
19.4: Anatomy of Lymphatic Organs and Tissues
- Page ID
- 22392

By the end of this section, you will be able to:
- Describe the structure and function of the primary and secondary lymphatic organs
- Describe the structure, function, and location of lymphoid tissues
Lymphoid organs are distinct structures consisting of multiple tissue types. The category can be further subdivided into primary lymphoid organs, which support lymphocyte production and development, and secondary lymphoid organs, which support lymphocyte storage and function. Lymphoid tissues are concentrations of lymphocytes and other immune cells within other organs of the body.
Primary Lymphoid Organs and Lymphocyte Development
The differentiation and development of B and T cells is critical to the adaptive immune response. When the body is exposed to a new pathogen, lymphocytes of the adaptive immune response must "learn" the new antigen associated with the pathogen, mount an effective response to eradicate the pathogen, and "remember" the antigen in case the body is exposed again in the future by forming memory cells. It is also through this process that the body (ideally) learns to destroy only pathogens and leaves the body’s own cells relatively intact. The primary lymphoid organs are the bone marrow and thymus gland. The lymphoid organs are where lymphocytes proliferate and mature.
Bone Marrow
Yellow bone marrow consists of adipose tissue, consisting largely of fat cells for energy storage (Figure \(\PageIndex{1}\)) and is primarily located in the medullary cavity of adult long bones. Red bone marrow is a loose collection of cells where hematopoiesis (blood cell formation) occurs surrounding a framework of reticular connective tissue. Red bone marrow is primarily located surrounding the trabeculae of spongy bone.
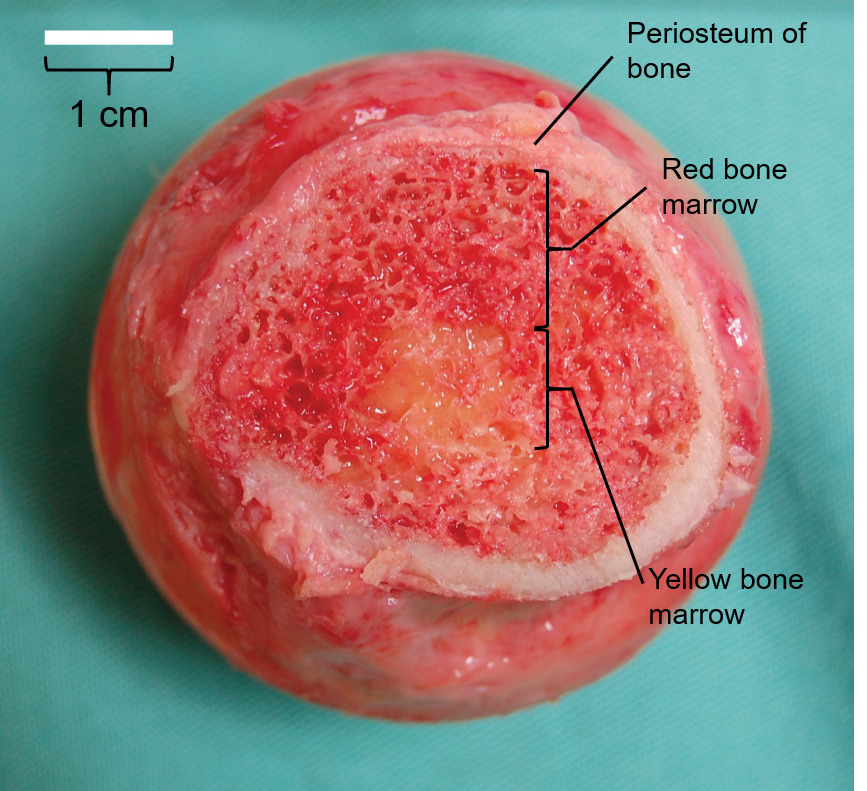 Figure \(\PageIndex{1}\): Bone Marrow. A layer of spongy bone over 1 cm thick with red bone marrow filling the spaces around its trabeculae forms the majority of the head of the femur, covered in periosteum and surrounding a spot of yellow bone marrow at the center slightly less than 1 cm in diameter. (Image credit: "Bone Marrow" by Julie Jenks is licensed under CC BY 4.0 / A derivative from the original work)
Figure \(\PageIndex{1}\): Bone Marrow. A layer of spongy bone over 1 cm thick with red bone marrow filling the spaces around its trabeculae forms the majority of the head of the femur, covered in periosteum and surrounding a spot of yellow bone marrow at the center slightly less than 1 cm in diameter. (Image credit: "Bone Marrow" by Julie Jenks is licensed under CC BY 4.0 / A derivative from the original work)Hematopoiesis is summarized in Figure \(\PageIndex{2}\) and was covered in more detail in the blood chapter. In the embryo, blood cells are made in the yolk sac. As development proceeds, this function is taken over by the spleen, lymph nodes, and liver. Later, the red bone marrow takes over most hematopoietic functions, although the final stages of the differentiation of some cells may take place in other organs. The B cell undergoes nearly all of its development in the red bone marrow, whereas the immature T cell, called a thymocyte, leaves the bone marrow and matures largely in the thymus gland.
