
5.5: Temporalis Muscle Flap
- Page ID
- 15458

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
THE TEMPORALIS MUSCLE FLAP
Johan Fagan
The temporalis muscle flap comprises the temporalis muscle, with or without the overlying temporalis fascia. It is an axial flap based on the anterior and posterior deep temporal arteries.
The temporoparietal fascial flap, on the other hand, is also an axial flap but is based on the superficial temporal vessels (Moore EJ. Temporoparietal Fascia Flap. Emedicine).
Relevant anatomy
Superficial temporalis fascia
Deep to the skin and subcutaneous tissues is the superficial temporal fascia, also known as the temporoparietal fascia. At the superior temporal line, this fascial layer continues superiorly as the epicranium, also known as the galea aponeurotica. It continues inferiorly at the level of the zygoma as the SMAS, or superficial musculoaponeurotic system.
Deep temporalis fascia
This layer of fascia is an inferior extension of the pericranium. From the superior temporal line, it overlies the temporalis muscle. Below the superior margin of the orbit, it separates into superficial and deep layers of deep temporalis fascia to attach inferiorly to the lateral and medial margins of the zygomatic arch respectively, with the superficial temporal fat interposed between the two layers.
Temporalis muscle
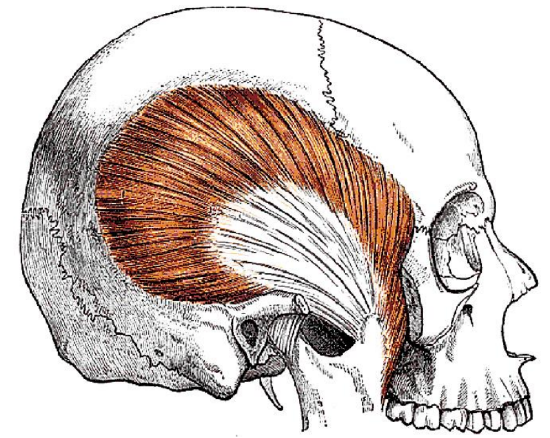
Figure 1: Temporalis muscle
The muscle is fan-shaped, and arises from the lateral surface of the cranium. It fills the temporal fossa and is covered laterally by the deep temporalis fascia. It passes medial to the zygomatic arch to insert onto the coronoid process and the anterior border of the ascending ramus of the mandible (Figure 1).
Innervation
The muscle is innervated by the deep temporal nerves that arise from the mandibular division of trigeminal nerve.
Blood supply (Figure 2)
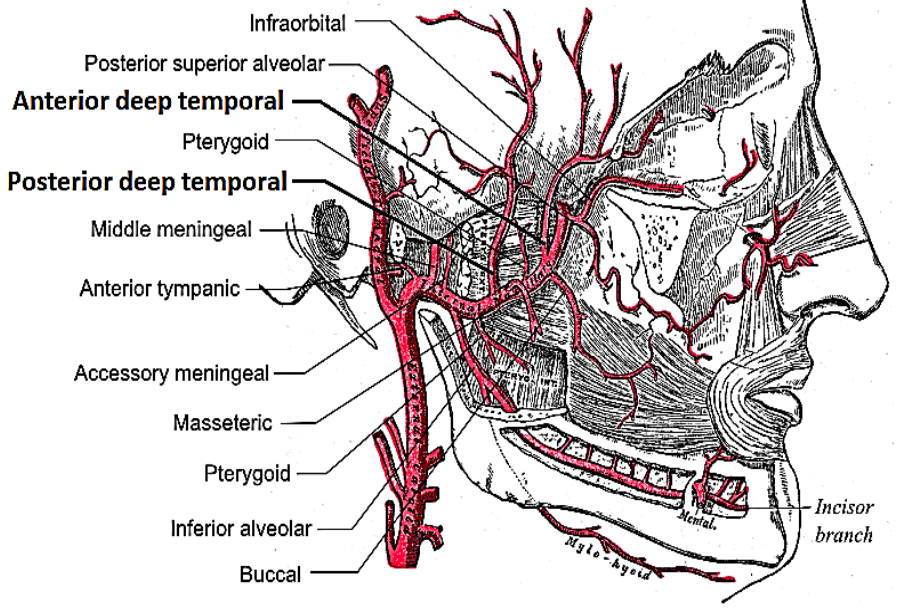
Figure 2: Blood supply
The muscle is supplied by the anterior and posterior deep temporal arteries which are branches of the internal maxillary artery. The arteries are situated on the medial (deep) aspect of the muscle and are medial to the coronoid process. Care therefore has to be taken not to injure the vessels during maxillectomy or oropharyngeal resection. These vessels anastomose within the muscle with the middle temporal artery which is a branch of the superficial temporal artery.
