
13.2: Pregnancy
- Page ID
- 6843

Learning Objectives
- Learn about the changes to your body during pregnancy
It is crucial to consume healthy foods at every phase of life, beginning in the womb. Good nutrition is vital for any pregnancy and not only helps an expectant mother remain healthy, but also impacts the development of the fetus and ensures that the baby thrives in infancy and beyond. During pregnancy, a woman’s needs increase for certain nutrients more than for others. If these nutritional needs are not met, infants could suffer from low birth weight (a birth weight less than 5.5 pounds, which is 2,500 grams), among other developmental problems. Therefore, it is crucial to make careful dietary choices.

The Early Days of Pregnancy
For medical purposes, pregnancy is measured from the first day of a woman’s last menstrual period until childbirth, and typically lasts about forty weeks. Major changes begin to occur in the earliest days, often weeks before a woman even knows that she is pregnant. During this period, adequate nutrition supports cell division, tissue differentiation, and organ development. As each week passes, new milestones are reached. Therefore, women who are trying to conceive should make proper dietary choices to ensure the delivery of a healthy baby. Fathers-to-be should also consider their eating habits. A sedentary lifestyle and a diet low in fresh fruits and vegetables may affect male fertility. Men who drink too much alcohol may also damage the quantity and quality of their sperm[1].
For both men and women, adopting healthy habits also boosts general well-being and makes it possible to meet the demands of parenting.
tools for change
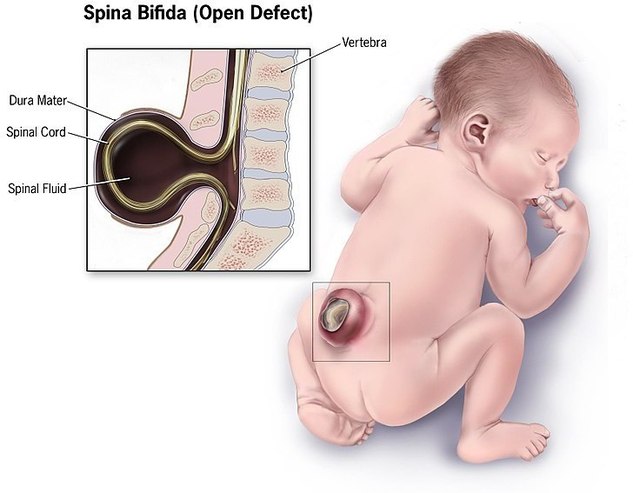
A pregnancy may happen unexpectedly. Therefore, it is important for all women of childbearing age to get 400 micrograms of folate per day prior to pregnancy and 600 micrograms per day during pregnancy. Folate, which is also known as folic acid, is crucial for the production of DNA and RNA and the synthesis of cells. A deficiency can cause megaloblastic anemia, or the development of abnormal red blood cells, in pregnant women. It can also have a profound affect on the unborn baby. Typically, folate intake has the greatest impact during the first eight weeks of pregnancy, when the neural tube closes. The neural tube develops into the fetus’s brain, and adequate folate reduces the risk of brain abnormalities or neural tube defects, which occur in one in a thousand pregnancies in North America each year. This vital nutrient also supports the spinal cord and its protective coverings. Inadequate folic acid can result in birth defects, such as spina bifida, which is the failure of the spinal column to close. The name “folate” is derived from the Latin word foliumfor leaf, and leafy green vegetables such as spinach and kale are excellent sources of it. Folate is also found in legumes, liver, and oranges. Additionally, since 1998, food manufacturers have been required to add folate to cereals and other grain products[2].
Weight Gain during Pregnancy
During pregnancy, a mother’s body changes in many ways. One of the most notable and significant changes is weight gain. If a pregnant woman does not gain enough weight, her unborn baby will be at risk. Poor weight gain, especially in the third trimester, could result not only in low birth weight, but also infant mortality and intellectual disabilities. Therefore, it is vital for a pregnant woman to maintain a healthy weight, and her weight prior to pregnancy has a major effect. Infant birth weight is one of the best indicators of a baby’s future health. Pregnant women of normal weight should gain between 25 and 35 pounds in total through the entire pregnancy. The precise amount that a mother should gain usually depends on her beginning body mass index (BMI). See Table \(\PageIndex{1}\) for The Institute of Medicine (IOM) recommendations.