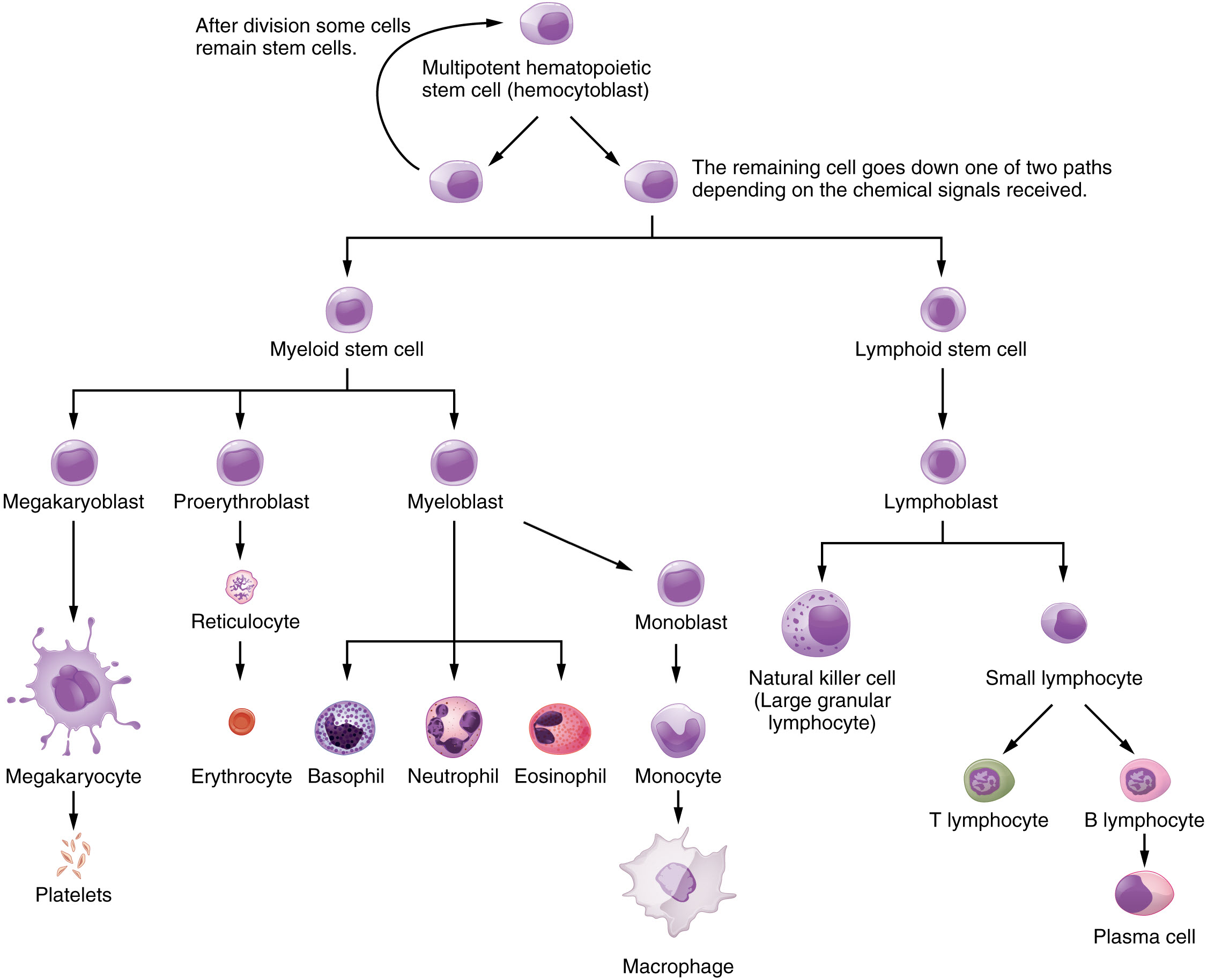 Figure \(\PageIndex{2}\): Hematopoietic System of Bone Marrow. Hematopoiesis is the proliferation and differentiation of the formed elements of blood. (Image credit: "Hematopoietic System of the Bone Marrow" by Julie Jenks is licensed under CC BY 4.0 / A derivative from the original work)
Figure \(\PageIndex{2}\): Hematopoietic System of Bone Marrow. Hematopoiesis is the proliferation and differentiation of the formed elements of blood. (Image credit: "Hematopoietic System of the Bone Marrow" by Julie Jenks is licensed under CC BY 4.0 / A derivative from the original work) Thymus
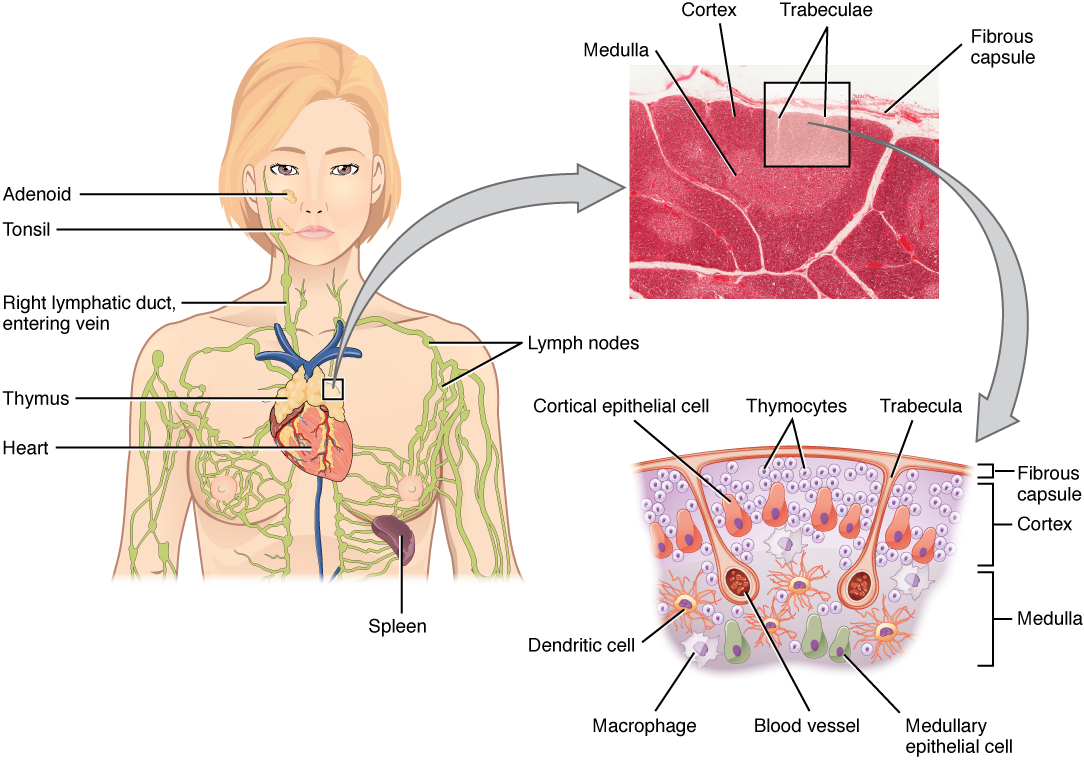
The thymus gland is a bilobed organ found in the space between the sternum and the aorta of the heart (Figure \(\PageIndex{3}\)) that serves as a specialized structure in which T lymphocytes mature. The thymus is most active early in life as you are exposed to and build immunity to many pathogens. After puberty, the thymus slowly but continuously decreases in activity and size as its tissue is replaced with a mix of fibrous and adipose connective tissues.
In the thymus, the maturation of T lymphocytes begins with thymocytes. Thymocytes travel through the bloodstream from the red bone marrow to the thymus. Thymocytes are precursors to T lymphocytes that lack the surface proteins mature T lymphocytes use to recognize an antigen and coordinate an adaptive immune response. There is a multi-step physiological process by which T lymphocytes mature into naïve T lymphocytes ready to be activated for an adaptive immune response.
Dense irregular connective tissue holds the lobes of the thymus closely together but also separates them and forms a fibrous capsule. The fibrous capsule further divides the thymus into lobules via extensions called trabeculae. Blood vessels and nerves are routed within the trabeculae. The outer region of each lobule is known as the cortex and here the structure of the thymus forms a blood-thymus barrier to prevent the thymocytes