
2.3: Chapter 3: Keys to Successful Programming
- Page ID
- 16014
In This Chapter…
- Guiding Principles
- Delivery of Services
- Improving Substance Abuse Treatment Systems and Programs
- Workforce Development and Staff Support
Overview
Many treatment agencies may recognize the need to provide quality care to persons with co-occurring disorders (COD), but see it as a daunting challenge beyond their resources. Programs that already have incorporated some elements of integrated services and want to do more may lack a clear framework for determining priorities. As programs look to improve their effectiveness in treating this population, what should they consider? How could the experience of other agencies inform their planning process? Are resources available that could help turn such a vision into reality? This chapter is designed both to help agencies that want to design programs for their clients with COD and to assist agencies that are trying to improve existing ones.
The chapter begins with a review of guiding principles derived from proven models, clinical experience, and the growing base of empirical evidence. Building on these guiding principles, the chapter turns to the core components for effective service delivery. It suggests that the provider needs to address in concrete terms the challenges of providing access, assessment, appropriate level of care, integrated treatment, comprehensive services, and continuity of care. This section provides guidance relevant to designing processes that are appropriate for this population within each of these key areas.
The chapter then moves onto a discussion of strategies for agencies that want to improve established systems, beginning with the too-familiar issue of how to access funding—a major hurdle for most, if not all, substance abuse treatment agencies. This portion of the chapter also gives an example of how one collaborative project crosses agency lines to share resources among a variety of partners and ensure continuity of care. The chapter then discusses difficulties of achieving equitable resource allocations for a venture of this nature, and highlights efforts to integrate research and practice.
Finally, the critical issues in workforce devel-opment are discussed, for without a well-pre-pared staff, the needs of these often-challenging clients cannot be met—regardless of what other systemic changes are made. The chapter describes the attitudes and values needed to successfully treat these clients, required compe-tencies, paths to professional development for those who wish to increase their skills in treat-ing clients with COD, and ways of avoiding staff burnout and reducing turnover—an espe-cially pressing concern for providers who work closely with this demanding population.
Guiding Principles
The consensus panel developed a list of guiding principles to serve as fundamental building blocks for programs that offer services to clients with COD (see Figure 3-1). These principles derive from a variety of sources: conceptual writings, well-articulated program models, a growing understanding of the essential features of COD, elements common to separate treatment models, clinical experience, and available empirical evidence. These principles may be applied at both a program level (e.g., providing literature for people with cognitive impairments) or at the individual level (e.g., addressing the client’s basic needs).
In identifying these principles, the TIP consensus panel recognizes that there are a number of carefully elaborated protocols to guide treatment for individuals with COD, including principles
identified by Drake and colleagues (1993) and by the Center for Mental Health Services Managed Care Initiative Panel (1998), as well as the assumptions that underlie the model Comprehensive Continuous Integrated Systems of Care described in chapter 2. The principles suggested in this chapter are consistent with these protocols, but reflect the specific focus of the consensus panel on how best to provide COD treatment in substance abuse treatment agencies. (However, the principles apply equally well to the treatment of COD in mental health agencies.)
The following section discusses each of the six principles in turn, highlighting the related field experience that underlies each one.
Employ a Recovery Perspective
There are two main features of the recovery perspective: It acknowledges that recovery is a long-term process of internal change, and it recognizes that these internal changes proceed through various stages. (See De Leon 1996 and Prochaska et al. 1992 for a detailed description. Also see chapter 5 of this TIP for a discussion of the recovery perspective as a guideline for practice.)
Figure 3-1
Six Guiding Principles in Treating Clients With COD
- Employ a recovery perspective.
- Adopt a multi-problem viewpoint.
- Develop a phased approach to treatment.
- Address specific real-life problems early in treatment.
- Plan for the client’s cognitive and functional impairments.
- Use support systems to maintain and extend treatment effectiveness.
The recovery perspective is applicable to clients who have COD. It generates at least two main principles for practice:
Develop a treatment plan that provides for continuity of care over time. In preparing this plan, the clinician should recognize that treatment may occur in different settings over time (i.e., residential, outpatient) and that much of the recovery process typically occurs outside of or following treatment (e.g., through participation in mutual self-help groups and through family and community support, including the faith community). It is important to reinforce long-term participation in these continuous care settings.