Table \(\PageIndex{1}\): Body Mass Index and Pregnancy[3].
| Prepregnancy BMI | Weight Category | Recommended Weight Gain |
|---|---|---|
| Below 18.5 | Underweight | 28–40 lbs. |
| 18.5–24.9 | Normal | 25–35 lbs. |
| 25.0–29.9 | Overweight | 15–25 lbs. |
| Above 30.0 | Obese (all classes) | 11–20 lbs. |
Starting weight below or above the normal range can lead to different complications. Pregnant women with a prepregnancy BMI below twenty are at a higher risk of a preterm delivery and an underweight infant. Pregnant women with a prepregnancy BMI above thirty have an increased risk of the need for a cesarean section during delivery. Therefore, it is optimal to have a BMI in the normal range prior to pregnancy.
Generally, women gain 2 to 5 pounds in the first trimester. After that, it is best not to gain more than one pound per week. Some of the new weight is due to the growth of the fetus, while some is due to changes in the mother’s body that support the pregnancy. Weight gain often breaks down in the following manner as shown in Figure \(\PageIndex{3}\) 6 to 8 pounds of fetus, 1 to 2 pounds for the placenta (which supplies nutrients to the fetus and removes waste products), 2 to 3 pounds for the amniotic sac (which contains fluids that surround and cushion the fetus), 1 to 2 pounds in the breasts, 1 to 2 pounds in the uterus, 3 to 4 pounds of maternal blood, 3 to 4 pounds maternal fluids, and 8 to 10 pounds of extra maternal fat stores that will be needed for breastfeeding and delivery. Women who are pregnant with more than one fetus are advised to gain even more weight to ensure the health of their unborn babies.
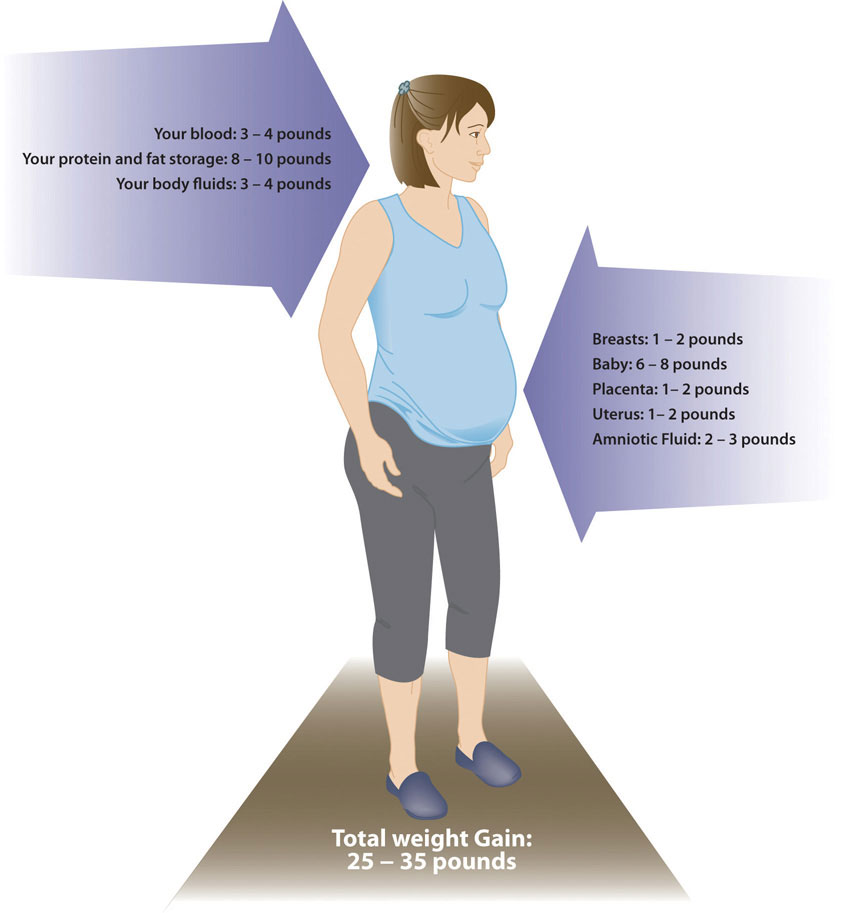
The weight an expectant mother gains during pregnancy is almost all lean tissue, including the placenta and fetus. Weight gain is not the only major change. A pregnant woman also will find that her breasts enlarge and that she has a tendency to retain water[4].
