
12.1: Pregnancy and Nutrition
- Page ID
- 21178
Learning Objectives
- Identify weight gain recommendations for pregnancy.
- Discuss nutritional requirements and concerns during pregnancy.
- Explore the relationship between fetal development and nutritional choices.
- Describe various discomforts and complications of pregnancy.
It is crucial to consume healthy foods at every phase of life, beginning in the womb. Good nutrition is vital for any pregnancy and not only helps an expectant parent remain healthy, but also impacts the development of the fetus and ensures that the baby thrives in infancy and beyond. During pregnancy, there is an increased need for certain nutrients. If these nutritional needs are not met, infants could suffer from low birth weight (a birth weight less than 5.5 pounds or 2,500 grams), among other developmental problems. Therefore, it is crucial to make careful dietary choices during pregnancy.
The Early Days of Pregnancy
For medical purposes, pregnancy is measured from the first day of a person’s last menstrual period until childbirth, and typically lasts 38-42 weeks. Pregnancy is divided into trimesters, with each trimester lasting 13-14 weeks. At conception, a sperm cell fertilizes an egg cell, creating a zygote. The zygote implants itself in the uterine wall and rapidly divides into multiple cells to become an embryo. The embryo develops organs, limb buds, and facial features. Embryos are extremely vulnerable to teratogens during this time; exposure to teratogens can cause birth defects and/or spontaneous abortion (miscarriage). At week 8 the embryo transitions to being called a fetus. Another important development during the first trimester is the development of the placenta which is responsible for oxygen, nutrient, and waste exchange between the mom and the fetus (via the umbilical cord). Major changes begin to occur in the earliest days, often weeks before a person even knows that they are pregnant. During this period, adequate nutrition supports cell division, tissue differentiation, and organ development. As each week passes, new milestones are reached. Therefore, people who are trying to conceive should make proper dietary choices to ensure the delivery of a healthy baby. All parents-to-be should consider their eating habits; a sedentary lifestyle and a diet low in fresh fruits and vegetables may affect fertility.
A pregnancy may happen unexpectedly. Therefore, it is important for all people who have the potential to get pregnant and are of childbearing age to get 400 micrograms of folate per day prior to pregnancy and 600 micrograms per day during pregnancy. Folate, which is also known as folic acid, is crucial for the production of DNA and RNA and the synthesis of cells. A deficiency can cause megaloblastic anemia (the development of abnormal red blood cells) during pregnancy. It can also have a profound effect on the unborn baby. Typically, folate intake has the greatest impact during the first eight weeks of pregnancy, when the neural tube closes. The neural tube develops into the fetus’s brain, and adequate folate reduces the risk of brain abnormalities or neural tube defects. This vital nutrient also supports the spinal cord and its protective coverings. As discussed in Chapter 10, inadequate folate can result in birth defects, such as spina bifida, which is the failure of the spinal column to close. Leafy green vegetables (such as spinach and kale) and legumes (such as lentils) are good sources of folate. Additionally, since 1998, food manufacturers have been required to add folate to cereals and other grain products. The required addition of folate has helped reduce the number of neural tube defects and was an important solution, especially since many people don't know that they're pregnant until after the neural tube closes.
Weight Gain during Pregnancy
During pregnancy, the body changes in many ways. One of the most notable and significant changes is weight gain. If a pregnant person does not gain enough weight, their unborn baby will be at risk. Poor weight gain, especially in the third trimester, could result not only in low birth weight, but also infant mortality and intellectual disabilities. Therefore, it is vital for a pregnant person to maintain a healthy weight. The amount of weight that should be gained during pregnancy is based on their pre-pregnancy body mass index (BMI). See Table \(\PageIndex{1}\) for the Institute of Medicine (IOM) recommendations.
| Prepregnancy BMI | Weight Category | Recommended Weight Gain |
|---|---|---|
| Below 18.5 | Underweight | 28–40 pounds |
| 18.5–24.9 | Normal weight | 25–35 pounds |
| 25.0–29.9 | Overweight | 15–25 pounds |
| 30.0 and above | Obese | 11–20 pounds |
A pre-pregnancy weight below or above the normal weight range can lead to different complications. Pregnant people with a pre-pregnancy BMI below 18.5 are at higher risk of a premature birth and delivering a low birth weight infant.2 Those with a pre-pregnancy BMI above 30 have an increased risk for gestational diabetes, preeclampsia (high blood pressure during pregnancy), cesarean delivery, and macrosomia (larger baby than normal).3 Therefore, it is optimal to have a BMI in the normal range prior to pregnancy.