Facial nerve (Figure 3)
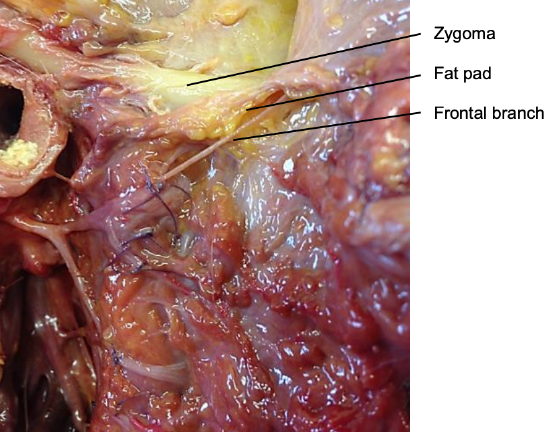
Figure 3: Frontal branch of facial nerve crossing zygoma at fat pad
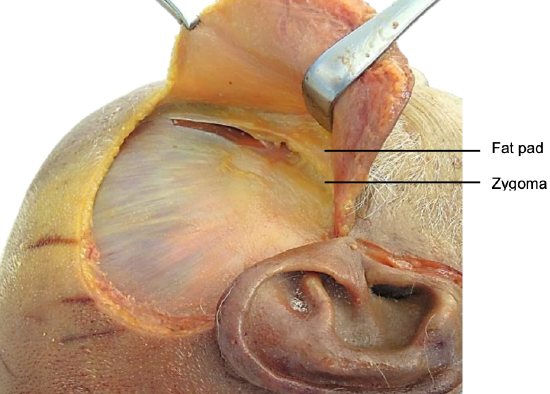
Figure 4: Hemicoronal incision, exposed temporalis fascia and fat pad
Frontal/temporal branches of the nerve cross the zygomatic arch, and run across the superficial temporal fat pad which is deep to the orbicularis oculi muscle just lateral to the orbital rim (Figures 3, 4).
Raising the flap
The flap is accessed via a hemicoronal skin incision commencing in a preauricular skin crease just below the level of the zygoma and placed behind the hairline for cosmetic reasons (Figure 4). The incision is extended to the temporalis fascia. The skin and subcutaneous tissue are elevated in the plane situated on the temporalis fascia (Figure 4). Anteriorly, elevation in this plane is stopped when the superficial temporal fat pad with the facial/temporal branches of the facial nerve is encountered.
At this point the deep layer of deep temporalis fascia is incised in a vertical direction, and the underlying temporalis muscle is exposed (Figure 4).
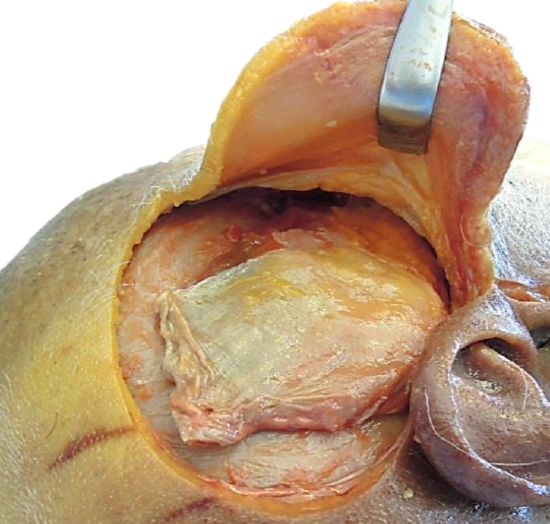
Figure 5: Mobilization of temporalis muscle and exposure of zygomatic arch
Anteriorly, further dissection is done in a subfascial plane, deep to the fat pad, up to the lateral orbital bony rim (anterior margin of temporal fossa). The temporalis fascia is now incised along the superior temporal line and the posterior margins of the muscle, down onto the bone (Figure 5).
If an extended flap is planned, then the superficial temporal vessels are identified and preserved in the preauricular area.
The superior aspect of the zygomatic arch is identified along its full length. This might require quite forceful retraction of the soft tissues with a Langenbeck retractor. The two layers of deep temporal fascia are incised along the superior margin of the zygoma.