The pace of weight gain is also important. If a woman puts on weight too slowly, her physician may recommend nutritional counseling. If she gains weight too quickly, especially in the third trimester, it may be the result of edema, or swelling due to excess fluid accumulation. Rapid weight gain may also result from increased calorie consumption or a lack of exercise.
Weight Loss after Pregnancy
During labor, new mothers lose some of the weight they gained during pregnancy with the delivery of their child. In the following weeks, they continue to shed weight as they lose accumulated fluids and their blood volume returns to normal. Some studies have hypothesized that breastfeeding also helps a new mother lose some of the extra weight, although research is ongoing[5].
New mothers who gain a healthy amount of weight and participate in regular physical activity during their pregnancies also have an easier time shedding weight post-pregnancy. However, women who gain more weight than needed for a pregnancy typically retain that excess weight as body fat. If those few pounds increase a new mother’s BMI by a unit or more, that could lead to complications such as hypertension or Type 2 diabetes in future pregnancies or later in life.
Nutritional Requirements
As a mother’s body changes, so do her nutritional needs. Pregnant women must consume more calories and nutrients in the second and third trimesters than other adult women. However, the average recommended daily caloric intake can vary depending on activity level and the mother’s normal weight. Also, pregnant women should choose a high-quality, diverse diet, consume fresh foods, and prepare nutrient-rich meals. Steaming is the best way to cook vegetables. Vitamins are destroyed by overcooking, whereas uncooked vegetables and fruits have the highest vitamin content. It is also standard for pregnant women to take prenatal supplements to ensure adequate intake of the needed micronutrients.
Energy and Macronutrients
During the first trimester, a pregnant woman has the same energy requirements as normal and should consume the same number of calories as usual. However, as the pregnancy progresses, a woman must increase her caloric intake. According to the IOM, she should consume an additional 340 calories per day during the second trimester, and an additional 450 calories per day during the third trimester. This is partly due to an increase in metabolism, which rises during pregnancy and contributes to increased energy needs. A woman can easily meet these increased needs by consuming more nutrient-dense foods.
The recommended daily allowance, or RDA, of carbohydrates during pregnancy is about 175 to 265 grams per day to fuel fetal brain development. The best food sources for pregnant women include whole-grain breads and cereals, brown rice, root vegetables, legumes, and fruits. These and other unrefined carbohydrates provide nutrients, phytochemicals, antioxidants, and the extra 3 mg/day of fiber that is recommended during pregnancy. These foods also help to build the placenta and supply energy for the growth of the unborn baby.
During pregnancy, extra protein is needed for the synthesis of new maternal and fetal tissues. Protein builds muscle and other tissues, enzymes, antibodies, and hormones in both the mother and the unborn baby. Additional protein also supports increased blood volume and the production of amniotic fluid. The RDA of protein during pregnancy is 71 grams per day, which is 25 grams above the normal recommendation. Protein should be derived from healthy sources, such as lean red meat, white-meat poultry, legumes, nuts, seeds, eggs, and fish. Low-fat milk and other dairy products also provide protein, along with calcium and other nutrients.
There are no specific recommendations for fats in pregnancy, apart from following normal dietary guidelines. Although this is the case, it is recommended to increase the amount of essential fatty acids linoleic acid and ∝-linolenic acid because they are incorporated into the placenta and fetal tissues. Fats should make up 25 to 35 percent of daily calories, and those calories should come from healthy fats, such as avocados. It is not recommended for pregnant women to be on a very low-fat diet, since it would be hard to meet the needs of essential fatty acids and fat-soluble vitamins. Fatty acids are important during pregnancy because they support the baby’s brain and eye development.