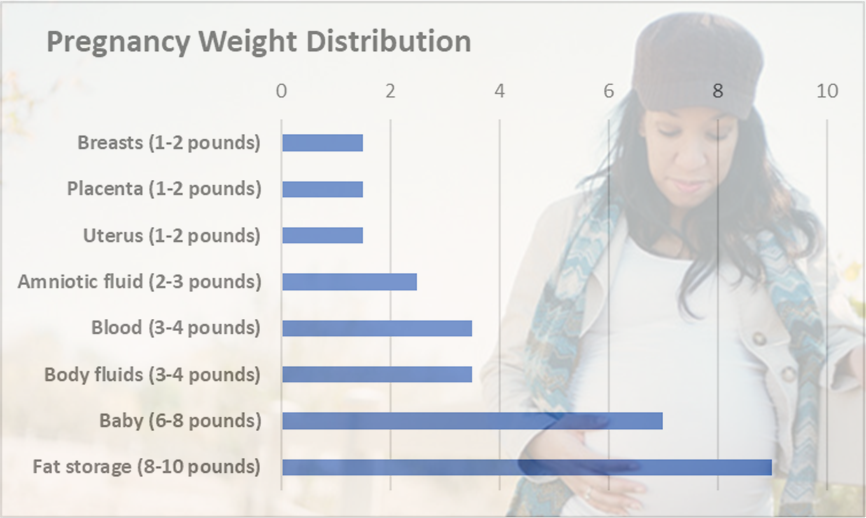
During the first trimester, pregnant people generally gain 3-5 pounds. During the 2nd and 3rd trimesters, gaining about 1 pound a week is considered healthful. Some of the new weight is due to the growth of the fetus, while some is due to changes in the parent’s body that support the pregnancy. For example, the placenta supplies nutrients to the fetus and removes waste products; the amniotic sac contains fluids that surround and cushion the fetus. The approximate distribution of weight gained during pregnancy can be seen in Figure \(\PageIndex{1}\). Those who are pregnant with more than one fetus are advised to gain even more weight to ensure the health of their unborn babies.
Preterm babies are born before 38 weeks and may be low birth weight or very low birth weight babies. In addition, an undernourished mother is more likely to give birth to a low-birth weight baby. Low birth weight and very low birth weight babies are at increased risk of infections, learning disabilities, impaired physical development, and death in the first year of life.
- Low birth weight: any baby born weighing less than 5.5 pounds
- Very low birth weight: any baby born weighing less than 3.3 pounds
Weight Loss after Pregnancy
During labor, some of the weight gained during pregnancy is lost with the delivery of the child. In the following weeks, the birthing parent continues to shed weight as they lose accumulated fluids and their blood volume returns to normal. Those who gain a healthy amount of weight and participate in regular physical activity during their pregnancies also have an easier time shedding weight post-pregnancy. However, people who gain more weight than needed for a pregnancy typically retain that excess weight as body fat which can lead to complications such as high blood pressure or Type 2 diabetes in future pregnancies or later in life.
Nutritional Requirements During Pregnancy
As a pregnant person's body changes, so do their nutritional needs. Pregnant people must consume more calories and nutrients in the 2nd and 3rd trimesters than non-pregnant adults. However, the average recommended daily caloric intake can vary depending on activity level and the person’s pre-pregnancy weight. Choosing nutrient-dense foods helps ensure nutrient needs during pregnancy are met. It is also standard to take prenatal supplements during pregnancy to ensure adequate intake of the needed micronutrients.
Energy
During the first trimester, a pregnant person has the same energy requirements as normal and should consume the same number of calories as usual. However, as the pregnancy progresses, caloric intake must increase. During the 2nd and 3rd trimesters, caloric needs increase by 350-450 calories per day. This is partly due to an increase in metabolism, which rises during pregnancy and contributes to increased energy needs. These increased needs can easily be met by consuming more nutrient-dense foods. For example, an additional 350 calories could include a large banana (about 120 calories), a cup of low-fat plain yogurt (about 170 calories), and a slice of whole-wheat toast (about 60 calories).