Devise treatment interventions that are specific to the tasks and challenges faced at each stage of the co-occurring disorder recovery process. Whether within the substance abuse treatment or mental health services system, the clinician is advised to use sensible stepwise approaches in developing and using treatment protocols. In addition, markers that are unique to individuals—such as those related to their cultural, social, or spiritual context—should be considered. It is important to engage the client in defining markers of progress meaningful to the individual and to each stage of recovery.
Adopt a Multi-Problem Viewpoint
People with COD generally have an array of mental health, medical, substance abuse, family, and social problems. Most are in need of substantial rehabilitation and habilitation (i.e., initial learning and acquisition of skills). Treatment should address immediate and longterm needs for housing, work, health care, and a supportive network. Therefore, services should be comprehensive to meet the multidimensional problems typically presented by clients with COD.
Develop a Phased Approach to Treatment
Many clinicians view clients as progressing though phases (Drake and Mueser 1996a; McHugo et al. 1995; Osher and Kofoed 1989; Sacks et al. 1998b). Generally, three to five phases are identified, including engagement, stabilization, treatment, and aftercare or continuing care. These phases are consistent with, and parallel to, stages identified in the recovery perspective. As noted above, use of these phases enables the clinician (whether within the substance abuse treatment or mental health services system) to develop and use effective, stage-appropriate treatment protocols. (See chapter 5 for a discussion of how to use motivational enhancement therapy appropriate to the client’s stage of recovery. Also see TIP 35, Enhancing Motivation for Change in Substance Abuse Treatment [Center for Substance Abuse Treatment (CSAT) 1999b]).
Address Specific Real-Life Problems Early in Treatment
The growing recognition that co-occurring disorders arise in a context of personal and social problems, with a corresponding disruption of personal and social life, has given rise to approaches that address specific life problems early in treatment. These approaches may incorporate case management and intensive case management to help clients find housing or handle legal and family matters. It may also be helpful to use specialized interventions that target important areas of client need, such as money management (e.g., Conrad et al. 1999) and housing-related support services (e.g., Clark and Rich 1999). Psychosocial rehabilitation, which helps the client develop the specific skills and approaches she needs to perform her chosen roles (e.g., student, employee, community member) also is a useful strategy for addressing these specific problems (Anthony 1996; Cnaan et al. 1990).
Solving such problems often is an important first step toward achieving client engagement in continuing treatment. Engagement is a critical part of substance abuse treatment generally and of treatment for COD specifically, since remaining in treatment for an adequate length of time is essential to achieving behavioral change.
Plan for the Client’s Cognitive and Functional Impairments
Services for clients with COD, especially those with more serious mental disorders, must be tailored to individual needs and functioning. Clients with COD often display cognitive and other functional impairments that affect their ability to comprehend information or complete tasks (CSAT 1998e; Sacks et al. 1997b). The manner in which interventions are presented must be compatible with client needs and functioning. Such impairments frequently call for relatively short, highly structured treatment sessions that are focused on practical life problems. Gradual pacing, visual aids, and repetition often are helpful. Even impairments that are comparatively subtle (e.g., certain learning disabilities) may still have significant impact on treatment success. Careful assessment of such impairments and a treatment plan consistent with the assessment are therefore essential.
Use Support Systems To Maintain and Extend Treatment Effectiveness
The mutual self-help movement, the family, the faith community, and other resources that exist within the client’s community can play an invaluable role in recovery. This can be particularly true for the client with COD, as many clients with COD have not enjoyed a consistently supportive environment for decades. In some cultures, the stigma surrounding substance use or mental disorders is so great that the client and even the entire family may be ostracized by the immediate community. Furthermore, the behaviors associated with active substance use may have alienated the client’s family and community. The clinician plays a role in ensuring that the client is aware of available support systems and motivated to use them effectively.
