
3.15: Cleft Lip and Palate Surgical Techniques - Introduction and Philosophy
- Page ID
- 47880

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
CLEFT LIP AND PALATE SURGICAL TECHNIQUES: INTRODUCTION AND PHILOSOPHY
Kurt Butow and Roger Zwahlen
Facial cleft deformity comprises cleft lip and palate deformities, as well as clefts of facial structures not associated with a cleft lip or palate.
Cleft surgery requires a comprehensive knowledge of function (speech, occlusion, nasal airflow, middle ear function and facial muscles) and aesthetics, including racial specific features. The surgery comprises almost all types of cranio-maxillofacial and oral surgical interventions and involves both soft tissue (always 3-dimensional), and hard tissue (2- and 3-dimensional) corrective surgery. Appropriate treatment should be done at the best point in time i.e. neonatal period, toddler stage and childhood or during adolescence.
Multidisciplinary care
Optimal treatment can only be achieved in a multidisciplinary setting in which various specialties evaluate, examine, diagnose and treat patients according to treatment protocols. Patients, together with their parents/ caregivers, are reviewed yearly or two-yearly by all the multidisciplinary clinic specialties and disciplines e.g. during their birthday week. A multidisciplinary team typically comprises the following:
- Surgeon
- Orthodontist
- Speech and language pathologist
- Audiologist
- Pediatrician
- Community nurses
- Clinical psychologist
- Medical geneticist
- Pedodontist
- Oral hygienist
- Prosthodontist
Community nurses are the most important members of the clinic.
Surgeons should be able to treat every surgical aspect from childhood to adulthood, and should be familiar with primary, secondary and tertiary reconstructive procedures of facial soft tissue, facial hard tissue, and intraoral soft and hard tissue defects. Therefore, cleft surgeons need to be comprehensively trained in all aspects of cleft surgery and care, and be competent in primary, secondary and tertiary cleft treatment. Surgeons should be familiar with treating children with jaw-orthognathic suction and drinking plates (jaw-orthopedic devices) and know basic pediatric treatment regimens.
Whereas the optimal treatment for facial cleft deformity can only be offered in a multidisciplinary cleft clinic, solitary cleft lip deformities may be treated successfully in a non-multidisciplinary environment. During long-term follow-up, however, unpredictable abnormal tooth eruption overlying the cleft side and secondary deformities may occur. Secondary reconstruction due to cleft lip scarring, as well as cleft rhinoplasty at around 14 years of age might become necessary. This indicates the necessity that even patients suffering from minimal variations of cleft deformities need to be followed up in multidisciplinary clinics during their growth period.
Charity and mission surgery
Children in developing countries represent the most facial cleft deformities. However, most children with facial cleft deformities do not have access to multidisciplinary care and advanced treatment. The only hope for such children is nationally or internationally sponsored charity or mission surgical organizations. Cleft lips are the most obvious correctable facial deformity, and constitute an important part of aesthetic appearance, and affect patients’ personalities. It is estimated that about 90% of charity or mission surgeries only do cleft lip repairs, and do not address palatal repair which is very important for speech development and feeding. Continuous follow-up and interventions for secondary reconstructions, speech pathology, orthodontic and prosthodontic treatment also rarely exist for these unfortunate patients. Despite these shortcomings, it is important that the poorest of the poor, which represent most cleft patients, receive at least some type of basic treatment, even if only a cleft lip repair, in order to be accepted in their communities.
Requirements for best results
- Surgical protocols for facial cleft deformities, the sequence of surgical interventions, avoidance of revision surgery in the growing face, and continuous follow-up for about 16 years
- Alignment of dento-alveolar arches and nasal ala molding, where possible, and columella stretch-molding in bilateral cleft lip
- Selecting surgical procedures that cause the least long-term growth disturbances of facial hard and soft tissues and avoid occlusal disturbances and midfacial growth deficiency
- Selecting surgical procedures that provide the best aesthetic appearance
- Selecting surgical procedures that provide optimal results for soft palate function in terms of feeding and speech and that reduce middle ear effusions for better hearing
Initial cleft management
- Pediatric examination
- Community nurse consultation, especially for airway and feeding issues
- Speech therapy consultation for parents (if required)
- Surgical consultation and introduction of custom-made surgical protocol
- Psychological support for parents
- Functional jaw-orthognathic treatment or primary jaw-orthodontics immediately after birth (if required)
- Genetic counseling for parents and investigation of family history
Tessier Classification of Clefts