Carbohydrates
The recommended daily allowance, or RDA, of carbohydrates during pregnancy is about 175-265 grams per day to fuel fetal brain development. The best nutrient-dense carbohydrate food sources include whole-grain breads and cereals, brown rice, root vegetables, legumes, and fruits. These and other unrefined carbohydrates provide nutrients, phytochemicals, antioxidants, and fiber. These foods also help to build the placenta and supply energy for the growth of the unborn baby.
Protein
During pregnancy, extra protein is needed for the synthesis of new tissues. Protein builds muscle and other tissues, enzymes, antibodies, and hormones in both the birthing parent and the unborn baby. Additional protein also supports increased blood volume and the production of amniotic fluid. The RDA for protein during pregnancy is 1.1 grams per kilogram per day, which is about 25 grams above the normal recommendation. However, in most instances, there is no need to make an effort to increase protein intake as long as the pregnant person has a normal appetite, because even non-pregnant people in North America typically eat that much protein. Protein should be derived from healthy sources, such as lean meats, legumes, nuts, seeds, eggs, and fish. Low-fat dairy products also provide protein, along with calcium and other nutrients.
Fat
During pregnancy, fats should make up 20-35% of daily calories. A very low-fat diet is not recommended during pregnancy since it would be hard to meet the needs of essential fatty acids and fat-soluble vitamins. Recommendations for omega-3 and omega-6 essential fatty acids increase during pregnancy. These essential fatty acids are important during pregnancy because they support the baby’s brain and eye development. In particular, the brain depends on omega-3 and omega-6 fatty acids for function, structure, and growth. Docosahexaenoic acid (DHA; an omega-3 fatty acid) and arachidonic acid (ARA; an omega-6 fatty acid) have been linked to enhanced brain growth and eye development. Good sources of DHA include oily fish such as salmon, sardines, anchovies, and mackerel. Good sources of ARA include meat, fish, and poultry. Additional sources of omega-3 and omega-6 fats can be found in Chapter 5.
Fiber
Ideally, a pregnant person should eat 28 grams of dietary fiber per day. Recall from Chapter 4 that there are two types of fiber. Insoluble fiber acts as a natural laxative, which softens stools and speeds the elimination of waste material through the colon to avoid constipation. Sources of insoluble fiber include whole grains, fruits, vegetables, dried peas, and beans. Soluble fiber has little effect on the intestines, however it helps to lower blood-cholesterol levels and regulate blood glucose. Sources of soluble fiber include fruits, vegetables, and beans, along with oats, barley, and other fiber-filled whole grains.
Vitamins and Minerals
Pregnancy requires certain conditionally essential nutrients, which are nutrients that are required in higher amounts only under special conditions, such as stress, illness, or aging. The daily requirements change with the onset of a pregnancy. Taking a daily prenatal supplement or multivitamin helps to meet many nutritional needs. However, many of these requirements can be fulfilled with a nutrient-dense diet. Table \(\PageIndex{2}\) compares the normal levels of required vitamins and minerals to the levels needed during pregnancy. It's important to note that during pregnancy, the DRI for nearly all vitamins and minerals increases.
| Nutrient | Non-pregnancy Recommendation | Recommendation during Pregnancy |
|---|---|---|
| Vitamin A (mcg) | 700 | 770 |
| Vitamin B6 (mg) | 1.3 | 1.9 |
| Vitamin B12 (mcg) | 2.4 | 2.6 |
| Vitamin C (mg) | 75 | 85 |
| Vitamin D (mcg) | 15 | 15 |
| Vitamin E (mg) | 15 | 15 |
| Calcium (mg) | 1,000 | 1,000 |
| Folate (mcg dietary folate equivalents; mcg DFE) | 400 | 600 |
| Iron (mg) | 18 | 27 |
| Magnesium (mg) | 320 | 360 |
| Niacin (B3) (mg) | 14 | 18 |
| Phosphorus (mg) | 700 | 700 |
| Riboflavin (B2) (mg) | 1.1 | 1.4 |
| Thiamin (B1) (mg) | 1.1 | 1.4 |
| Zinc (mg) | 8 | 11 |
The micronutrients involved with building the skeleton—vitamin D, calcium, phosphorus, and magnesium—are crucial during pregnancy to support fetal bone development. Although the levels are the same (or very similar) during both non-pregnancy and pregnancy, many individuals do not typically consume adequate amounts and should make an extra effort to meet those needs during pregnancy.