Mutual self-help
Based on the Alcoholics Anonymous model, the mutual self-help movement has grown to encompass a wide variety of addictions. Narcotics Anonymous and Cocaine Anonymous are two of the largest mutual self-help organizations for substance use disorders; Recoveries Anonymous and Schizophrenics Anonymous are among the best known for mental illness. Personal responsibility, self-management, and helping one another are the basic tenets of mutual self-help approaches. Such programs apply a broad spectrum of personal responsibility and peer support principles, usually including 12-Step methods that prescribe a planned regimen of change (see Peyrot 1985 for the history, structure, and approach of Narcotics Anonymous, representative of 12-Step approaches in general). However, in the past clients with COD felt that either their mental health or their substance use issues could not be addressed in a single-themed mutual self-help group; that has changed.
Mutual self-help principles, highly valued in the substance abuse treatment field, are now widely recognized as important components in the treatment of COD. Mutual self-help groups may be used as an adjunct to primary treatment, as a continuing feature of treatment in the community, or both. These groups not only provide a vital means of support during outpatient treatment, but also are used commonly in residential programs such as therapeutic communities. As clients gain employment, travel, or relocate, mutual self-help meetings may become the most easily accessible means of providing continuity of care. For a more extensive discussion of dual recovery mutual self-help programs applicable to persons with COD, see chapter 7.
Building community
The need to build an enduring community arises from three interrelated factors—the persistent nature of COD, the recognized effectiveness of mutual self-help principles, and the importance of client empowerment. The therapeutic community (TC), modified mutual self-help programs for COD (e.g., Double Trouble in Recovery), and the client consumer movement all reflect an understanding of the critical role clients play in their own recovery, as well as the recognition that support from other clients with similar problems promotes and sustains change.
Reintegration with family and community
The client with COD who successfully completes treatment must face the fragility of recovery, the toxicity of the past environment, and the negative impact of previous associates who may encourage drug or alcohol use and illicit or maladaptive behaviors. There is a need for groups and activities that support change. In this context it is important that these clients receive support from family and significant others where that support is available or can be developed. There is also the need to help the client reintegrate into the community through such resources as religious, recreation, and social organizations. (See chapter 6 for a discussion of continuing care issues in treatment.)
Delivery of Services
While the guiding principles described above serve as the fundamental building blocks for effective treatment, ensuring effective treatment requires attention to other variables. This section discusses six core components that form the ideal delivery of services for clients with COD. These include:
- Providing access
- Completing a full assessment
- Providing an appropriate level of care
- Achieving integrated treatment
- Providing comprehensive services
- Ensuring continuity of care
Providing Access
“Access” refers to the process by which a person with COD makes initial contact with the service system, receives an initial evaluation, and is welcomed into services that are appropriate for his or her needs.
Access occurs in four main ways:
- Routine access for individuals seeking services who are not in crisis
- Crisis access for individuals requiring immediate services due to an emergency
- Outreach, in which agencies target individuals in great need (e.g., people who are homeless) who are not seeking services or cannot access ordinary routine or crisis services
- Access that is involuntary, coerced, or mandated by the criminal justice system, employers, or the child welfare system
Treatment access may be complicated by clients’ criminal justice involvement, homelessness, or health status. CSAT’s “no wrong door” policy should be applied to the full range of clients with COD, and programs should address obstacles that bar entry to treatment for either the mental or substance use dis-orders. (See chapter 7 for recommendations on removing systemic barriers to care and the text box on p. 42 for more on CSAT’s “no wrong door” policy.)
It is important that clients receive support from family and significant others where that support is available or can be developed.
Completing a Full Assessment
While chapter 4 provides a complete description of the assessment process, this section highlights several important features of assessment that must be considered in the context of effective service delivery. Assessment of individuals with COD involves a combination of the following:
- Screening to detect the possible presence of COD in the setting where the client is first seen for treatment
- Evaluation of background factors (family, trauma history, marital status, health, education and work history), mental disorders, substance abuse, and related medical and psychosocial problems (e.g., living circumstances, employment, family) that are critical to address in treatment planning
- Diagnosis of the type and severity of substance use and mental disorders
- Initial matching of individual client to services (often, this must be done before a full assessment is completed and diagnoses clarified; also, the client’s motivation to change with regard to one or more of the co-occurring disorders may not be well established)
- Appraisal of existing social and community support systems
- Continuous evaluation (that is, re-evaluation over time as needs and symptoms change and as more information becomes available)
The challenge of assessment for individuals with COD in any system involves maximizing the likelihood of the identification of COD, immediately facilitating accurate treatment planning, and revising treatment over time as the client’s needs change.
