
3.13: Surgical Correction of Choanal Atresia
- Page ID
- 47878

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
CHOANAL ATRESIA SURGERY
Neil Tan, Nico Jonas

Figure 1: Axial CT demonstrating bilateral choanal atresia with left-sided mixed bony / membranous atresia and right-sided bony atresia
Choanal atresia is defined as a blockage of the posterior nasal openings. It is a rare condition and has an incidence of 1/7000 live births. It can be unilateral or bilateral. The blockage is purely bony in 30% of cases; in the remaining 70% it is a mixed bony and membranous obstruction (Figure 1). Complete total bony obstruction is extremely rare.
It is believed that membranous obstruction occurs due to failure of the bucconasal membrane to rupture sometime between the 5th and 6th weeks of foetal development. Bony obstruction occurs due to a combination of
- A narrow nasal cavity
- Medial thickening of the medial pterygoid plate
- Lateral thickening of the vomer

Figure 2: Axial CT scan demonstrating unilateral left-sided choanal atresia

Figure 3: Retropalatal 700 endoscopic view demonstrating unilateral choanal atresia

Figure 4: Retropalatal endoscopic view demonstrating bilateral choanal atresia
Unilateral choanal atresia (Figures 2, 3) is most commonly an isolated problem. However 75% of bilateral cases (Figure 4) have associated syndromic or congenital abnormalities. These include CHARGE syndrome (coloboma, heart defects, choanal atresia, retardation of growth, genital abnormalities and ear abnormalities) and other syndromes that have associated craniofacial abnormalities such as Treacher Collins, Crouzon syndrome, velocardiofacial syndrome or craniosynostosis.
Differential diagnosis
The differential diagnosis of choanal atresia includes
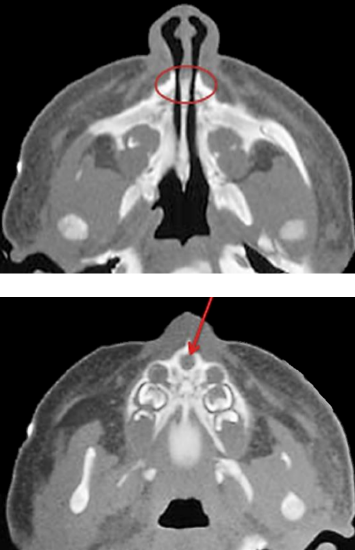
Figure 5: Axial CT scan in a patient with pyriform aperture stenosis and with a single central incisor (Red arrow)
- Nasal pyriform aperture stenosis (Figure 5)
- Deviated nasal septum
- Dislocated nasal septum
- Septal hematoma
- Neonatal rhinitis
- Mucosal swelling
- Turbinate hypertrophy
- Encephalocoele
- Nasal glioma
- Intranasal dermoid
- Chordoma
- Teratoma
Presentation
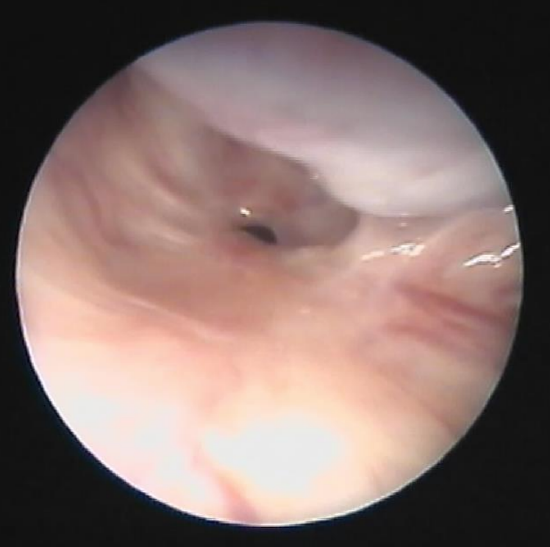
Figure 6: Previously undiagnosed membranous choanal stenosis in an adult
Unilateral choanal atresia may not present until later in life with complaints of a unilateral blocked nose or profuse unilateral nasal discharge (Figure 6).
On the contrary, bilateral choanal atresia presents as an acute emergency at birth as respiratory distress because newborns are obligate nasal breathers. A common feature of bilateral atresia is cyclical cyanosis whereby a newborn has respiratory distress with cyanotic episodes that improve on crying, and worsen on feeding.
Clinical evaluation
1. Two simple tests can be used to demonstrate airflow through the nose to exclude choanal atresia
- Movement of a thin piece of cotton wool held directly underneath the nares during inspiration and expiration
- A shiny metal tongue depressor held under the nares will reveal nasal misting in patients with patent nasal airways
2. Failure to pass an 8F (or smaller) suction catheter into the nasal cavity more than 5.5 cm from the alar rim can suggest the diagnosis

