathyroid hormone. On the other hand, high blood phosphorus can occur with kidney disease, taking excessive amounts of vitamin D supplements, or taking too many phosphorus-containing antacids. Too much phosphorus can lead to muscle spasms and convulsions.
Phosphorus Recommendations
The National Academies of Sciences, Engineering, and Medicine set the Dietary Reference Intake levels for phosphorus as outlined in (Table \(\PageIndex{5}\)).4
| Age Group | Recommended Dietary Allowance (mg/day) | Tolerable Upper Intake Level (g/day) |
|---|---|---|
| Infants (0–6 months) | 100* | ND |
| Infants (7–12 months) | 275* | ND |
| Children (1–3 years) | 460 | 3 |
| Children (4–8 years) | 500 | 3 |
| Children (9–13 years) | 1,250 | 4 |
| Adolescents (14–18 years) | 1,250 | 4 |
| Adults (19 - 70 years) | 700 | 4 |
| Adults (> 70 years) | 700 | 3 |
| * denotes Adequate Intake; ND = not determined | ||
Sources of Phosphorus
Phosphorus is found in many foods and is found in high amounts in foods that contain protein (e.g., meat, milk, eggs).
Key Takeaways
- Sodium is the primary positively-charged ion in extracellular fluid.
- Sodium helps regulate fluid balance and plays important roles in nerve transmission, muscle contraction, and nutrient absorption and reabsorption.
- Most sodium in the typical American diet comes from processed and prepared foods.
- Chloride is the primary negatively-charged ion in extracellular fluid.
- Chloride aids in fluid balance by helping to maintain charge neutrality. Chloride channels also play a role in regulating fluid secretion, such as the flow of pancreatic juice into the small intestine and the flow of water into mucus.
- Potassium is the primary positively-charged ion in intracellular fluid.
- Potassium has multiple functions including its role in regulating fluid balance and nerve transmission.
- Fruits, vegetables, and whole grains tend to be good sources of potassium.
- Phosphorus is the primary negatively-charged ion/electrolyte in the intracellular fluid.
- Phosphorus is found in many foods and is found in high amounts in foods that contain protein (e.g., meat, milk, eggs).
References
- National Academies of Sciences, Engineering, and Medicine. 2019. Dietary Reference Intakes for Sodium and Potassium. Washington, DC: The National Academies Press. https://doi.org/10.17226/25353.
- US Food and Drug Administration. Food Labeling Guide. Last updated January 2013. https://www.fda.gov/media/81606/download. Accessed June 6, 2020.
- Institute of Medicine. 2005. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate. Washington, DC: The National Academies Press. https://doi.org/10.17226/10925.
- Institute of Medicine. 1997. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington, DC: The National Academies Press. https://doi.org/10.17226/5776.