Providing an Appropriate Level of Care
Clients enter the treatment system at various levels of need and encounter agencies with varying capacity to meet those needs. Ideally, clients should be placed in the level of care appropriate to the severity of both their substance use disorder and their mental illness.
The American Society of Addiction Medicine’s (ASAM) classification is one standard way of identifying programs that offer the needed services. As described in chapter 2, ASAM describes programs’ ability to address COD as “addiction only services,” “dual diagnosis capable,” and “dual diagnosis enhanced.”
Making “No Wrong Door” a Reality
CSAT’s “no wrong door” policy states that effective systems must ensure that an individual needing treatment will be identified and assessed and will receive treatment, either directly or through appropriate referral, no matter where he or she enters the realm of services (CSAT 2000a). The consensus panel strongly endorses this policy.
The focus of the “no wrong door” imperative is on constructing the healthcare delivery system so that treatment access is available at any point of entry. A client with COD needing treatment might enter the service system by means of primary healthcare facilities, homeless shelters, social service agencies, emergency rooms, or criminal justice settings. Some clients require the creation of a “right door” for treatment entry—for example, mobile outreach teams who can access clients with COD who are unlikely to knock on the door of any treatment facility.
The “no wrong door” approach has five major implications for service planning:
- Assessment, referral, and treatment planning for all settings must be consistent with a “no wrong door” policy.
- Creative outreach strategies may be needed to encourage some people to engage in treatment.
- Programs and staff may need to change expectations and program requirements to engage reluctant and “unmotivated” clients.
- Treatment plans should be based on clients’ needs and should respond to changes as they progress through stages of treatment.
- The overall system of care needs to be seamless, providing continuity of care across service systems. This can only be achieved through an established pattern of interagency cooperation or a clear willingness to attain that cooperation.
While recognizing ASAM’s contribution, the consensus panel suggests an alternative classification system: basic, intermediate, advanced, or fully integrated. As conceived by the consensus panel
- A basic program has the capacity to provide treatment for one disorder, but also screens for the other disorder and can access necessary consultations.
- A program with an intermediate level of capacity tends to focus primarily on one disorder without substantial modification to its usual treatment, but also explicitly addresses some specific needs of the other disorder. For example, a substance abuse treatment program may recognize the importance of continued use of psychiatric medications in recovery, or a psychiatrist could provide motivational interviewing regarding substance use while prescribing medication for mental disorders.
- A program with an advanced level of capacity provides integrated substance abuse treatment and mental health services for clients with COD. Several program models of this sort are described in chapter 6. Essentially, these programs address COD using an integrated perspective and provide services for both disorders. This usually means strengthening substance abuse treatment in the mental health setting by adding interventions such as mutual self-help and relapse prevention groups. It also means adding mental health services, such as psychoeducational classes on mental disorder symptoms and groups for medication monitoring, in substance abuse treatment settings. Collaboration with other agencies may add to the comprehensiveness of services.
- A program that is fully integrated actively combines substance abuse and mental health interventions to treat disorders, related problems, and the whole person more effectively.
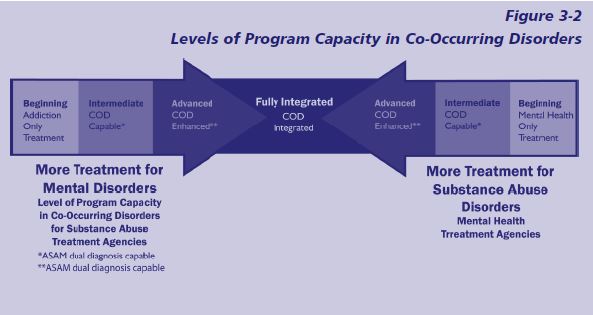
The suggested classification has several advantages. For one, it avoids the use of the term “dual diagnosis” (instead of COD) and allows a more general, flexible approach to describing capacity without specific criteria. In addition, the recommended classification system conceptualizes a bidirectionality of movement where either substance abuse or mental health agencies can advance toward more integrated care for clients with COD, as shown in Figure 3-2 (p. 44).