from being exposed to antigens from the bloodstream before they mature. The densely packed thymocytes in the cortex stain more intensely than the rest of the thymus (see Figure \(\PageIndex{3}\)). The medulla contains a less dense collection of thymocytes, epithelial cells, macrophages, and dendritic cells, so it appears more lightly stained in the micrograph. Thymocytes move from the cortex to the medulla as they mature where the lack of the blood-thymus barrier allows them to enter the bloodstream and travel to other lymphatic structures to await activation for an adaptive immune response.
AGING AND THE...
Immune System
By the year 2050, 25 percent of the population of the United States will be 60 years of age or older. The CDC estimates that 80 percent of those 60 years and older have one or more chronic diseases associated with deficiencies of the immune systems. This loss of immune function with age is called immunosenescence. To treat this growing population, medical professionals must better understand the aging process. One major cause of age-related immune deficiencies is thymic involution, the shrinking of the thymus gland that begins after puberty, at a rate of about three percent tissue loss per year, and continues until 35–45 years of age, when the rate declines to about one percent loss per year for the rest of one’s life. At that pace, the total loss of thymic epithelial tissue and thymocytes would occur at about 120 years of age. Thus, this age is a theoretical limit to a healthy human lifespan.
Thymic involution has been observed in all vertebrate species that have a thymus gland. Animal studies have shown that transplanted thymic grafts between inbred strains of mice involuted according to the age of the donor and not of the recipient, implying the process is genetically programmed. There is evidence that the thymic microenvironment, so vital to the development of naïve T cells, loses thymic epithelial cells according to the decreasing expression of the FOXN1 gene with age.
