
10.3: Minerals Important for Metabolism and Blood Function
- Page ID
- 21166
Learning Objectives
- Identify the primary function of each of the minerals involved in metabolism.
- Summarize the roles of minerals important in blood function.
- Identify iron-deficiency anemia as the most prevalent nutritional deficiency worldwide.
Minerals are cofactors for hundreds of enzymes involved in metabolism. In addition, several minerals are critical for proper blood function. Interestingly, the mineral content of foods is greatly affected by the soil from which it grew, and thus geographic location is the primary determinant of the mineral content of foods. For instance, iodine comes mostly from seawater so the greater the distance from the sea the lesser the iodine content in the soil.
Magnesium
Magnesium is a macromineral (major mineral) that participates as a cofactor in hundreds of metabolic reactions. ATP exists as a complex with magnesium and therefore this mineral is involved in all reactions that synthesize or require ATP including carbohydrate, lipid, protein, RNA, and DNA synthesis. Many Americans do not get the recommended intake of magnesium from their diets. Some observational studies suggest mild magnesium deficiency is linked to increased risk for cardiovascular disease. Signs and symptoms of severe magnesium deficiency may include tremor, muscle spasms, loss of appetite, and nausea. Magnesium is also involved with bone health; the DRIs and good food sources for magnesium can be found in Chapter 9.
Iron
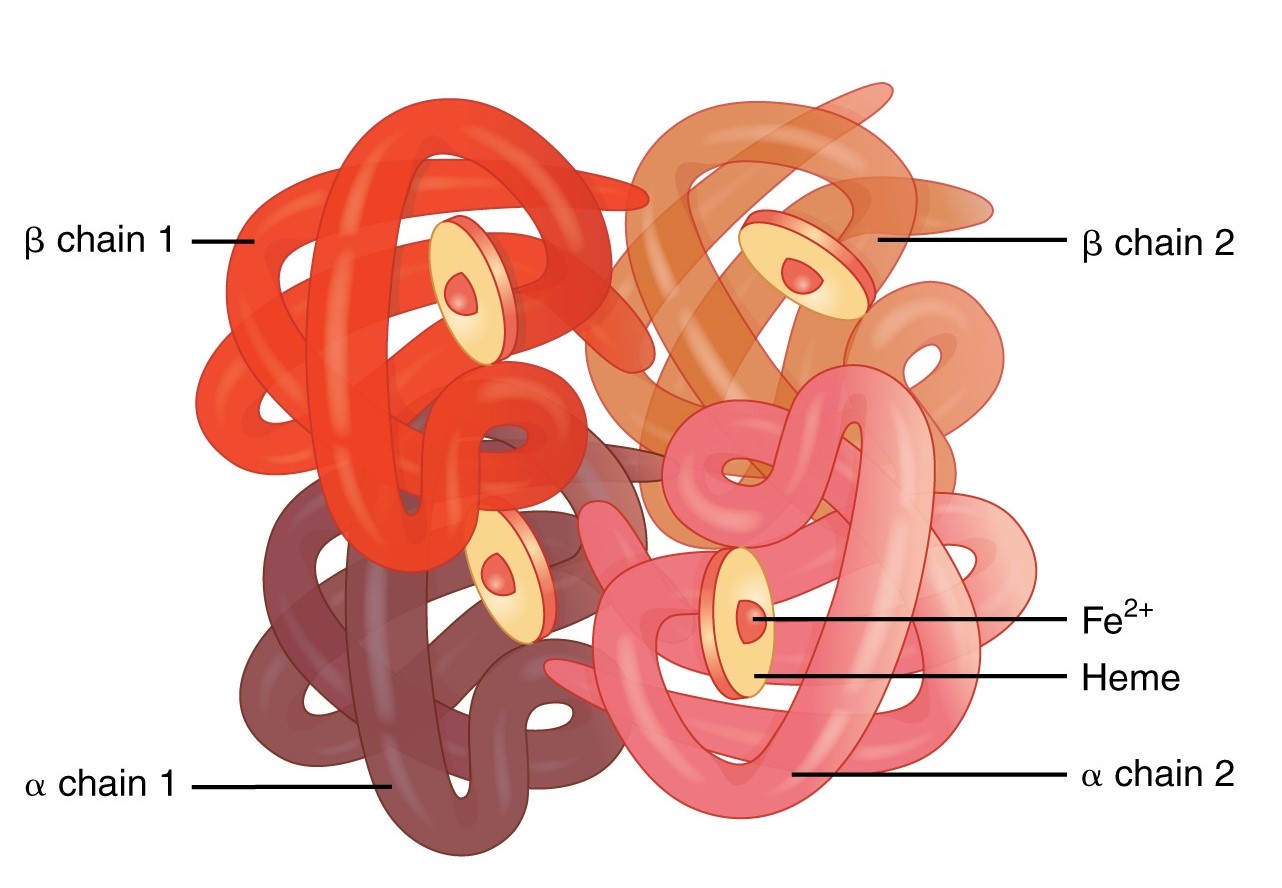
Red blood cells contain the oxygen-carrier protein hemoglobin. It is composed of four globular peptides, each containing a heme complex. Iron (Fe2+) lies in the center of each heme complex (Figure \(\PageIndex{1}\)). Iron is a trace mineral and a key component of hundreds of metabolic enzymes. Iron is also involved in numerous metabolic reactions that take place mainly in the liver and detoxify harmful substances. The great majority of iron used in the body is recycled from the continuous breakdown of red blood cells.