Figure 3-2 depicts a model of basic, intermediate (COD capable), and advanced (COD enhanced) programming within mental health services and substance abuse treatment systems. The idea of integrated COD treatment is shown in the center. For the purpose of this TIP, both mental health and substance abuse treatment providers may be conceived of as beginning, intermediate, or advanced in terms of their progress toward the highest level of capacity to treat persons with COD.
It should also be recognized that not all services want or need to be fully integrated, since many clients do not need a full array of services. (See Figure 2-1 in chapter 2.) In Figure 3-2, the middle box—fully integrated—refers to a system that has achieved an integrated setting in which staff, administration, regulations, and funding streams are fully integrated.
Achieving Integrated Treatment
The concept of integrated treatment for persons with severe mental disorders and substance use disorders, as articulated by Minkoff (1989), emphasized the need for correlation between the treatment models for mental health services and substance abuse treatment in a residential setting. Minkoff’s model stressed the importance of well-coordinated, stage-specific treatment (i.e., engagement, primary treatment, continuing care) of substance use and mental disorders, with emphasis on dual recovery goals as well and the use effective treatment strategies from both the mental health services and the substance abuse treatment fields.
During the last decade integrated treatment continued to evolve. Several successful treatment models have been described for addiction settings (Charney et al. 2001; McLellan et al. 1993; Saxon and Calsyn 1995; Weisner et al. 2001), including the addition of psychiatric and mental health services to methadone treatment (Kraft et al. 1997; Woody et al. 1983), and a modified therapeutic community for providing integrated care to persons with COD (De Leon 1993b; Guydish et al. 1994; Sacks 2000; Sacks et al. 1997a, b, 1998a, 2002). Likewise, the literature also describes numerous models for mental health settings (CSAT 1994a; Drake and Mueser 1996b; Lehman and Dixon 1995; Minkoff and Drake 1991; Zimberg 1993). Figure 3-3 illustrates one vision of a comprehensive, fully integrated approach to treatment for persons with severe mental disorders and substance use disorders from the mental health literature. However, as noted in the following section, programs may be integrated in a variety of ways.
The literature from both the substance abuse and mental health fields has evolved to describe integrated treatment as a unified treatment approach to meet the substance abuse, mental health, and related needs of a client. It is the preferred model of treatment.
Integrated treatment can occur on different levels and through different mechanisms. For example:
- One clinician delivers a variety of needed services.
- Two or more clinicians work together to provide needed services.
- A clinician may consult with other specialties and then integrate that consultation into the care provided.
- A clinician may coordinate a variety of efforts in an individualized treatment plan that integrates the needed services. For example, if someone with housing needs was not accepted at certain facilities, the clinician might work with a State-level community-housing program to find the transitional or supported housing the client needs.
- One program or program model (e.g., modified TC or Assertive Community Treatment) can provide integrated care.
- Multiple agencies can join together to create a program that will serve a specific population. For example, a substance abuse treatment program, a mental health center, a local housing authority, a foundation, a county government funding agency, and a neighborhood association could join together to establish a treatment center to serve women with COD and their children.
Integrated treatment also is based on positive working relationships between service providers. The National Association of State Mental Health Program Directors (NASMHPD) and the National Association of State Alcohol and Drug Abuse Directors’ (NASADAD) four-quadrant category framework described in chapter 2 provides a useful structure for fostering consultation, collaboration, and integration among systems and providers to deliver appropriate care to every client with COD (see chapter 2, Figure 2-1). According to the NASMHPD–NASADAD (1999) framework
- Consultation refers to the traditional types of informal relationships among providers—from referrals to requests for exchanging information and keeping each other informed. The framework calls for particular attention to the consultation relationship during identification, engagement, prevention, and early intervention activities.