Figure 1: Tessier classification of cleft deformities
Figure 1 illustrates the Tessier classification of cleft deformities (1976) and is based on the anatomical position of the clefts.
The different types of Tessier clefts are numbered 0 to 14. These 15 different types of clefts can be put into 4 groups, based on their position: midline, paramedian, orbital and lateral clefts. The Tessier classification describes the clefts at soft tissue level as well as at bone level, because it appears that the soft tissue clefts can have a slightly different location on the face than the bony clefts.
Midline clefts are Tessier number 0 ("median craniofacial dysplasia"), number 14 (frontonasal dysplasia), and number 30 ("lower midline facial cleft", also known as "median mandibular cleft"). These clefts bisect the face vertically through the midline. Tessier number 0 bisects the maxilla and the nose, Tessier number 14 comes between the nose and the frontal bone. The Tessier number 30 facial cleft is through the tongue, lower lip and mandible. The tongue may be absent, hypoplastic, bifid, or even duplicated. People with this condition may be tongue-tied.
Paramedian clefts are Tessier number 1, 2, 12 and 13. These clefts are quite similar to the midline clefts, but they are further away from the midline. Tessier number 1 and 2 both come through the maxilla and the nose, in which Tessier number 2 is further from the midline (lateral) than number 1. Tessier number 12 is in extent of number 2, positioned between nose and frontal bone, while Tessier number 13 is in extent of number 1, also running between nose and forehead. Both 12 and 13 runs between the midline and the orbit.
Orbital clefts are Tessier numbers 3, 4, 5, 9, 10 and 11 are orbital clefts. These clefts all involve the orbit. Tessier numbers 3, 4, and 5 are positioned through the maxilla and the orbital floor. Tessier numbers 9, 10 and 11 are positioned between the upper side of the orbit and the forehead or between the upper side of the orbit and the temple of the head. Like the other clefts, Tessier number 11 is in extent to number 3, number 10 is in extent to number 4 and number 9 is in extent to number 5.
Lateral clefts are positioned horizontally on the face. These are Tessier numbers 6, 7 and 8. Tessier number 6 runs from the orbit to the cheek bone. Tessier number 7 is positioned on the line between the corner of the mouth and the ear. A possible lateral cleft comes from the corner of the mouth towards the ear, which gives the impression that the mouth is bigger. It’s also possible that the cleft begins at the ear and runs towards the mouth. Tessier number 8 runs from the outer corner of the eye towards the ear. The combination of a Tessier number 6-7-8 is seen in the Treacher Collins syndrome. Tessier number 7 is more related to hemifacial microsomia and number 8 is more related to Goldenhar syndrome.

Figure 2: Diagnostic key for cleft lip and palate
Figure 2 is a visual symbolic classification of cleft lip and palate cases. For documentation and classification purposes, clinical findings in cleft lip alveolus and palate patients are transferred into a “Y-scheme”. It represents a quick visual guide both regarding the anterior-posterior extension and regarding the distinction between partial and complete. The key in Figure 2 explains the structure of the “Y-scheme” related to cleft extensions and its colouring related to cleft completeness.
Cleft lips can be classified as follows:
- Micro-microform
- Mini-microform
- Microform
- Minor-form
- Total-/-Partial-incomplete (subcutaneous)
- Total / Complete
- Median facial dysgenesis

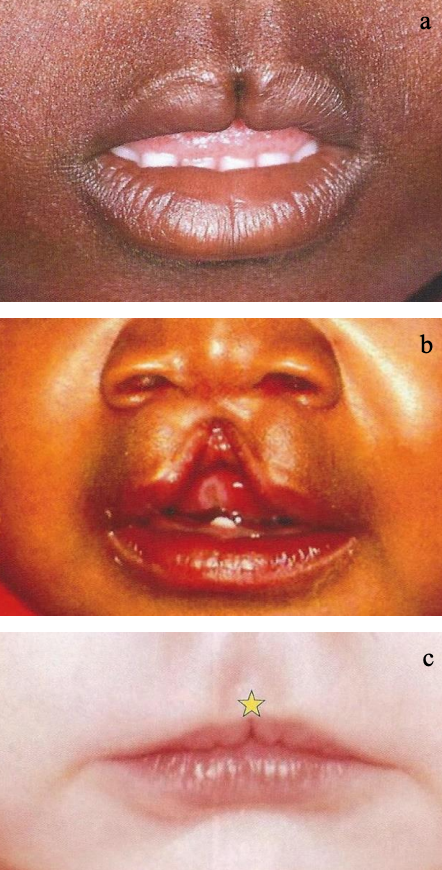
Figure 3a-c: Examples of types of cleft lips: Micro-microform ⇨; Mini-microform ✴︎; Minor-form ☆; Total / partial-incomplete (subcutaneous) △
Figure 3 illustrates examples of cleft lips (CL). The clinical picture of clefts may vary considerably, sometimes rendering their detection difficult. The pictures below highlight different cleft appearances, due to various degrees of cleft severity and its description under 1 to 7.
Clinical examples of cleft lips and palates
Cleft lip-alveolus (Figures 4a-c)