Oxygen transport is one of the main functions of iron. The iron in hemoglobin binds to oxygen in the capillaries of the lungs and transports it to cells where the oxygen is released. If iron levels are low, hemoglobin is not synthesized in sufficient amounts and the oxygen-carrying capacity of red blood cells is reduced, resulting in anemia. When iron levels are low in the diet the small intestine more efficiently absorbs iron in an attempt to compensate for the low dietary intake, but this process cannot make up for the excessive loss of iron that occurs with chronic blood loss or low intake. When blood cells are decommissioned for use, the body recycles the iron back to the bone marrow where red blood cells are made. The body stores some iron in the bone marrow, liver, spleen, and skeletal muscle. A relatively small amount of iron is excreted when cells lining the small intestine and skin cells die and in blood loss, such as during menstrual bleeding. The lost iron must be replaced from dietary sources.
The bioavailability of iron (ability for your body to absorb and use iron) is highly dependent on the source of the iron. Foods have two types of iron: heme iron and non-heme iron. Heme iron is found only in animal-based foods. Non-heme iron is found in plant-based and animal-based foods. Heme iron is more bioavailable than nonheme iron. In addition, some plants contain chemicals (such as phytates, oxalates, tannins, and polyphenols) that inhibit iron absorption. However, eating fruits and vegetables rich in vitamin C at the same time as iron-containing foods markedly increases iron absorption. In addition, cooking foods in an iron skillet can increase the iron content of the cooked food. Iron toxicity can cause symptoms such as nausea, vomiting, diarrhea, dizziness, and confusion. In the United States, iron overdose is the most common cause of poisoning deaths in children younger than 6, so iron supplements should be stored out of children's reach. The DRIs for iron are listed in Table \(\PageIndex{1}\). Good food sources of iron are listed in Table \(\PageIndex{2}\).
| Age Group | RDA (mg/day) | UL (mg/day) |
|---|---|---|
| Infants (0–6 months) | 0.27* | 40 |
| Infants (7–12 months) | 11 | 40 |
| Children (1–3 years) | 7 | 40 |
| Children (4–8 years) | 10 | 40 |
| Children (9–13 years) | 8 | 40 |
| Adolescents (14–18 years) | 11 (males), 15 (females) | 45 |
| Adults (19-30 years) | 8 (males), 18 (females) | 45 |
| Adults (31-50 years) | 8 (males), 18 (females) | 45 |
| Adults (> 50 years) | 8 | 45 |
| * denotes Adequate Intake | ||
| Food | Iron (mg) | % Daily Value |
|---|---|---|
| Oysters (3 ounces) | 8 | 44 |
| White beans, canned (1 cup) | 8 | 44 |
| Chocolate, dark, 45-69% cacao (3 ounces) | 7 | 39 |
| Beef liver (3 ounces) | 5 | 28 |
| Spinach, boiled (1/2 cup) | 3 | 17 |
Learn even more about this nutrient by reading the Iron Fact Sheet from the National Institutes of Health, Office of Dietary Supplements.
Iron-Deficiency Anemia
Iron-deficiency anemia is the most common and widespread nutritional disorder in the world.3 It's a condition that develops from having insufficient iron levels in the body resulting in fewer and smaller red blood cells containing lower amounts of hemoglobin. Iron-deficiency anemia has the following signs and symptoms, which are linked to the essential functions of iron in energy metabolism and blood health:
- Fatigue
- Weakness
- Pale skin
- Shortness of breath
- Dizziness
- Swollen, sore tongue
- Abnormal heart rate
Iron-deficiency anemia is diagnosed from characteristic signs and symptoms and confirmed with simple blood tests that count red blood cells and determine hemoglobin and iron content in blood. Anemia is most often treated with iron supplements and increasing the consumption of foods that are higher in iron.