There is an increased need for several vitamins and minerals during pregnancy. Adequate vitamin B6 supports the metabolism of amino acids, while more vitamin B12 is needed for the synthesis of red blood cells and DNA. Additional zinc is crucial for cell development and protein synthesis. Extra iron intake is important because of the increase in blood supply during pregnancy and to support the fetus and placenta. In addition, during the 3rd trimester, the fetus stores iron for use during the first few months after birth. Iron is the one micronutrient that is almost impossible to obtain in adequate amounts from food sources only. Therefore, even if a pregnant person consumes a healthy diet, there is still typically a need to take an iron supplement. Also, remember that folate needs increase during pregnancy to 600 micrograms DFE per day to prevent neural tube defects, assist with cell division, and to help produce the extra blood a pregnant body requires.
Those who are pregnant should avoid exceeding any vitamin or mineral recommendations. Taking megadose supplements can lead to excessive amounts of certain micronutrients, such as vitamin A and zinc, which may produce toxic effects that can also result in birth defects.
Guide to Eating during Pregnancy
While pregnant people have an increased need for energy, vitamins, and minerals, energy increases are proportionally less than other macronutrient and micronutrient increases. So, nutrient-dense foods, which have a higher proportion of macronutrients and micronutrients relative to calories, are essential to a healthy diet during pregnancy. Examples of nutrient-dense foods include fruits, vegetables, whole grains, legumes (beans), reduced-fat dairy, and lean meats. Those who are pregnant should be able to meet almost all of their increased needs with a nutrient-dense diet. However, a prenatal supplement should be taken to ensure an adequate intake of iron and folate.
Foods to Avoid
A number of substances can harm a growing fetus; therefore, it is vital to avoid them throughout a pregnancy. Some substances are so detrimental that they should be avoided even if there's a suspicion of being pregnant. For example, consumption of alcoholic beverages results in a range of abnormalities that fall under the umbrella of fetal alcohol spectrum disorders. They include learning and attention deficits, heart defects, and abnormal facial features. Alcohol enters the unborn baby via the umbilical cord and can slow fetal growth, damage the brain, or even result in miscarriage. The effects of alcohol are most severe in the first trimester, when the organs are developing. As a result, there is no safe amount of alcohol that a pregnant person can consume.
Caffeine is a stimulant that crosses the placenta and reaches the fetus. Caffeine may increase the risk of miscarriage and low birth weight. Pregnant people should limit caffeine intake, which is found not only in coffee, but also tea, sodas, chocolate, and energy drinks. Current recommendations suggest limiting caffeine to less than 200 milligrams a day (which is the amount in 12 ounces of brewed coffee).5
Foodborne Illness
For both the birthing parent and the fetus, foodborne illness can cause major health problems. For example, the foodborne illness caused by the bacteria Listeria monocytogenes can cause preterm labor or miscarriages. Those who are pregnant are more likely to become infected with this disease, which is known as listeriosis, than non-pregnant, healthy adults.6 Foods more likely to contain the bacteria are unpasteurized dairy products, especially soft cheeses, and also smoked seafood, hot dogs, paté, cold cuts, and uncooked meats. To avoid consuming contaminated foods, people who are pregnant or breastfeeding should take the following measures:
- Thoroughly rinse fruits and vegetables before eating them
- Keep cooked and ready-to-eat food separate from raw meat, poultry, and seafood
- Store food at 40° F (4° C) or below in the refrigerator and at 0° F (−18° C) in the freezer
- Refrigerate perishables, prepared food, or leftovers within two hours of preparation or eating
- Clean the refrigerator regularly and wipe up any spills right away
- Check the expiration dates of stored food once per week
You will learn more about foodborne illness and its consequences in Chapter 14.