Figures 4a-c: Cleft lip-alveolus
The following three pictures show cases of cleft lip alveolus (abbreviated as CLA). No clefts can be found in the hard- and softpalate. Figure 4a depicts a bilateral atrophic cleft lip with a unilateral cleft alveolus, Figure 4b a wide left-sided cleft lip and cleft alveolus, and Figure 4c a very protrusive and rotated prolabium-premaxilla in a bilateral CLA.
Lip and/or alveolar bands

Figures 5a-d: Examples of lip-to-lip (Simonartz’) bands (1), lip-to-alveolar bands (2), and alveolar-to-alveolar bands (3)
The scheme in Figure 5a highlights three different types of detectable soft tissue adhesions between lips and/or alveolar processes in cleft patients. Figure 5b represents the Simonart’s Band, a lip to lip adhesion.
Figures 5c and 5d show clinical pictures of a lip to alveolus and an alveolus to alveolus adhesion, respectively.
Cleft Lip-Alveolus and Palate (CLAP)

Figures 6a-c: Lip and/or alveolar bands
The following three pictures show cases of cleft lip-alveolus and palate (abbreviated as CLAP). Figure 6a depicts a left-sided unilateral complete CLAP. Figures 6b and 6c display cases with complete bilateral CLAP. Additionally, Figure 6c highlights a very much anteriorly displaced and laterally rotated prolabium-premaxilla (white dotted circle).
Hard palate (hP) clefts
Figures 7a-d: Hard palate (hP) clefts
Figures 7a-d show different extensions of isolated clefts of the hard palate. Figure 7a shows a full view of the nasal septum/ vomer.
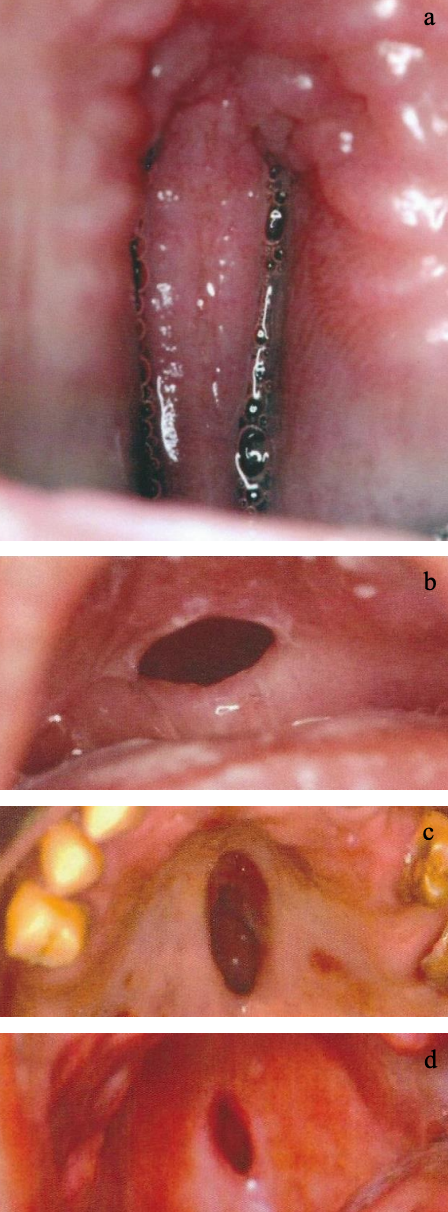
Hard and soft palate (hPsP) clefts