Infants, children, adolescents, and women are the populations most at risk worldwide for iron-deficiency anemia. Infants, children, and teens require more iron because iron is essential for growth. In these populations, iron deficiency (and eventually iron-deficiency anemia) can also cause the following signs and symptoms: poor growth, failure-to-thrive, and poor performance in school, as well as mental, motor, and behavioral disorders. Women who experience heavy menstrual bleeding or who are pregnant require more iron in the diet. One more high-risk group is the elderly. Both elderly men and women have a high incidence of anemia and the most common causes are dietary iron deficiency and chronic disease such as ulcer, inflammatory diseases, and cancer. Additionally, those who have recently suffered from traumatic blood loss, frequently donate blood, or take excessive antacids for heartburn need more iron in the diet. For more on anemia, watch the following video from the Khan Academy:
"What is Anemia?" (CC BY-NC-SA 4.0 by Nauroz Syed for Khan Academy)
Zinc
Zinc is a trace mineral and a cofactor for over two hundred enzymes in the human body and plays a direct role in RNA, DNA, and protein synthesis. Zinc is a required cofactor for an enzyme that synthesizes the heme portion of hemoglobin and severely deficient zinc diets can result in anemia. Zinc is also a cofactor for enzymes involved in energy metabolism. Zinc also performs structural functions - it helps stabilize the structure of proteins involved in gene expression, vision, antioxidant enzyme systems, and immune function. In addition, zinc regulates gene expression (e.g., activates cells that regulate cell growth during fetal development). As the result of its prominent roles in anabolic and energy metabolism, a zinc deficiency in infants and children limits growth. In adults, severe zinc deficiency can cause hair loss, diarrhea, skin sores, loss of appetite, and weight loss. Toxicity can occur from supplements; symptoms include intestinal pain, headaches, and depressed immune function. The DRIs for zinc are listed in Table \(\PageIndex{3}\). Red meat and poultry provide the majority of zinc in the American diet. Additional good food sources of zinc are listed in Table \(\PageIndex{4}\).
| Age Group | RDA (mg/day) | UL (mg/day) |
|---|---|---|
| Infants (0–6 months) | 2* | 4 |
| Infants (7–12 months) | 3 | 5 |
| Children (1–3 years) | 3 | 7 |
| Children (4–8 years) | 5 | 12 |
| Children (9–13 years) | 8 | 23 |
| Adolescents (14–18 years) | 11 (males), 9 (females) | 34 |
| Adults (> 18 years) | 11 (males), 8 (females) | 40 |
| * denotes Adequate Intake | ||
| Food | Zinc (mg) | % Daily Value |
|---|---|---|
| Beef, chuck roast (3 ounces) | 7 | 64 |
| Alaska king crab (3 ounces) | 6.5 | 59 |
| Pork chop (3 ounces) | 2.9 | 26 |
| Baked beans, canned (1/2 cup) | 2.9 | 26 |
| Chicken, dark meat (3 ounces) | 2.4 | 22 |
| Pumpkin seeds (1 ounce) | 2.2 | 20 |
Learn even more about this nutrient by reading the Zinc Fact Sheet from the National Institutes of Health, Office of Dietary Supplements.
Iodine
Iodine is a trace element essential for the synthesis of thyroid hormone, which regulates metabolism, growth, and development. Low iodine levels can lead to hypothyroidism which has many signs and symptoms including fatigue, sensitivity to cold, constipation, weight gain, depression, dry, itchy skin and paleness. The development of goiter (Figure \(\PageIndex{2}\)) may often be the most visible sign of chronic iodine deficiency, but the consequences of low levels of thyroid hormone can be severe during infancy, childhood, and adolescence as it affects all stages of growth and development. Thyroid hormone plays a major role in brain development and growth. Fetuses and infants with severe iodine deficiency develop a condition known as cretinism, in which physical and neurological impairment can be severe. Too much iodine blocks the synthesis of thyroid hormones and also results in goiter. The DRIs for iodine are listed in Table \(\PageIndex{5}\). Seaweed is one of the best food sources of iodine, but it is highly variable in its content. Seafood and dairy products are good food sources of iodine (Table \(\PageIndex{6}\)). For many people worldwide, iodized salt is the only source of iodine.