It is also known that thymic involution can be altered by hormone levels. Sex hormones such as estrogen and testosterone enhance involution, and the hormonal changes in pregnant women cause a temporary thymic involution that reverses itself, when the size of the thymus and its hormone levels return to normal, usually after lactation ceases. What does all this tell us? Can we reverse immunosenescence, or at least slow it down? The potential is there for using thymic transplants from younger donors to keep thymic output of naïve T cells high. Gene therapies that target gene expression are also seen as future possibilities. The more we learn through immunosenescence research, the more opportunities there will be to develop therapies, even though these therapies will likely take decades to develop. The ultimate goal is for everyone to live and be healthy longer, but there may be limits to immortality imposed by our genes and hormones.
DISORDERS OF THE...
Immune System: Autoimmune Responses
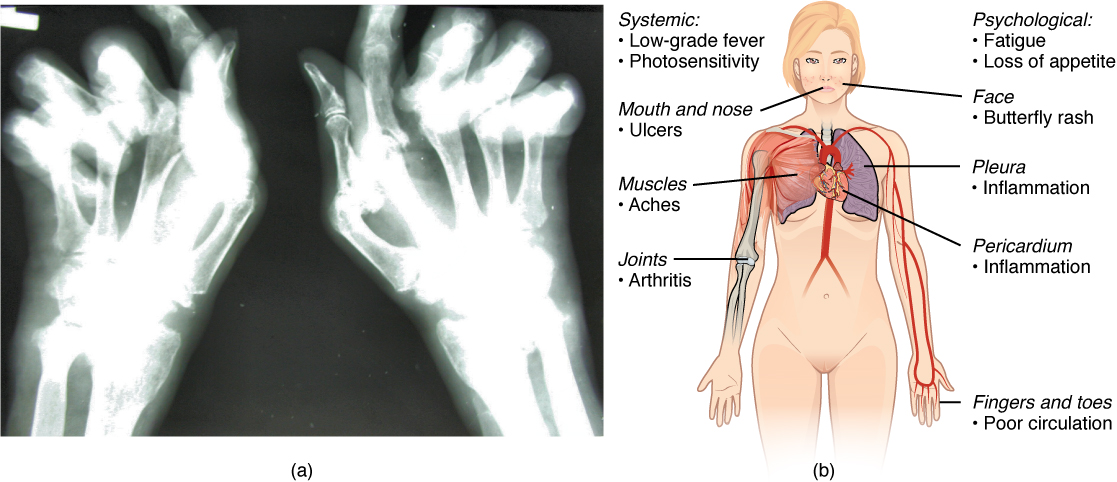
The worst cases of the immune system over-reacting are autoimmune diseases. Somehow, tolerance breaks down and the immune systems in individuals with these diseases begin to attack their own bodies, causing significant damage. The trigger for these diseases is, more often than not, unknown and the treatments are usually based on resolving or minimizing the symptoms using immunosuppressive and anti-inflammatory drugs such as steroids. These diseases can be localized and crippling, as in rheumatoid arthritis, or diffuse in the body with multiple symptoms that differ in different individuals, as is the case with systemic lupus erythematosus (Figure \(\PageIndex{4}\)).
Environmental triggers seem to play large roles in autoimmune responses. One explanation for the breakdown of tolerance is that, after certain bacterial infections, an immune response to a component of the bacterium cross-reacts with a self-antigen. This mechanism is seen in rheumatic fever, a result of infection with Streptococcus bacteria, which causes strep throat. The antibodies to this pathogen’s M protein cross-react with an antigenic component of heart myosin, a major contractile protein of the heart that is critical to its normal function. The antibody binds to these molecules and activates complement proteins, causing damage to the heart, especially to the heart valves. On the other hand, some theories propose that having multiple common infectious diseases actually prevents autoimmune responses. The fact that autoimmune diseases are rare in countries that have a high incidence of infectious diseases supports this idea.
There are genetic factors in autoimmune diseases as well. Overall, there are more than 80 different autoimmune diseases, which are a significant health problem in the elderly. Table \(\PageIndex{1}\) lists several of the most common autoimmune diseases, along with the antigens that are targeted and symptoms of the disease.