Figures 8a-c: Hard and soft palate (hPsP) clefts (Synechia/oral band ☆)
Figures 8a-c demonstrate three different combined hard and soft palate clefts (abbreviated hPsP). Figure 8a additionally focuses on a specific soft tissue adhesion, a synechiae, between the alveolar process and the tongue. Figures 8b and c show various extensions of combined hPsP clefts.
Soft palate (sP) clefts: Figures 9ab

Figures 9ab: Soft palate (sP) clefts
Figures 9a and b show soft palate clefts. As Figure 9a clearly shows a uvula on both sides of an asymmetric soft palate cleft, in Figure 9b the uvula is located entirely on the left side of the soft palate cleft.
Combination of clefts (Combi) (Figures 10ab)

Figures 10ab: Combi clefts
Combi cleft cases may present with a cleft lip and cleft soft palate (CL+sP) without necessarily involving the alveolar bone and hard palate as a CLAP case.
Median clefts (CL, CLA, CLAP)

Figures 11a-c: Median cleft – DeMyer II (a+c), DeMyer I (b+d) (d = holoprosencephaly)
Figures 11a-d highlight the vast variety of the clinical picture of median clefts. The anlage of various midline tissues might be missing, such as soft tissues like skin, muscle, but also alveolar and palatal bones. Whereas Figures 11a & 11c show a partial incomplete median cleft lip, a subcutaneous median cleft, respectively (DeMyer group II), Figures 11b & 11d demonstrate tissue deficiency due to a major non-anlage of midline structures (DeMyer group I).
Median cleft (lower lip, tongue)


Figures 12a-c: Median clefts of tongue, palate and lower lip
Figures 12a-c highlight the vast clinical variety of median clefts. The anlage of various midline tissues might be involved, presenting clinical pictures such as cleft tongue with additional central tissue and the hard palate in Figure 12a, as minor median cleft tongue in Figure 12b, and as median incomplete lower cleft lip in Figure 12c.
Lateral facial clefts = Tessier-7 cleft

Figures 13ab: Lateral clefts
Figure 13a displays a unilateral lateral facial cleft. A bilateral lateral facial cleft is shown in Figure 13b.
Oblique facial clefts (Figures 14a-c)

Figures 14a-c: Oblique facial clefts
Figures 14a-c show the clinical variety of oblique facial clefts, probably caused by amniotic bands during the intrauterine gestation (Figure 1). Figure 14a shows a left Tessier-3 cleft, Figure 14b Tessier-2 and Tessier-4 clefts on the right side, and Figure 14c a left Tessier-6 and a right Tessier-7 cleft.
Cleft Treatment Protocols from Neonate to Adult
Prior to initiation of treatment, a long-term strategy must be established: a so-called treatment/therapy protocol
1. General Treatment Protocol
Regular follow-ups
- Plate treatment for jaw-orthognathic or primary orthopedic reasons - 4 weekly
- Postoperative follow-up at week 2 and 8
- Annual follow-up during patient's birthday week (exception: for CL and sP, every 2 years, during patient's birthday week)
Other non-surgical specialists and involved disciplines
- Specialists e.g. orthodontist, community nurse, pediatrician and speech pathologist should attend every clinic
- If needed, attendance of other specialists, e.g. pedontist, prosthodontist and audiologist
- Others based on referral, such as anesthetist and pediatric neurologist
Pre-surgical examination
- Photographs
- Dental casts (if applicable)
- Blood tests (if applicable)
Non-surgical intervention
- Psychological support for parents with babies, for children and for adolescents
2. Nursing Protocol
Regular follow-up duties of community nurses
- Clinic management: arrange clinic times and patients' records, maintain photo-documentation, liaise with auxiliary disciplines related to social and family problems
- Check patients' attendance during normal and outside clinic hours, such as newborn consultation, appointments for plate manufacturing
- Help and support with feeding problems
- Organize preoperative visits of patients at their homes
- Advise re preoperative hospital admission and on inward period
- Call other hospitals to consult parents with newborn cleft babies
- Arrange surgical bookings for cleft babies
- Gather statistical data on new arrivals and on surgical interventions of cleft patients
- Reachable by phone for parents' nursing questions
- Involved in research
Pediatric nursing in surgical ward
- Implement pediatric nursing protocol re medication, nasogastric feeding, oral cavity cleaning, prevention of vomiting
- Assistance with suture removal
3. Pediatric pharmacological protocol
Medication and care
4. Surgical Protocol
a. Timing of surgery
| Pathology | Timing |
| CL | 5 mnths |
| CLA | 5 mnths |
| sP (CLAP) | 5 mnths |
| sPhP: Mirror-image protocol: hP closed before lip and ant nasal floor) | 7 mnths |
| CLAP | 7 mnths |
| Bilat CLA/CLAP: Columella lengthening | 12 mnths |
| hPsP: Hard palate cleft | 18 mnths |
| CLAP, hPsP, sP CLAP requires speech therapy | 2-4 yrs |
| CLAP, hPsP, sP CLAP requires fluorography exam | 4 yrs |
| CLAP, hPsP, sP: Velopharyngeal flap | 4 yrs |
| CLA, CLAP: Secondary osteoplasty (Ideal age: 9 years, but this depends on completeness of orthodontic presurgical treatment) | 9-13 yrs |
| Any cleft type: Orthognathic surgery | 14-18 yrs |
| CL, CLA, CLAP: Revision cleft lip and/or cleft nose. The ideal age is around 14 years. However, it depends on eventual orthognathic surgical reconstruction of midface or mandible | 14-18 yrs |
Table 1: Timing of surgery: CL (Cleft lip); sP (Soft palate); hP (Hard palate), CLAP (Cleft lip, anterior nasal floor + hard palate)
b. Cleft surgery: Mirror Image Protocol