Fluids
Fluid intake must also be monitored. According to the IOM, pregnant women should drink 2.3 liters (about 10 cups) of liquids per day to provide enough fluid for blood production. It is also important to drink liquids during physical activity or when it is hot and humid outside, to replace fluids lost to perspiration. The combination of a high-fiber diet and lots of liquids also helps to eliminate waste.
Pregnancy: Body Changes and Discomforts. US Department of Health and Human Services, Office on Women’s Health. www.womenshealth.gov/pregnanc...t/body-changes -discomforts.cfm. Updated September 27, 2010. Accessed December 2, 2017.
Vitamins and Minerals
The daily requirements for nonpregnant women change with the onset of a pregnancy. Taking a daily prenatal supplement or multivitamin helps to meet many nutritional needs. However, most of these requirements should be fulfilled with a healthy diet. The following table compares the normal levels of required vitamins and minerals to the levels needed during pregnancy. For pregnant women, the RDA of nearly all vitamins and minerals increases.
Table \(\PageIndex{2}\): Recommended Nutrient Intakes during Pregnancy.
| Nutrient | Nonpregnant Women | Pregnant Women |
|---|---|---|
| Vitamin A (mcg) | 700.0 | 770.0 |
| Vitamin B6 (mg) | 1.5 | 1.9 |
| Vitamin B12 (mcg) | 2.4 | 2.6 |
| Vitamin C (mg) | 75.0 | 85.0 |
| Vitamin D (mcg) | 5.0 | 5.0 |
| Vitamin E (mg) | 15.0 | 15.0 |
| Calcium (mg) | 1,000.0 | 1,000.0 |
| Folate (mcg) | 400.0 | 600 |
| Iron (mg) | 18.0 | 27.0 |
| Magnesium (mg) | 320.0 | 360.0 |
| Niacin (B3) (mg) | 14.0 | 18.0 |
| Phosphorus | 700.0 | 700.0 |
| Riboflavin (B2) (mg) | 1.1 | 1.4 |
| Thiamine (B1) (mg) | 1.1 | 1.4 |
| Zinc (mg) | 8.0 | 11.0 |
Source: Nutrition during Pregnancy: Part I: Weight Gain, Part II: Nutrient Supplements. Institute of Medicine. iom.edu/Reports/1990/Nutritio...pplements.aspx. Published January 1, 1990. Accessed November 22, 2017.
The micronutrients involved with building the skeleton—vitamin D, calcium, phosphorus, and magnesium—are crucial during pregnancy to support fetal bone development. Although the levels are the same as those for nonpregnant women, many women do not typically consume adequate amounts and should make an extra effort to meet those needs.
There is an increased need for all B vitamins during pregnancy. Adequate vitamin B6 supports the metabolism of amino acids, while more vitamin B12 is needed for the synthesis of red blood cells and DNA. Additional zinc is crucial for cell development and protein synthesis. The need for vitamin A also increases, and extra iron intake is important because of the increase in blood supply during pregnancy and to support the fetus and placenta. Iron is the one micronutrient that is almost impossible to obtain in adequate amounts from food sources only. Therefore, even if a pregnant woman consumes a healthy diet, there still is a need to take an iron supplement, in the form of ferrous salts. Also remember that folate needs increase during pregnancy to 600 micrograms per day to prevent neural tube defects. This micronutrient is crucial for fetal development because it helps produce the extra blood a woman’s body requires during pregnancy.
For most other minerals, recommended intakes are similar to those for nonpregnant women, although it is crucial for pregnant women to make sure to meet the RDAs to reduce the risk of birth defects. In addition, pregnant mothers should avoid exceeding any recommendations. Taking megadose supplements can lead to excessive amounts of certain micronutrients, such as vitamin A and zinc, which may produce toxic effects that can also result in birth defects.
Guide to Eating during Pregnancy
While pregnant women have an increased need for energy, vitamins, and minerals, energy increases are proportionally less than other macronutrient and micronutrient increases. So, nutrient-dense foods, which are higher in proportion of macronutrients and micronutrients relative to calories, are essential to a healthy diet. Examples of nutrient-dense foods include fruits, vegetables, whole grains, peas, beans, reduced-fat dairy, and lean meats. Pregnant women should be able to meet almost all of their increased needs via a healthy diet. However, expectant mothers should take a prenatal supplement to ensure an adequate intake of iron and folate. Here are some additional dietary guidelines for pregnant women[6]:
- Eat iron-rich or iron-fortified foods, including meat or meat alternatives, breads, and cereals, to help satisfy increased need for iron and prevent anemia.