| Disease | Autoantigen | Symptoms |
|---|---|---|
| Celiac disease | Tissue transglutaminase | Damage to small intestine |
| Diabetes mellitus type I | Beta cells of pancreas | Low insulin production; inability to regulate serum glucose |
| Graves’ disease | Thyroid-stimulating hormone receptor (antibody blocks receptor) | Hyperthyroidism |
| Hashimoto’s thyroiditis | Thyroid-stimulating hormone receptor (antibody mimics hormone and stimulates receptor) | Hypothyroidism |
| Lupus erythematosus | Nuclear DNA and proteins | Damage to many body systems |
| Myasthenia gravis | Acetylcholine receptor in neuromuscular junctions | Debilitating muscle weakness |
| Rheumatoid arthritis | Joint capsule antigens | Chronic inflammation of joints |
Secondary Lymphoid Organs and their Roles in Immune Responses
Lymphocytes develop and mature in the primary lymphoid organs, but they mount immune responses from the secondary lymphoid organs. A naïve lymphocyte is one that has left the primary organ and entered a secondary lymphoid organ. Naïve lymphocytes are fully functional immunologically, sometimes referred to as immunocompetency, but have yet to encounter an antigen to which to respond. In addition to circulating in the blood and lymph, lymphocytes concentrate in secondary lymphoid organs, which include the lymph nodes, spleen, and lymphoid tissues associated with several organs in the body. All of these tissues have many features in common, including the following:
- An internal structure of reticular connective tissue with associated fixed macrophages
- The presence of lymphoid follicles, collections of lymphocytes, with specific B cell-rich and T cell-rich areas
- Germinal centers, which are the sites of activated (rapidly dividing) B lymphocytes and plasma cells, with the exception of the spleen
- Specialized post-capillary vessels known as high endothelial venules; the cells lining these venules are thicker and more columnar than normal endothelial cells, which allow cells from the blood to directly enter these tissues
Lymph Nodes
As described in the previous section, lymph nodes are positioned at regular intervals along the length of lymphatic vessels. Lymph nodes function to remove debris and pathogens from the lymph, and are thus sometimes referred to as the “filters of the lymph” (Figure \(\PageIndex{5}\)). Any bacteria that infect the interstitial fluid are taken up by the lymphatic capillaries and transported to a regional lymph node. Dendritic cells and macrophages within this organ internalize and kill many of the pathogens and debris that pass through, thereby removing them from the body. The lymph node is the most common site of activation of adaptive immune responses mediated by T cells, B cells, and accessory cells of the adaptive immune system. This is why swollen lymph nodes can be a sign of infection.
Like the thymus, the bean-shaped lymph nodes are surrounded by a tough capsule of dense connective tissue and are separated into compartments by trabeculae, extensions of the capsule. In addition to the structure provided by the capsule and trabeculae, the structural support of the lymph node is provided by a series of reticular fibers laid down by fibroblasts of its reticular connective tissue framework. Several afferent lymphatic vessels deliver lymph into the convex side of a lymph node and a one-way valve in each vessel near where it connects with the lymph node prevents back-flow of lymph. One or two efferent lymphatic vessels allow lymph to flow out of the concave hilum of the lymph node. The tissue inside the lymph node consists of two generalized regions: the cortex and the medulla. The cortex is nearest the convex side of the node and contains lymphoid follicles where activated lymphocytes proliferate. The medulla, nearest the hilum of each node, is rich with lymphocytes (T cells, B cells, and plasma cells), as well as macrophages and dendritic cells.
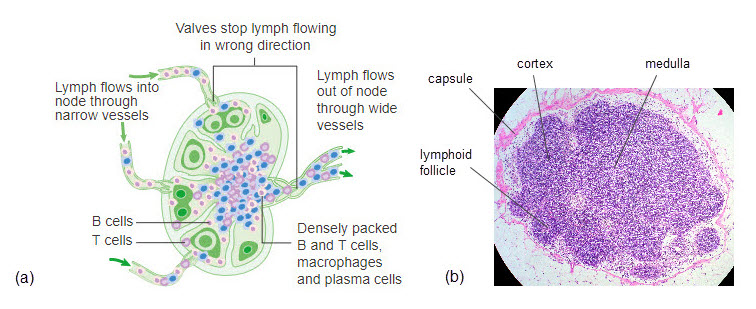 Figure \(\PageIndex{5}\): Lymph Node. (a) Lymph flows into a lymph node via afferent vessels through the open cusps of one-way valves that prevent lymph from flowing in the wrong direction. Within the lymph node, lymph flows past densely packed immune cells that remove debris and pathogens (including B and T cells, macrophages, and plasma cells), and then out of the node through more back-flow preventing one-way valves into efferent vessels. (b) Histological view of lymph node cross-section showing capsule surrounding several visible lymphoid follicles in the cortex surrounding the medulla that is densely packed with dark-staining cells. (Image credit: "Lymph Node" by Julie Jenks is licensed under CC BY 4.0 / a derivative from the original work in (a) and the original work in (b))
Figure \(\PageIndex{5}\): Lymph Node. (a) Lymph flows into a lymph node via afferent vessels through the open cusps of one-way valves that prevent lymph from flowing in the wrong direction. Within the lymph node, lymph flows past densely packed immune cells that remove debris and pathogens (including B and T cells, macrophages, and plasma cells), and then out of the node through more back-flow preventing one-way valves into efferent vessels. (b) Histological view of lymph node cross-section showing capsule surrounding several visible lymphoid follicles in the cortex surrounding the medulla that is densely packed with dark-staining cells. (Image credit: "Lymph Node" by Julie Jenks is licensed under CC BY 4.0 / a derivative from the original work in (a) and the original work in (b))Spleen
The spleen is located inferior and medial to the curve of the diaphragm and lateral to the stomach in the upper left quadrant of the abdomen. It is built on a framework of reticular connective tissue and surrounded by a capsule of dense irregular connective tissue that invaginates into trabeculae to divide the spleen into nodules (Figure \(\PageIndex{6}\)). Upon entering the spleen, the splenic artery splits into several arterioles and eventually into sinusoid capillaries. Blood from the capillaries subsequently collects in venules that drain into the splenic vein.