| Age Group | RDA (mcg/day) | UL (mcg/day) |
|---|---|---|
| Infants (0–6 months) | 110* | ND |
| Infants (7–12 months) | 130* | ND |
| Children (1–3 years) | 90 | 200 |
| Children (4–8 years) | 90 | 300 |
| Children (9–13 years) | 120 | 600 |
| Adolescents (14–18 years) | 150 | 900 |
| Adults (> 18 years) | 150 | 1,100 |
| * denotes Adequate Intake; ND=not determined | ||
| Food | Iodine (mcg) | % Daily Value |
|---|---|---|
| Cod, baked (3 ounces) | 158 | 106 |
| Nori, seaweed, dried (2 tablespoons) | 116 | 77 |
| Yogurt, plain, low-fat (3/4 cup) | 87 | 58 |
| Iodized salt (1/4 teaspoon) | 76 | 51 |
| Egg, hard boiled (1 large) | 26 | 17 |
| Shrimp (3 ounces) | 13 | 9 |
Learn even more about this nutrient by reading the Iodine Fact Sheet from the National Institutes of Health, Office of Dietary Supplements.
Selenium
Selenium is a trace mineral and a cofactor for enzymes that release active thyroid hormone in cells; therefore, low levels can cause similar signs and symptoms as iodine deficiency. Selenium also functions as an antioxidant; the DRIs and good food sources for selenium can be found in Chapter 8. Learn even more about this nutrient by reading the Selenium Fact Sheet from the National Institutes of Health, Office of Dietary Supplements.
Copper
Copper is a trace mineral and cofactor for enzymes essential in iron absorption and transport. The other important function of copper is as an antioxidant, which was also discussed briefly in Chapter 8. Symptoms of mild to moderate copper deficiency are rare. More severe copper deficiency can cause anemia from the lack of iron mobilization in the body for red blood cell synthesis. Other signs and symptoms include growth retardation in children and neurological problems, because copper is a cofactor for an enzyme that synthesizes myelin, which surrounds many nerves. The DRIs for copper are listed in Table \(\PageIndex{7}\). Good food sources of copper are included in (Table \(\PageIndex{8}\)).
| Age Group | RDA (mcg/day) | UL (mcg/day) |
|---|---|---|
| Infants (0–6 months) | 200* | ND |
| Infants (7–12 months) | 220* | ND |
| Children (1–3 years) | 340 | 1,000 |
| Children (4–8 years) | 440 | 3,000 |
| Children (9–13 years) | 700 | 5,000 |
| Adolescents (14–18 years) | 890 | 8,000 |
| Adults (> 18 years) | 900 | 10,000 |
| * denotes Adequate Intake; ND=not determined | ||
| Food | Copper (mcg) | % Daily Value |
|---|---|---|
| Oysters, wild, cooked (3 ounces) | 4,850 | 539 |
| Baking chocolate, unsweetened (1 ounce) | 938 | 104 |
| Potatoes (1 medium) | 675 | 75 |
| Mushrooms, shitake (1/2 cup) | 650 | 70 |
| Tofu, raw, firm (1/2 cup) | 476 | 53 |
| Pasta, whole wheat, cooked (1 cup) | 263 | 29 |
| Avocado (1/2 cup) | 219 | 24 |
Learn even more about this nutrient by reading the Copper Fact Sheet from the National Institutes of Health, Office of Dietary Supplements.
Chromium
The functioning of chromium in the body is less understood than that of most other minerals. Chromium is a trace mineral that enhances the actions of insulin and plays a role in carbohydrate, fat, and protein metabolism. More research is needed to better determine the full range of chromium's roles in the body. The Adequate Intakes (AIs) for chromium are listed in Table \(\PageIndex{9}\). A Tolerable Upper Intake Level (UL) for chromium has not been set. The chromium content of foods cannot be reliably determined, so the values presented in Table \(\PageIndex{10}\) should only be used as a guide.
| Age Group | AI (mcg/day) |
|---|---|
| Infants (0–6 months) | 0.2 |
| Infants (7–12 months) | 5.5 |
| Children (1–3 years) | 11 |
| Children (4–8 years) | 15 |
| Children (9–13 years) | 25 (males), 21 (females) |
| Adolescents (14–18 years) | 35 (males), 24 (females) |
| Adults (19-50 years) | 35 (males), 25 (females) |
| Adults (> 50 years) | 30 (males), 20 (females) |
| Food | Chromium (mcg) | % Daily Value |
|---|---|---|
| Broccoli (1/2 cup) | 11 | 31 |
| Grape juice (1 cup) | 8 | 23 |
| English muffin, whole wheat (1) | 4 | 11 |
| Potatoes, mashed (1 cup) | 3 | 9 |
Learn even more about this nutrient by reading the Chromium Fact Sheet from the National Institutes of Health, Office of Dietary Supplements.