- Include vitamin C-rich foods, such as orange juice, broccoli, or strawberries, to enhance iron absorption.
- Eat a well-balanced diet, including fruits, vegetables, whole grains, calcium-rich foods, lean meats, and a variety of cooked seafood (excluding fish that are high in mercury, such as swordfish and shark).
- Drink additional fluids, water especially.
Foods to Avoid
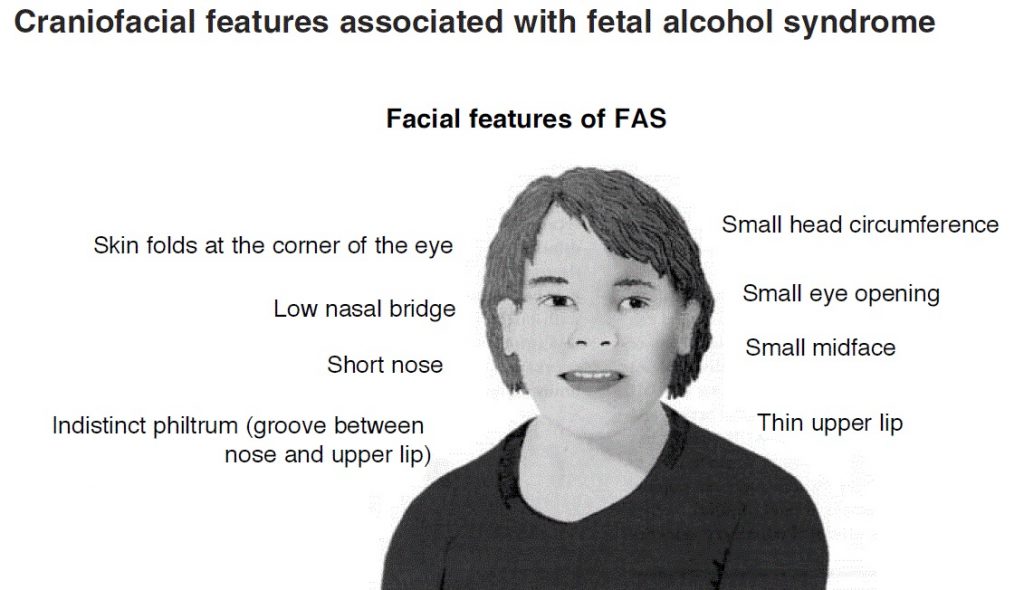
A number of substances can harm a growing fetus. Therefore, it is vital for women to avoid them throughout a pregnancy. Some are so detrimental that a woman should avoid them even if she suspects that she might be pregnant. For example, consumption of alcoholic beverages results in a range of abnormalities that fall under the umbrella of fetal alcohol spectrum disorders. They include learning and attention deficits, heart defects, and abnormal facial features (See Figure 13.3). Alcohol enters the unborn baby via the umbilical cord and can slow fetal growth, damage the brain, or even result in miscarriage. The effects of alcohol are most severe in the first trimester, when the organs are developing. As a result, there is no safe amount of alcohol that a pregnant woman can consume. Although pregnant women in the past may have participated in behavior that was not known to be risky at the time, such as drinking alcohol or smoking cigarettes, today we know that it is best to avoid those substances completely to protect the health of the unborn baby.
Pregnant women should also limit caffeine intake, which is found not only in coffee, but also tea, colas, cocoa, chocolate, and some over-the-counter painkillers. Some studies suggest that very high amounts of caffeine have been linked to babies born with low birth weights. The American Journal of Obstetrics and Gynecology released a report, which found that women who consume 200 milligrams or more of caffeine a day (which is the amount in 10 ounces of coffee or 25 ounces of tea) increase the risk of miscarriage[7].
Consuming large quantities of caffeine affects the pregnant mother as well, leading to irritability, anxiety, and insomnia. Most experts agree that small amounts of caffeine each day are safe (about one 8-ounce cup of coffee a day or less)[8]. However, that amount should not be exceeded.