Within each splenic nodule is a large area of red pulp surrounding the sinusoid capillaries that is so-called because it consists mainly of erythrocytes. The red pulp consists of reticular fibers with fixed macrophages attached, free macrophages, and other formed elements of the blood, including some lymphocytes. The red pulp primarily functions in phagocytosis of worn-out erythrocytes and bloodbourne pathogens. Aside from the blood vessels, the remaining tissue of each nodule is called the white pulp, so-called because it lacks the erythrocytes found in the red pulp. The white pulp surrounds the arteriole and resembles the lymphoid follicles of the lymph nodes. It consists of germinal centers of dividing B cells surrounded by T cells and accessory cells, including macrophages and dendritic cells. Germinal centers function as a site of T cell and B cell activation. The marginal zone is the region where the white pulp transitions to the red pulp and their functions mix.
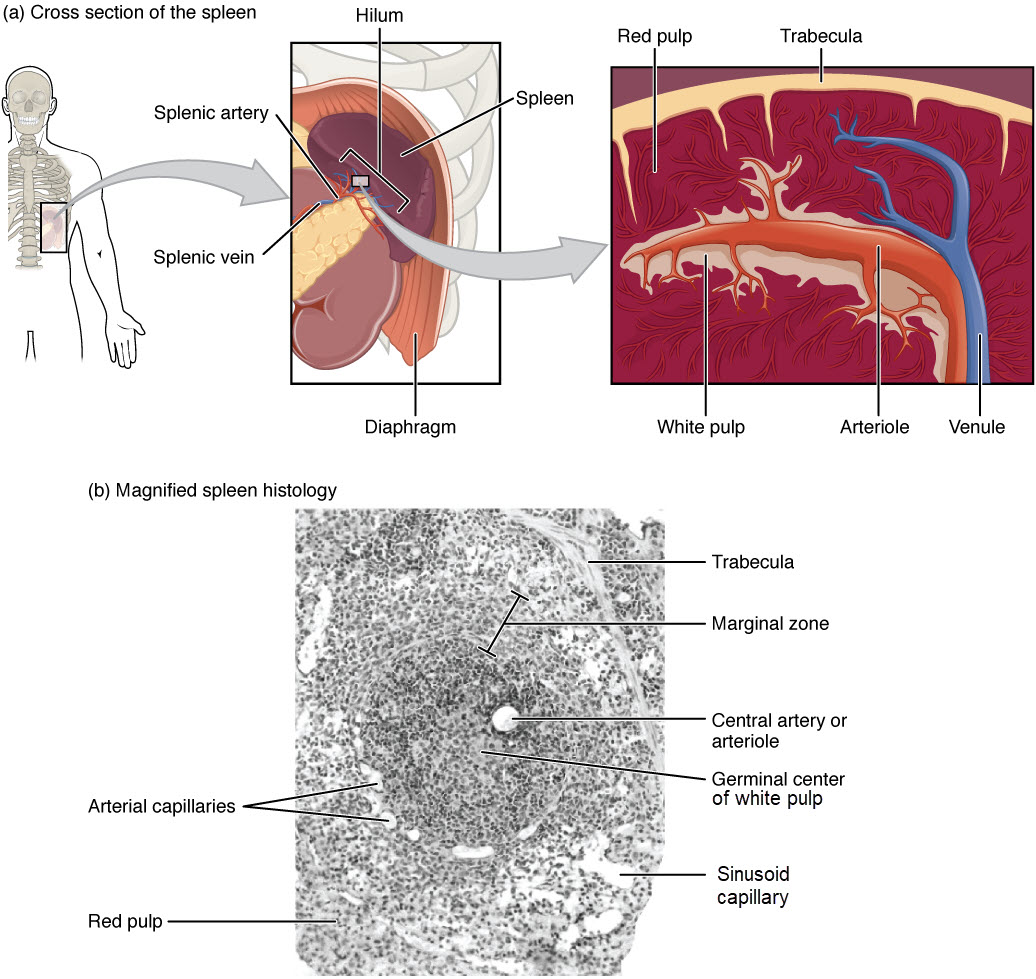 Figure \(\PageIndex{6}\): Location, Structure, and Histology of the Spleen. (a) The spleen is lateral to the stomach and pancreas. A cross-section reveals trabeculae that divide the spleen into nodules consisting of an arteriole surrounded by white pulp and feeding sinusoid capillaries surrounded by red pulp that drain to a venule (b) A micrograph of spleen tissue shows the red pulp and white pulp separated by a marginal zone. The white pulp contains germinal centers and is centrally located in the nodule surrounding the arteriole and arterial capillaries. EM × 660. (Image credit: "Spleen" by Julie Jenks is licensed under CC BY 4.0 / A derivative from the original work / Micrograph provided by the Regents of the University of Michigan Medical School © 2012)
Figure \(\PageIndex{6}\): Location, Structure, and Histology of the Spleen. (a) The spleen is lateral to the stomach and pancreas. A cross-section reveals trabeculae that divide the spleen into nodules consisting of an arteriole surrounded by white pulp and feeding sinusoid capillaries surrounded by red pulp that drain to a venule (b) A micrograph of spleen tissue shows the red pulp and white pulp separated by a marginal zone. The white pulp contains germinal centers and is centrally located in the nodule surrounding the arteriole and arterial capillaries. EM × 660. (Image credit: "Spleen" by Julie Jenks is licensed under CC BY 4.0 / A derivative from the original work / Micrograph provided by the Regents of the University of Michigan Medical School © 2012)Lymphoid Nodules
The other lymphoid tissues, lymphoid nodules, have a simpler architecture than the spleen and lymph nodes in that they consist of a dense cluster of lymphocytes on a framework of reticular connective tissue without a surrounding fibrous capsule. These nodules are associated with the mucus membranes of the respiratory and digestive tracts, areas routinely exposed to environmental pathogens.