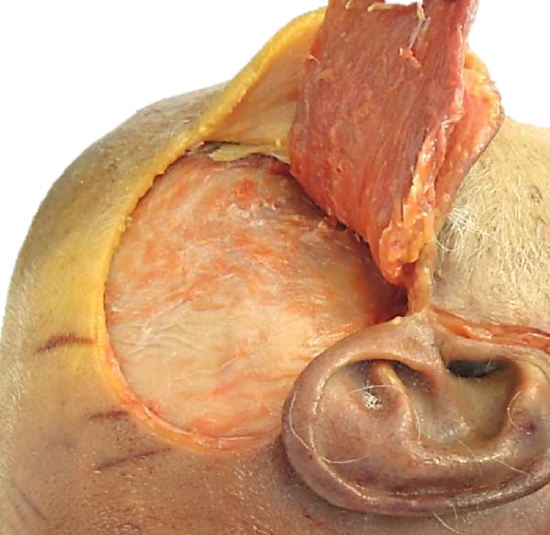
Figure 6: Flap completely elevated from temporal fossa
The temporalis muscle is elevated from the bone of the temporal fossa using either diathermy or a periosteal elevator. The dissection remains hard on the bone and extends medial to the coronoid process of the mandible that is now readily palpable medial to the zygoma, especially when the mouth is closed (Figure 6).
Should the flap need to be passed into the oral cavity, then a finger can now been tunneled into the mouth medial to the muscle and its origin from the coronoid process. With a thin muscle the flap can now be passed through this tunnel into the mouth, taking care not to rotate the flap and strangulate its blood supply. With a bulky muscle, the zygomatic arch and/or the coronoid process of the mandible may be osteotomized to permit passage of the flap. The zygomatic bone can be kept in saline and plated/wired back later in the procedure. The coronoid osteotomy is done either from above via the temporal fossa, or via the mouth. Great care has to be taken not to injure the deep temporal vessels by staying close to the bony surface of the coronoid.
Additional length of flap may be obtained by transecting or resecting the coronoid process and thus freeing the origin of the muscle from the bone, or by using an extended myofascial flap that includes additional temporalis fascia.
Clinical Applications
The temporalis muscle flap may be used for reconstruction of defects of the oral cavity (floor of mouth, tongue, buccal, retromolar trigone, palate), oropharynx, nasopharynx, orbit, maxilla and facial soft tissues.
Palatal and maxillary resections
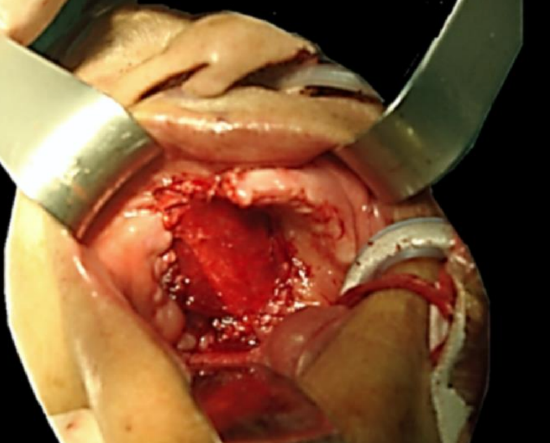
Figure 7: Reconstruction of inferior maxillectomy defect
The flap is ideally suited for reconstruction of the palate following Le Fort 1 maxillectomy (Figure 7), but also following total maxillectomy. The coronoid process of the mandible on which it is pedicled is immediately adjacent to the defect. It may reach across the midline. The muscle is left bare in the mouth, and mucosalises within a matter of weeks. Bilateral palatal resection defects may be reconstructed with bilateral temporalis muscle flaps that are sutured together in the midline.

Figure 8: Mucosalized muscle following palatal reconstruction
Note in Figure 8 how the muscle has become covered with mucosa in a patient with bilateral temporalis muscle flaps for bilateral inferior maxillectomy.
Orbital exenteration

Figure 9: Temporalis muscle filling the orbit

Figure 10: Outcome of primary closure of skin over temporalis muscle flap
The lateral wall of the orbit is removed to provide space for passage of the muscle pedicle. The orbit is filled with the temporalis muscle flap (Figure 9), and is covered with skin or split skin graft, or closed primarily if a lid has been spared (Figure 10).
Drawbacks of temporalis muscle flap
Temporal fossa concavity (Figure 11)

Figure 11: Temporal fossa concavity
The concavity of the temporal fossa from which the muscle has been mobilized can be quite pronounced. It may be filled with a fat graft or hydroxyapatite or molded prosthetic implants.
Dental rehabilitation
Due to the absence of alveolar bone, it is not possible to insert dental implants following inferior maxillectomy reconstruction. With bilateral inferior maxillectomy, it is not possible to fit and retain an upper denture.
Another clinical example (Courtesy Dr Zenon Yeung, Hong Kong)
This patient underwent left inferior maxillectomy via Weber-Ferguson approach. The defect was repaired with a temporalis muscle flap.