Foodborne Illness
For both mother and child, foodborne illness can cause major health problems. For example, the foodborne illness caused by the bacteria Listeria monocytogenes can cause spontaneous abortion and fetal or newborn meningitis. According to the CDC, pregnant women are twenty times more likely to become infected with this disease, which is known as listeriosis, than nonpregnant, healthy adults. Symptoms include headaches, muscle aches, nausea, vomiting, and fever. If the infection spreads to the nervous system, it can result in a stiff neck, convulsions, or a feeling of disorientation[9].
Foods more likely to contain the bacteria that should be avoided are unpasteurized dairy products, especially soft cheeses, and also smoked seafood, hot dogs, paté, cold cuts, and uncooked meats. To avoid consuming contaminated foods, women who are pregnant or breastfeeding should take the following measures:
- Thoroughly rinse fruits and vegetables before eating them
- Keep cooked and ready-to-eat food separate from raw meat, poultry, and seafood
- Store food at 40° F (4° C) or below in the refrigerator and at 0° F (−18° C) in the freezer
- Refrigerate perishables, prepared food, or leftovers within two hours of preparation or eating
- Clean the refrigerator regularly and wipe up any spills right away
- Check the expiration dates of stored food once per week
- Cook hot dogs, cold cuts (e.g., deli meats/luncheon meat), and smoked seafood to 160° F
It is always important to avoid consuming contaminated food to prevent food poisoning. This is especially true during pregnancy. Heavy metal contaminants, particularly mercury, lead, and cadmium, pose risks to pregnant mothers. As a result, vegetables should be washed thoroughly or have their skins removed to avoid heavy metals.
Pregnant women can eat fish, ideally 8 to 12 ounces of different types each week. Expectant mothers are able to eat cooked shellfish such as shrimp, farm-raised fish such as salmon, and a maximum of 6 ounces of albacore, or white, tuna. However, they should avoid fish with high methylmercury levels, such as shark, swordfish, tilefish, and king mackerel. Pregnant women should also avoid consuming raw shellfish to avoid foodborne illness. The Environmental Defense Fund eco-rates fish to provide guidelines to consumers about the safest and most environmentally friendly choices. You can find ratings for fish and seafood at http://www.edf.org.
Physical Activity during Pregnancy
For most pregnant women, physical activity is a must and is recommended in the 2015 Dietary Guidelines for Americans. Regular exercise of moderate intensity, about thirty minutes per day most days of the week, keeps the heart and lungs healthy. It also helps to improve sleep and boosts mood and energy levels. In addition, women who exercise during pregnancy report fewer discomforts and may have an easier time losing excess weight after childbirth. Brisk walking, swimming, or an aerobics class geared toward expectant mothers are all great ways to get exercise during a pregnancy. Healthy women who already participate in vigorous activities, such as running, can continue doing so during pregnancy provided they discuss an exercise plan with their physicians.
However, pregnant women should avoid pastimes that could cause injury, such as soccer, football, and other contact sports, or activities that could lead to falls, such as horseback riding and downhill skiing. It may be best for pregnant women not to participate in certain sports, such as tennis, that require you to jump or change direction quickly. Scuba diving should also be avoided because it might result in the fetus developing decompression sickness. This potentially fatal condition results from a rapid decrease in pressure when a diver ascends too quickly[10].
Food Cravings and Aversions
Food aversions and cravings do not have a major impact unless food choices are extremely limited. The most common food aversions are milk, meats, pork, and liver. For most women, it is not harmful to indulge in the occasional craving, such as the desire for pickles and ice cream. However, a medical disorder known as pica is willingly consuming foods with little or no nutritive value, such as dirt, clay, and laundry starch. In some places this is a culturally accepted practice. However, it can be harmful if these substances take the place of nutritious foods or contain toxins.
Complications during Pregnancy
Expectant mothers may face different complications during the course of their pregnancy. They include certain medical conditions that could greatly impact a pregnancy if left untreated, such as gestational hypertension and gestational diabetes, which have diet and nutrition implications.
Gestational hypertension is a condition of high blood pressure during the second half of pregnancy.