Figure 7: Transnasal endoscopic view of previously undiagnosed (R) unilateral choanal atresia in an adult (S = Septum; IT = inferior turbinate)
3. Direct visualization with a flexible nasendoscope after nasal suctioning will definitively diagnose the condition (Figure 7)
Radiological evaluation

Figure 8: Lateral X-ray after filling the nose with radio-opaque dye demonstrates hold-up in the posterior nasal cavity (yellow arrows). Note oropharyngeal airway to maintain the airway
The diagnosis can be confirmed with a lateral skull X-ray after filling the nose with radiopaque dye and demonstrating hold-up of the dye in the posterior nasal cavity (Figure 8).
The atresia can be subclassified by CT scanning into bony or mixed bony membranous types (Figure 1). It is important to apply nasal decongestant (0.5% xylometazaline) 30 minutes prior to the CT scan and to suction the nose immediately before the CT scan to remove all nasal secretions in order to enable accurate radiological diagnosis.
Immediate Emergency Management

Figure 9: Oral airway secured with tape
An oral airway is generally adequate to temporarily secure an airway in a newborn with bilateral choanal atresia and respiratory distress (Figure 9).

Figure 10: Standard dummy with the tip cut off

Figure 11: Guedel oropharyngeal airway
A McGovern nipple or a standard feeding bottle teat or dummy with the tip cut off (Figure 10) can also be used to facilitate oral breathing. In the short-term this has the effect of stenting the oral cavity open to allow mouth breathing; however it is not a long-term solution. Alternative options include a Guedel oropharyngeal airway (Figure 11). If an oral airway is not effective one has to proceed to endotracheal intubation.
Feeding should be established via orogastric tube until surgical correction of the atresia is performed.
The patient should ideally be managed in a neonatal or pediatric intensive care unit with involvement of neonatologists, geneticists, pediatric ENT surgery and other specialties as required.
Timing of surgery
Surgery is urgently required for bilateral disease and symptomatic unilateral disease. Definitive surgery can often be delayed in patients with asymptomatic unilateral atresia. However, syndromic babies can have respiratory complications from unilateral atresia that require earlier surgery.
Preoperative Workup
All patients should undergo a full workup and evaluation once the airway has been secured, including for possible syndromic associations. The minimum investigations beyond the initial CT scan include ultrasonography of the cardiac and renal systems as well as ophthalmological and audiological assessment.
Genetic testing may be useful for patients with features of CHARGE syndrome; 67% are due to a recognized mutation in the chromodomain helicase DNA-binding protein-7 (CHD7) gene. The remainder are related to mutations in unrelated genes or other cytogenetic anomalies such as chromosome deletions.
Surgical management

Figure 12: CT demonstrates need to thin the thickened vomer (red arrow) and widen the medialized medial pterygoid plate (yellow arrow)
The key to a successful outcome, regardless of surgical approach, is to create a large, 3-dimensional opening by a combination of (Figure 12)
- Puncturing the membranous obstruction
- Widening the medial bony thickening of the medial pterygoid plate
- Thinning the thickened vomer
Traditionally the atresia was approached by transnasal / retropalatal, transseptal or transpalatal routes, but the last two are rarely used today. Transnasal punctures alone have high rates of restenosis.
Multiple procedures are often required to achieve a permanent opening in the posterior nares.
Retropalatal endoscopic approach
This endoscopic technique is currently favored by most pediatric otolaryngologists. The benefit of the retropalatal approach is that the newborn’s nasal cavity is usually too small to accommodate both a 0° endoscope and a drill.
Transnasal instrumentation

Figure 13: 120 degree rigid endoscope
Visualization is achieved with a retropalatal 120° Hopkins rod (Figure 13).