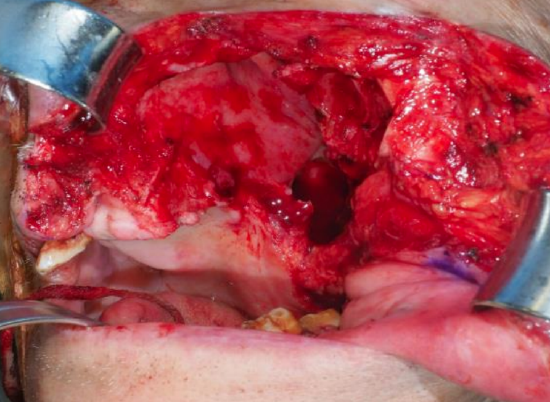
Figure 12: (L) inferior maxillectomy defect

Figure 13: Temporalis muscle flap elevation
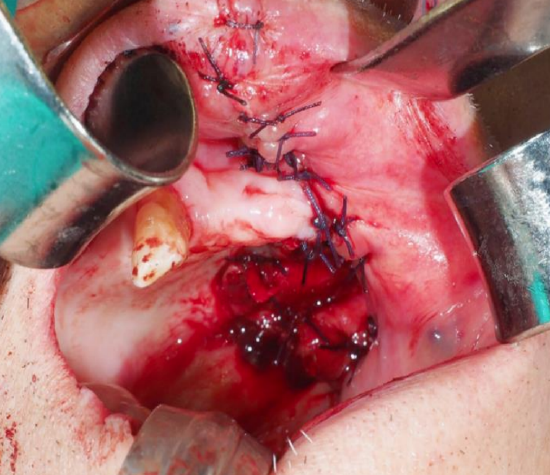
Figure 14: Temporalis muscle flap inset into inferior maxillectomy defect
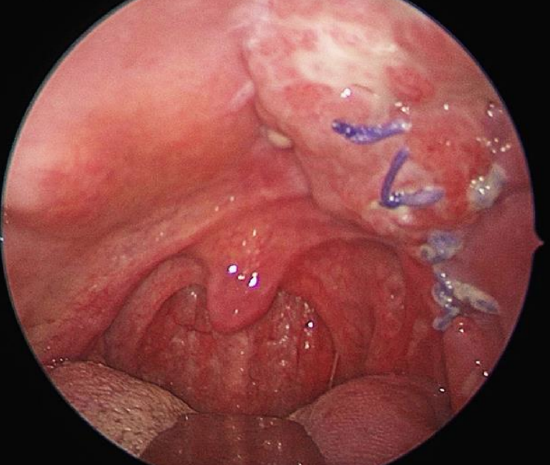
Figure 15: Oral view of flap at 17 days
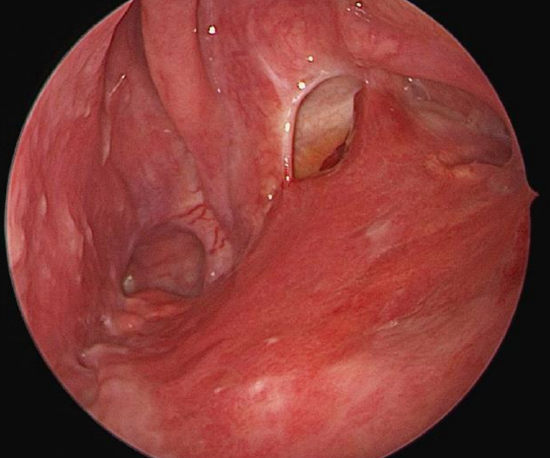
Figure 16: Transnasal view of flap at 17 days
Some useful references
- Moore EJ. Temporoparietal Fascia Flap. emedicine
- Smith J, Ducic Y, Adelson R. The utility of the temporalis muscle flap for oropharyngeal, base of tongue, and nasopharyngeal reconstruction. Otolaryngol Head Neck Surg 2005;132:373- 80
Other flaps described in The Open Access Atlas of Otolaryngology Head & Neck Operative Surgery
- Pectoralis major flap
- Buccinator myomucosal flap
- Buccal fat pad flap
- Nasolabial flap
- Deltopectoral flap
- Paramedian forehead flap
- Upper and lower trapezius flaps
- Cervicofacial flaps
- Submental artery island flap
- Supraclavicular flap
- Latissimus dorsi flap
- Local flaps for facial reconstruction
- Radial free forearm flap
- Free fibula flap
- Rectus abdominis flap
- Anterolateral free thigh flap
- Thoracodorsal artery scapular tip (TDAST) flap
- Principles and technique of microvascular anastomosis for free tissue transfer flaps in head and neck reconstructive surgery
Author & Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za