First-time mothers are at a greater risk, along with women who have mothers or sisters who had gestational hypertension, women carrying multiple fetuses, women with a prior history of high blood pressure or kidney disease, and women who are overweight or obese when they become pregnant. Hypertension can prevent the placenta from getting enough blood, which would result in the baby getting less oxygen and nutrients. This can result in low birth weight, although most women with gestational hypertension can still deliver a healthy baby if the condition is detected and treated early.
Some risk factors can be controlled, such as diet, while others cannot, such as family history. If left untreated, gestational hypertension can lead to a serious complication called preeclampsia, which is sometimes referred to as toxemia. This disorder is marked by elevated blood pressure and protein in the urine and is associated with swelling. To prevent preeclampsia, the WHO recommends increasing calcium intake for women consuming diets low in that micronutrient, administering a low dosage of aspirin (75 milligrams), and increasing prenatal checkups[11].
About 4 percent of pregnant women suffer from a condition known as gestational diabetes, which is abnormal glucose tolerance during pregnancy. The body becomes resistant to the hormone insulin, which enables cells to transport glucose from the blood. Gestational diabetes is usually diagnosed around twenty-four to twenty-six weeks, although it is possible for the condition to develop later into a pregnancy. Signs and symptoms of this disease include extreme hunger, thirst, or fatigue. If blood sugar levels are not properly monitored and treated, the baby might gain too much weight and require a cesarean delivery. Diet and regular physical activity can help to manage this condition. Most patients who suffer from gestational diabetes also require daily insulin injections to boost the absorption of glucose from the bloodstream and promote the storage of glucose in the form of glycogen in liver and muscle cells. Gestational diabetes usually resolves after childbirth, although some women who suffer from this condition develop Type 2 diabetes later in life, particularly if they are overweight.
Footnotes
- Healthy Sperm: Improving Your Fertility. Mayo Clinic. 1998–2012 Mayo Foundation for Medical Education and Research. www.mayoclinic.com/health/fertility/MC00023. Accessed February 21, 2012.
- Folic Acid. MedlinePlus, a service of the National Institutes of Health. 1995–2012 http://www.nlm.nih.gov/medlineplus/d...ural/1017.html. Updated August 7, 2011. Accessed November 22, 2017.
- Weight Gain during Pregnancy: Reexamining the Guidelines. Institute of Medicine. https://www.nap.edu/resource/12584/R...-Pregnancy.pdf
- Weight Gain during Pregnancy. Utah Department of Health, Baby Your Baby. http://www.babyyourbaby.org/pregnancy/during. Published 2012. Accessed November 22, 2017.
- Stuebe AM, Rich-Edwards JW. The Reset Hypothesis: Lactation and Maternal Metabolism. , Am J Perinatol. 2009; 26(1), 81–88.
- Staying Healthy and Safe. US Department of Health and Human Services, Office on Women’s Health. Last updated March 5, 2009. https://www.womenshealth.gov/pregnan...althy-and-safe. Updated February 1, 2017. Accessed November 30, 2017.
- Weng X, Odouli R, Li DK. Maternal caffeine consumption during pregnancy and the risk of miscarriage: a prospective cohort study. Am J Obstet Gynecol 2008;198, 279.e1-279.e8.
- American Medical Association. Complete Guide to Prevention and Wellness. Hoboken, NJ: John Wiley & Sons, Inc.; 2008, 495.
- Listeria and Pregnancy. American Pregnancy Association. http://www.americanpregnancy.org/pre.../listeria.html. Updated March 10, 2017. Accessed November 29, 2017.
- Should I Exercise During My Pregnancy?. National Institutes of Health, and Friends of the National Library of Medicine. NIH Medline Plus. 2008; 3(1), 26. http://www.nlm.nih.gov/medlineplus/m...ter08pg26.html. Accessed December 2, 2017.
- WHO Recommendations for Prevention and Treatment of Pre-eclampsia and Eclampsia.World Health Organization. http://whqlibdoc.who.int/publication...548335_eng.pdf. Published 2011. Accessed June 8, 2012.
Contributors and Attributions
University of Hawai’i at Mānoa Food Science and Human Nutrition Program: Allison Calabrese, Cheryl Gibby, Billy Meinke, Marie Kainoa Fialkowski Revilla, and Alan Titchenal