Food Contaminants
It is always important to avoid consuming contaminated food. This is especially true during pregnancy. Heavy metal contaminants, particularly mercury, lead, and cadmium, pose risks to those who are pregnant. Some fish contain high levels of mercury. As a result, there are guidelines related to fish intake during pregnancy. Pregnant people can eat fish, ideally 8 to 12 ounces of a variety of seafood per week, from choices that are lower in mercury. Figure \(\PageIndex{2}\) includes good and best choices of seafood that are lower in mercury. In addition, the figure identifies fish with high mercury levels, such as shark, swordfish, tilefish, marlin, orange roughy, bigeye tuna, and king mackerel that should be avoided.

Physical Activity during Pregnancy
Physical activity during pregnancy is recommended in the Physical Activity Guidelines for Americans. People should do at least 150 minutes (2 hours and 30 minutes) of moderate-intensity aerobic activity a week during pregnancy and the postpartum period. Preferably, aerobic activity should be spread throughout the week. People who habitually engaged in vigorous-intensity aerobic activity or who were physically active before pregnancy can continue these activities during pregnancy and the postpartum period.7 Physical activity during pregnancy reduces the risk of gestational diabetes, preeclampsia, preterm birth, and large for gestational age infants. In addition, physical activity can enhance mood, reduce lower back pain and shorten labor.
Common Discomforts during Pregnancy
Pregnancy can lead to certain discomforts, from back strain to swollen ankles. A pregnant person is likely to experience constipation because increased hormone levels can slow digestion and relax muscles in the bowels. Constipation and pressure from growth of the uterus can result in hemorrhoids, which are another common discomfort. Getting mild to moderate exercise and drinking enough fluids can help prevent both conditions. Also, eating a high-fiber diet softens the stools and reduces the pressure on hemorrhoids.
Heartburn (gastroesophageal reflux) can occur during the early months of pregnancy due to an increase in the hormone progesterone, and during the later months due to the expanding size of the fetus, which limits stomach contraction. Avoiding foods that cause heartburn and remaining upright for an hour after meals can help pregnant people avoid heartburn. In addition, it can be helpful to drink fluids between meals, instead of with food.
Other common complaints can include leg cramps and bloating. Regular exercise can help to alleviate these discomforts. Many pregnant people develop gastrointestinal issues, such as nausea and vomiting. Many also experience food cravings and aversions. All of these can impact a pregnant person’s nutritional intake and it is important to protect against adverse effects.
Nausea and Vomiting
Nausea and vomiting are gastrointestinal issues that strike many pregnant people, typically in the first trimester. Nausea tends to occur more frequently than vomiting. These conditions are often referred to as “morning sickness,” although that’s something of a misnomer because nausea and vomiting can occur all day long, although it is often the worst in the first part of the day.
Increased levels of hormones may cause nausea and vomiting. Nausea usually subsides after 16 weeks, possibly because the body becomes adjusted to higher hormone levels.
It can be useful for those who are pregnant to keep a food diary to discover which foods trigger nausea, so they can avoid them in the future. Other tips to help avoid or treat nausea and vomiting include the following:
- Avoid spicy foods
- Avoid strong or unusual odors
- Eat dry cereal, toast, or crackers
- Eat frequent, small meals
- Consume more unrefined carbohydrates
- Get moderate aerobic exercise
- Drink ginger tea, which aids in stomach upset
- Seek fresh air when a bout of nausea comes on
A severe form of nausea and vomiting is a condition known as hyperemesis gravidarum. It is marked by prolonged vomiting, which can result in dehydration and require hospitalization.
Food Cravings and Aversions
Food aversions and cravings do not have a major impact unless food choices are extremely limited. Some common food aversions include meat, eggs, milk, and spicy foods. During pregnancy, it is not harmful to indulge in the occasional craving, such as the desire for chocolate or ice cream. A medical disorder known as pica is willingly consuming foods with little or no nutritive value, such as dirt, clay, or soap. In some places this is a culturally accepted practice. However, it can be harmful if these substances take the place of nutritious foods or contain toxins.
Complications during Pregnancy
Different complications may arise during the course of a pregnancy. These complications include certain medical conditions that could greatly impact a pregnancy if left untreated, such as gestational hypertension and gestational diabetes, which have diet and nutrition implications.