- Collaboration is essential when a person who is receiving care in one treatment setting also requires services from another provider. Collaboration is distinguished from consultation on the basis of the formal quality of collaborative agreements, such as memoranda of understanding or service contracts, which document the roles and responsibilities each party will assume in a continuing relationship. For example, parties must ensure that they can share information without violating Federal Law 42 C.F.R. Part 2 on confidentiality (see appendix K for more information). This will require the client to give written authorization for release of information to all providers.
- Integration denotes “those relationships among mental health and substance abuse providers in which the contributions of professionals in both fields are moved into a single treatment setting and treatment regimen” (p. 15).
For the purposes of this TIP, integration is seen as a continuum. Depending on the needs of the client and the constraints and resources of particular systems, appropriate degrees and means of integration will differ.
Figure 3-3
A Vision of Fully Integrated Treatment for COD
- The client participates in one program that provides treatment for both disorders.
- The client’s mental and substance use disorders are treated by the same clinicians.
- The clinicians are trained in psychopathology, assessment, and treatment strategies for both mental and substance use disorders.
- The clinicians offer substance abuse treatments tailored for clients who have severe mental disorders.
- The focus is on preventing anxiety rather than breaking through denial.
- Emphasis is placed on trust, understanding, and learning.
- Treatment is characterized by a slow pace and a long-term perspective.
- Providers offer stagewise and motivational counseling.
- Supportive clinicians are readily available.
- 12-Step groups are available to those who choose to participate and can benefit from participation.
- Neuroleptics and other pharmacotherapies are indicated according to clients’ psychiatric and other medical
needs.
Source: Adapted from Drake et al. 1998b, p. 591.
Providing Comprehensive Services
People with COD have a range of medical and social problems—multidimensional problems that require comprehensive services. In addition to treatment for their substance use and mental disorders, these clients often require a variety of other services to address other social problems and stabilize their living conditions. Treatment providers should be prepared to help clients access a broad array of services, including life skills development, English as a second language, parenting, nutrition, and employment assistance.
McLellan and colleagues have shown the need for wraparound services to address difficult-to treat public-sector clients, not all of whom were diagnosed with COD (Gould et al. 2000; McLellan et al. 1997). Two areas of particular value, highlighted below, are housing and work.
Housing
The high proportion of homelessness among clients with COD has focused attention on the importance of providing housing for people with COD and of integrating housing into treatment. Approaches vary from those that provide housing at the point of entry into the service system combined with case management and supportive services (Tsemberis and Asmussen 1999), to those that provide housing as a reward contingent on successful completion of treatment (Milby et al. 1996; Schumacher et al. 1995), or as part of a continuing care strategy that combines housing and continuing care services (Sacks et al. 1998a, 2003a).
Addressing housing needs requires an ongoing relationship with housing authorities, landlords, and other housing providers. Groups and seminars that discuss housing issues also may be necessary to help clients with COD transition from residential treatment to housing. Another effective strategy for easing the transition has been organizing and coordinating housing tours with supportive housing programs. Finally, relapse prevention efforts are essential, since substance abuse generally disqualifies clients from public housing in the community.
Work
Vocational rehabilitation has long been one of the services offered to clients recovering from mental disorders and, to some degree, to those recovering from substance use disorders. However, in the past clients often were expected first to maintain a period of abstinence. As a result of this policy, people with serious mental disorders often were underserved, if served at all (CSAT 2000c). For people with COD, Blankertz and colleagues contend that, “work can serve as a rehabilitative tool and be an integral part of the process of stabilizing the mental illness and attaining sobriety” (Blankertz et al. 1998, p. 114).
The fact is that many individuals with COD are unemployed. However, it is unreasonable to expect employers to tolerate employees who are actively using alcohol on the job or who violate their drug-free workplace policies. Therefore, if work is to become an achievable goal for individuals with COD, vocational rehabilitation and substance abuse treatment must be closely integrated into mental health rehabilitation (Blankertz et al. 1998). For more information about incorporating vocational rehabilitation into treatment, see TIP 38, Integrating Substance Abuse Treatment and Vocational Services (CSAT 2000c).