Figure 15: surgical protocol or "reverse" surgical protocol or “Principle: from inside to outside”
A "mirror-image" protocol (Figure 15) is used to completely close primary cleft lips and palates for the following reasons:
Watertight closure of the entire cleft can only be achieved by perfect closure of the lip, anterior nasal floor, area between the dentoalveolar arches, from the anterior nasal floor to the hard palate and from the hard palate to the soft palate, with the surgical closure starting with the soft palate and working towards the lip. On the contrary, primary closure of cleft lip preceding the hard palate cleft closure will always lead to an anterior or a buccal oronasal fistula.
Closure of the soft palate should be considered between 5 and 7 months of age, as the phonetic age of babies begins around this time.
Closure of the hard palate should be done after the soft palate closure. This avoids babies experiencing compromised breathing during the recovery period. During the reconstructed soft pal-ate healing period, the hard palate is still open toward the nasal cavity i.e. breathing is not restricted. This is of utmost importance particularly in combined hard and soft palate clefts and especially in patients suffering from a FairbairnRobin triad, a subdivision of a Pierre Robin sequence.
c. Reasons for a surgical protocol
1. Achieve optimal closure and avoid oronasal fistula
- Close from inside-to-out-side
- Use mirror-image protocol
2. Use best predictable surgical techniques for complete closure (Table 2)
| Surgical techniques | |
| sP |
Intravelar veloplasty with tensor stitch to activate Eustachian tube Sommerlad's levator & palatoglossopharyngeal muscle repositioning and reconstruction, and an Ivanov's uvula reconstruction |
| hP |
Inferior or caudally based vomer flap or Superior or cranially based vomer flap with Polylactic acid resorbable sheet to cover vertical triangular defect for maintaining the blood clot and to achieve flat palatal healing |
| CA | Anterior nasal floor flap in cranial part of cleft |
| CL | Anatomical lip-plasty [unilateral type] and a Broadbent's modification or NoordhoffTrott [bilateral] type technique |
Table 2: Best predictable surgical techniques for complete closure
3. Achieve optimal speech development and occlusal function
4. Avoid midfacial growth disturbances (dysgnathia) by selecting the optimal primary surgical techniques
5. Avoid revision surgeries and excessive orthodontic treatment
Note about above surgical protocol
- These techniques are the authors’ preferred techniques, based on research and clinical observations
- It helps to achieve complete closure using minimally invasive surgery, and to minimize long-term growth disturbances
Recommended online text
Authors
Professor Kurt-W Bütow MChD (MFO Surg), DrMedDent, PhD, DSc, FCMFOS, Maxillo-Facial Surgery; Fellowship in Cleft Facial Deformities
University of Pretoria Cleft Palate Deformities Clinic
Pretoria, South Africa
kurt@butow.co.za
Roger Zwahlen DipMedDent, DipMed, DrMed, DrMedDent, Private Docent
FMHMKG, FEBOMFS, FIBCSOMS
Specialist in Oral and Maxillofacial Surgery
Practice Verdeja
Fribourg, Switzerland
rozwahlen@gmail.com
Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za