Figures 14a, b: Urethral sounds used for initial perforation of the atresia

Figure 15: Powered drill (Choanal atresia bur)
Additional equipment includes curved urethral sounds and powered drills (Figures 14, 15).
Surgical steps

Figure 16: Rae tube
- Surgery is done under general anesthesia with a downwards-facing Rae tube
- Tape the Rae tube to the lower lip in the midline as for a tonsillectomy
- Lay the patient supine with a shoulder roll in place
- Decongest the nose using 0.5% xylometazalone

Figure 17: Cleft palate / tonsil gag
- A cleft palate / tonsil gag is used to open the mouth and placed in suspension (Figure 17)
- Retract the soft palate
- With unilateral atresia, insert a nasogastric tube on the unaffected side and pull it out of the mouth
- With bilateral choanal atresia, place a suture in the soft palate to retract the palate until such time as a nasogastric tube can be inserted
- Insert the 120 degree rigid endoscope through the mouth and inspect the nasopharynx and the choanal atresia

Figure 18: Transnasal puncture of membranous atresia with a urethral sound
- Insert a urethral sound into the nose and puncture the atretic plate under direct view with the 120 degree scope (Figure 18)
- The urethral sound may pass easily in a membranous obstruction or less easily in a purely bony atresia

Figure 19: Junction of vomer and palate
- The most common position of the membranous section of an atresia is in the inferomedial corner at the junction of the vomer and the palate (Figure 19)
- Puncturing the atresia is however not sufficient to relieve the obstruction in the long-term, as rapid restenosis will occur without additional bone removal
- Insert the powered drill transnasally with a 4 mm choanal diamond burr

Figure 20: Bilaterally opened choanal atresias after laterally drilling the medial pterygoid plates; vomer intact
- Drill the medial pterygoid plate under direct vision taking care preserve as much mucosa as possible (Figure 20)
- If the vomer impinges on the choana, it can be resected
- If necessary a common posterior choanal opening can be created by removing the posterior few millimeters of the vomer
- Once again as much mucosa as possible is preserved in an attempt to leave as little exposed bone as possible at the end of the procedure
- Obtain hemostasis by using neurosurgical patties soaked in 1:10,000 adrenaline
To stent?

Figure 21: Retropalatal view of bilateral stents in position in the posterior choanae
Stents may be fashioned from cut endotracheal tubes, suction catheters, or custom made silicone stents can be used (Figure 21).
Traditionally almost all patients were stented. Currently stenting is however controversial as stents can cause granulations and scarring.
Stents are still preferred in very small babies that are surgically challenging. In such cases stenting preserves patency for the duration of the stent’s placement and allows for weight gain to occur prior to revision surgery.
Mitomycin C
This is another contentious area with some evidence both for and against its use. It is believed to act topically to reduce mucosal restenosis by decreasing fibroblast mediated scarring.
Postoperative considerations
- After successful choanal atresia surgery the child should be extubated and can usually be managed on a general pediatric ward with regular nasal suctioning
- Oral feeding is established as soon as possible
- Postoperative nasal decongestant drops (0.5% xylometazalone) should be used for one week
- Saline and steroid drops should be used for 2 weeks to reduce postoperative inflammation and granulations
Alternative techniques
Transnasal drill-out with operating microscope
If the equipment required to perform a retropalatal endoscopic approach is not available, a standard operating microscope and a small bur can be used transnasally to open the stenosis. A standard ear speculum can be inserted in the nose after adequate decongestion and will allow for a view of the choanae with the use of a microscope.
Non-powered dilation techniques
If the above equipment is not available, transnasal opening and dilatation of the choanal atresia remains a viable and useful surgical option.
The safest way to achieve this is to use curved urethral sounds to perform an initial puncture of the membranous atresia followed by serial dilatation (Figures 14, 18).
- The surgical setup is identical, with the patient positioned supine with a shoulder roll in position, under general anesthetic with a down-facing Rae endotracheal tube
- Insert a cleft palate/tonsillectomy gag
- Retract the palate using the methods previously described
- A dental mirror and headlight can be used to obtain a view of the posterior choana in order to directly visualize the stenosis
- Prepare the nose with a decongestant
- Insert the smallest urethral sound with the curve pointing towards the floor of the nose and hug the septum to try and puncture the infero-medial corner of the choanal atresia (Figure 18). This avoids potential injury of the skull base during this “blind” procedure
- A finger can be placed on the soft palate or in the postnasal space to monitor when the atresia is punctured
- The opening can be further dilated by using serial urethral sounds until an adequate-sized stent (3.5 ET tube) can be passed


Figures 22a, b: Back-biting forceps used to remove bone from posterior septum
- Back-biting forceps introduced down the nose can be used to remove the posterior septum if necessary (Figure 22)
Author
Neil Tan FRCS, PhD
Pediatric ENT Registrar
Addenbrookes Hospital
Cambridge, United Kingdom
neil.tan@gmail.com
Author and Pediatric Section Editor
Nico Jonas MBChB, FCORL, MMed
Pediatric Otolaryngologist
Addenbrooke’s Hospital
Cambridge, United Kingdom
nicojonas@gmail.com
Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za