Mineral Summary
A summary of the prominent functions of minerals involved in metabolism and blood function as well as their related deficiency syndromes is given in Table \(\PageIndex{11}\).
| Mineral | Function | Deficiency: Signs and Symptoms |
|---|---|---|
| Macro | ||
| Magnesium | ATP synthesis and utilization, carbohydrate, lipid, protein, RNA, and DNA synthesis | Tremor, muscle spasms, loss of appetite, nausea |
| Trace | ||
| Iron | Assists in energy production, DNA synthesis required for red blood cell function | Anemia: fatigue, paleness, faster heart rate |
| Zinc | Assists in energy production, protein, RNA and DNA synthesis; required for hemoglobin synthesis | Growth retardation in children, hair loss, diarrhea, skin sores, loss of appetite, weight loss |
| Iodine | Making thyroid hormone, metabolism, growth and development | Goiter, cretinism, other signs and symptoms include fatigue, depression, weight gain, itchy skin, low heart-rate |
| Selenium | Essential for thyroid hormone activity | fatigue |
| Copper | Assists in energy production, iron metabolism | Anemia: fatigue, paleness, faster heart rate |
| Chromium | Assists insulin in carbohydrate, lipid and protein metabolism | abnormal glucose metabolism |
Mineral Bioavailability
Minerals are not as efficiently absorbed as most vitamins and so the bioavailability of minerals (ability for your body to absorb and use minerals) can be very low. Plant-based foods often contain factors, such as oxalates and phytates, that bind to minerals and inhibit their absorption. In general, minerals are better absorbed from animal-based foods. In most cases, if dietary intake of a particular mineral is increased, absorption will decrease. Some minerals influence the absorption of others. For instance, excess zinc in the diet can impair iron and copper absorption. Conversely, certain vitamins enhance mineral absorption. For example, vitamin C boosts iron absorption, and vitamin D boosts calcium and magnesium absorption. As is the case with vitamins, certain gastrointestinal disorders and diseases, such as Crohn’s disease and kidney disease, as well as the aging process, impair mineral absorption, putting people with malabsorption conditions and the elderly at higher risk for mineral deficiencies.
Key Takeaways
- Minerals are cofactors for hundreds of enzymes involved in metabolism.
- Iron, copper and zinc are critical for blood function.
- Iron-deficiency anemia is a condition that develops from having insufficient iron levels in the body, resulting in fewer and smaller red blood cells containing lower amounts of hemoglobin. Anemia is most often treated with iron supplements and increasing the consumption of foods that are higher in iron.
- Infants, children, adolescents, and women are the populations most at risk worldwide for iron-deficiency anemia by all causes.
- Minerals are not as efficiently absorbed as most vitamins and bioavailability can be very low.
References
- Summary Report of the Dietary Reference Intakes. nationalacademies.org. www.nationalacademies.org/our-work/summary-report-of-the-dietary-reference-intakes. Accessed July 5, 2020.
- Iron - Health Professional Fact Sheet. ods.od.nih.gov. https://ods.od.nih.gov/factsheets/Iron-HealthProfessional/. Accessed July 5, 2020.
- Micronutrient deficiencies. who.int. https://www.who.int/nutrition/topics/ida/en/. Accessed July 5, 2020.
- Zinc - Health Professional Fact Sheet. ods.od.nih.gov. https://ods.od.nih.gov/factsheets/Zinc-HealthProfessional/. Accessed July 5, 2020.
- Iodine - Health Professional Fact Sheet. ods.od.nih.gov. https://ods.od.nih.gov/factsheets/Iodine-HealthProfessional/. Accessed July 21, 2022.
- USDA, FDA and ODS-NIH Database for the Iodine Content of Common Foods Release 2.0 (2022). ars.usda.gov. https://www.ars.usda.gov/ARSUSERFILES/80400535/DATA/IODINE/IODINE_DATABASE_RELEASE_2_PER_SERVING.PDF. Accessed July 21, 2022.
- Copper - Health Professional Fact Sheet. ods.od.nih.gov. https://ods.od.nih.gov/factsheets/Copper-HealthProfessional/. Accessed July 5, 2020.
- Chromium - Health Professional Fact Sheet. ods.od.nih.gov. https://ods.od.nih.gov/factsheets/Chromium-HealthProfessional/. Accessed July 5, 2020.