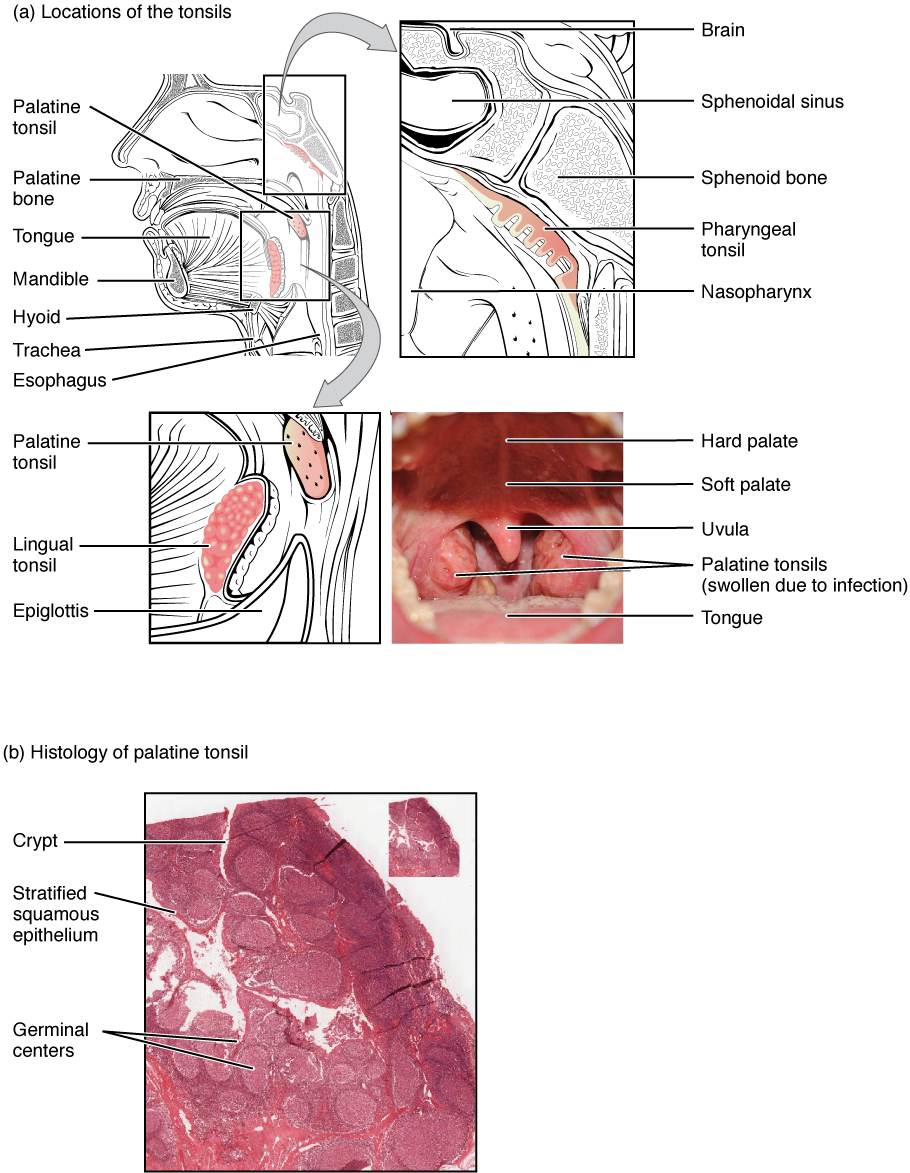
Tonsils are lymphoid nodules located along the inner surface of the pharynx and are important in developing immunity to oral pathogens (Figure \(\PageIndex{7}\)).
- The pharyngeal tonsil, sometimes referred to as the adenoid, is located in the superoposterior of the nasopharynx
- The palatine tonsils are in the lateral wall of the oropharynx
- The lingual tonsil faces the oropharynx in the wall at the posterior of the tongue
Swelling of the tonsils is an indication of an active immune response to infection. Histologically, tonsils do not contain a complete capsule, and the epithelial layer invaginates deeply into the interior of the tonsil to form tonsillar crypts. The crypts allow all sorts of materials taken into the body through eating and breathing to accumulate in the tonsils, actually “encouraging” pathogens to penetrate deep into the tonsillar tissues where T cells and B cells in the germinal centers can be activated for an adaptive immune response. This seems to be the major function of tonsils—to help children’s bodies recognize, destroy, and develop immunity to common environmental pathogens so that they will be protected in their later lives. Tonsils are often removed in those children who have recurring throat infections, especially those involving the palatine tonsils on either side of the throat, whose swelling may interfere with their breathing and/or swallowing.