Gestational Hypertension
Gestational hypertension is a condition of high blood pressure during the second half of pregnancy. First-time birthing parents are at a greater risk, along with those who have parents or siblings who had gestational hypertension, those carrying multiple fetuses, those with a prior history of high blood pressure or kidney disease, and people who are overweight or obese when they become pregnant.
Hypertension can prevent the placenta from getting enough blood, which would result in the baby getting less oxygen and nutrients. This can result in low birth weight, although most people with gestational hypertension can still deliver a healthy baby if the condition is detected and treated early. Some risk factors can be controlled, such as diet, while others cannot, such as family history. If left untreated, gestational hypertension can lead to a serious complication called preeclampsia. This disorder is marked by elevated blood pressure and protein in the urine and is associated with swelling (edema) and unexplained rapid weight gain. To prevent preeclampsia, the WHO recommends increasing calcium intake for pregnant people consuming diets low in calcium and administering a low dosage of aspirin (75 milligrams) among other interventions.8
Gestational Diabetes
About 4% of pregnant people suffer from a condition known as gestational diabetes, which is abnormal glucose tolerance during pregnancy. The body becomes resistant to the hormone insulin, which enables cells to transport glucose from the blood. Gestational diabetes is usually tested for and diagnosed near the end of the 2nd trimester, although it is possible for the condition to develop later into a pregnancy. Signs and symptoms of this disease include extreme hunger, thirst, or fatigue. If blood sugar levels are not properly monitored and treated, the baby might gain too much weight and require a cesarean delivery. Diet and regular physical activity can help to manage this condition. Most patients who suffer from gestational diabetes also require daily insulin injections to boost the absorption of glucose from the bloodstream and promote the storage of glucose in the form of glycogen in liver and muscle cells. Gestational diabetes usually resolves after childbirth, although some people who suffer from this condition develop Type 2 diabetes later in life, particularly if they are overweight.
Key Takeaways
- Pre-pregnancy BMI determines how much weight a person needs to gain throughout their pregnancy.
- During pregnancy, it is imperative to meet the nutritional needs of both the pregnant person and the unborn child. This includes an increase in certain micronutrients, such as iron and folate.
- Common discomforts that can impact nutritional intake during pregnancy include nausea and vomiting, heartburn, and constipation.
- Gestational hypertension is a condition that results in a rise of blood pressure levels and can lead to preeclampsia during a pregnancy.
- Gestational diabetes is a condition that results in a rise of blood glucose levels and can lead to Type 2 diabetes later in life.
References
Chapter cover photo "Maternity shot with toddler" by Philippe Put is licensed under CC BY 2.0.
- Institute of Medicine. Weight gain during pregnancy: reexamining the guidelines . Washington, DC: National Academies Press; 2009.
- Han, Z., Mulla, S., Beyene, J., Liao, G., McDonald, S.D., Knowledge Synthesis Group. Maternal underweight and the risk of preterm birth and low birth weight: a systematic review and meta-analysis. International Journal of Epidemiology; 2011;40(1): 65-101.
- Obesity and Pregnancy. acog.org. www.acog.org/patient-resources/faqs/pregnancy/obesity-and-pregnancy. Accessed July 9, 2020.
- Summary Report of the Dietary Reference Intakes. nationalacademies.org. www.nationalacademies.org/our-work/summary-report-of-the-dietary-reference-intakes. Accessed July 9, 2020.
- Caffeine in pregnancy. marchofdimes.org. https://www.marchofdimes.org/pregnancy/caffeine-in-pregnancy.aspx. Accessed July 9, 2020.
- People at Risk - Pregnant Women and Newborns. cdc.gov. https://www.cdc.gov/listeria/risk-groups/pregnant-women.html. Accessed July 9, 2020.
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd edition. Washington, DC: U.S. Department of Health and Human Services; 2018. https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf. Accessed July 9, 2020.
- World Health Organization. WHO recommendations for prevention and treatment of pre-eclampsia and eclampsia. Geneva, Switzerland: WHO Press; 2011. https://www.who.int/reproductivehealth/publications/maternal_perinatal_health/9789241548335/en/. Accessed July 9, 2020.