Mucosa-associated lymphoid tissue (MALT) consists of an aggregate of lymphoid follicles directly associated with the mucous membrane epithelia. MALT makes up dome-shaped structures found underlying the mucosa of the gastrointestinal tract, breast tissue, lungs, and eyes. Peyer’s patches, a type of MALT in the small intestine, are especially important for immune responses against ingested substances (Figure \(\PageIndex{8}\)). Peyer’s patches contain specialized endothelial cells called M (or microfold) cells that sample material from the intestinal lumen and transport it to nearby follicles so that adaptive immune responses to potential pathogens can be mounted.
_Nodule.jpg?revision=1&size=bestfit&width=600&height=408)
Concept Review
Lymphoid organs are comprised of multiple tissues forming a distinct structure in the body. Primary lymphoid organs include bone marrow and the thymus. Lymphocytes and other blood cells are produced in red bone marrow while lipids are stored for long-term energy in yellow bone marrow. B lymphocytes remain in red bone marrow to develop into naïve B lymphocytes. The thymus is the organ in which immature T lymphocytes are stored and develop into naïve T lymphocytes. Naïve T and B lymphocytes travel to secondary lymphoid organs, lymph nodes and the spleen, from where they can be activated for the adaptive immune response. Lymph nodes filter lymph for invaders, abnormal cells, and debris as it drains to the bloodstream through lymphatic vessels. The spleen, in the white pulp, filters the blood for invaders, abnormal cells, and debris as it circulates through the bloodstream. The red pulp of the spleen also filters the blood and serves to remove worn-out red blood cells from circulation. Concentrations of lymphocytes and other immune cells within mucus membranes of other organ systems are called lymphoid tissues or nodules. The tonsils surround the pharynx while mucosa-associated lymphoid tissue (MALT) are found in mucus membranes of the gastrointestinal tract, breast tissue, lungs, and eyes.
Review Questions
Q. Which of the lymphoid nodules is most likely to see food-bourne antigens first?
A. tonsils
B. Peyer’s patches
C. bronchus-associated lymphoid tissue
D. mucosa-associated lymphoid tissue
- Answer
-
Answer: A
Critical Thinking Questions
Q. Compare and contrast functions of the lymph nodes and the spleen.
- Answer
-
A. Both lymph nodes and the spleen filter transport fluids in the body for pathogens, abnormal cells, and debris. Lymph nodes are positioned at intervals along lymphatic vessels to filter lymph as it travels through the lymphatic vessels. The spleen filters blood as it travels through the blood stream. Both lymph nodes and the spleen are secondary lymphoid organs meaning they contain concentrations of naïve lymphocytes and other immune cells from which an adaptive immune response can be mounted.
Glossary
- afferent lymphatic vessels
- lead into a lymph node
- bone marrow
- tissue found inside bones; the site of all blood cell differentiation and maturation of B lymphocytes
- efferent lymphatic vessels
- lead out of a lymph node
- germinal centers
- clusters of rapidly proliferating B cells found in secondary lymphoid tissues
- high endothelial venules
- vessels containing unique endothelial cells specialized to allow migration of lymphocytes from the blood to the lymph node
- lingual tonsil
- lymphoid nodule in the anterior wall of the oropharynx posterior to the tongue
- lymph node
- one of the bean-shaped organs found associated with the lymphatic vessels
- lymphoid nodules
- unencapsulated patches of lymphoid tissue found throughout the body
- mucosa-associated lymphoid tissue (MALT)
- lymphoid nodule associated with the mucosa
- palatine tonsils
- lymphoid nodules in the right and left lateral walls of the oropharynx
- pharyngeal tonsil (adenoid)
- lymphoid nodule in the superoposterior wall of the nasopharynx
- primary lymphoid organ
- site where lymphocytes mature and proliferate; red bone marrow and thymus gland
- red pulp
- region of a spleen nodule that is so-called because it is filled with many erythrocytes that surrounds the sinusoid capillaries and functions primarily to remove worn-out erythrocytes from circulation
- secondary lymphoid organs
- sites where lymphocytes mount adaptive immune responses; examples include lymph nodes and spleen
- spleen
- secondary lymphoid organ that filters pathogens from the blood (white pulp) and removes degenerating or damaged blood cells (red pulp)
- thymocyte
- immature T cell found in the thymus
- thymus
- primary lymphoid organ; where T lymphocytes proliferate and mature
- tonsils
- lymphoid nodules associated with the pharynx
- white pulp
- region of a spleen nodule that is filled with germinal centers surrounding the arteriole that functions to activate B cells and T cells
Contributors and Attributions
OpenStax Anatomy & Physiology (CC BY 4.0). Access for free at https://openstax.org/books/anatomy-and-physiology