Ensuring Continuity of Care
Continuity of care implies coordination of care as clients move across different service systems (e.g., Morrissey et al. 1997). Since both substance use and mental disorders frequently are long-term conditions, treatment for persons with COD should take into consideration rehabilitation and recovery over a significant period of time. Therefore, to be effective, treatment must address the three features that characterize continuity of care:
- Consistency between primary treatment and ancillary services
- Seamlessness as clients move across levels of care (e.g., from residential to outpatient treatment)
- Coordination of present and past treatment episodes
It is important to set up systems that prevent gaps between service system levels and between clinic-based services and those outside the clinic. The ideal is to include outreach, employment, housing, health care and medication, financial supports, recreational activities, and social networks in a comprehensive and integrated service delivery system.
Empirical evidence related to continuity of care
Evidence for the benefits of ensuring continuity of care comes from multiple sources. In one study of criminal justice populations not specifically identified as having COD, Wexler and colleagues (1999) found that at 3 years post-treatment only 27 percent of those prison program completers who also completed an aftercare program were returned to custody. In contrast, about three-fourths of the subjects in all other study groups were returned. Similar findings have been reported by Knight and colleagues (1999). Although selection bias exists in these studies for entry into aftercare, the long-term outcomes suggest the critical role of aftercare in maintaining positive treatment effects in the criminal justice population.
A study of homeless clients with COD provided further evidence (again with selection bias into aftercare) that after-care is crucial to positive treatment out-comes. In this study, clients who lived in supported housing after residing in a modified therapeutic community demonstrated reductions in antisocial behavior occurring during the residential modified therapeutic community program and stabilizing during supported housing, while increases in prosocial behavior were largely incremental and continuous throughout both the residential and supported housing programs (Sacks et al. 2003a).
Continuity of care implies coordination of care as clients move across different service systems.
Organizing continuity of care
In organizing continuity of care—a high-priority aspect of any treatment plan for a client with COD—the substance abuse treatment agency must carefully consider and strive to overcome systemic barriers. It is important to recognize that the public mental health and substance abuse treatment systems have evolved in different ways, and these differing histories must be recognized as collaborative ventures are formed.
Community mental health centers were created to be relatively comprehensive in nature, but have not been funded to deliver comprehensive services. Furthermore, there are wide variations in the types of mental disorders that publicly funded mental health centers are permitted to treat; many restrict their services to those in acute crisis or who have serious and persistent mental illnesses, such as schizophrenia, bipolar affective disorder, or major depression. Many States explicitly prevent public mental health programs from treating those with primary substance use disorders.
Substance abuse treatment programs exist within a variety of organizational structures. Many of them are stand-alone substance abuse treatment programs, several are part of comprehensive drug treatment agencies, some are affiliated with hospitals, some are located within hospitals, many have evolved as part of the criminal justice system, some exist in community mental health settings, and still others are faith-based programs. Many substance abuse treatment programs are the last refuge of the most underserved populations (e.g., the homeless).
The different organizational structures and settings in which services occur influence the ease or difficulty of providing a service delivery network that is integrated, comprehensive, and continuous. Many of the larger drug treatment agencies are to be commended for developing state-of-the-art programming for COD, and some smaller programs also have extended themselves to serve this population. Nevertheless, the strains imposed by organizational and system constraints should be recognized. As substance abuse treatment agencies continue to develop their capabilities for treating clients with COD, the consensus panel recommends that groups of providers organize themselves into coherent systems of care that enable them to provide comprehensive services.
An example of a collaborative that promotes the development of a local infrastructure in support of co-occurring treatment is the Co-Occurring Collaborative of Southern Maine. The Collaborative’s ways of working, accomplishments, and the critical elements for success identified at the close of Figure 3-4 may well inspire others to weave similar structures, crossing agency boundaries to better serve shared clients.
Improving Substance Abuse Treatment Systems and Programs
Critical challenges face substance abuse treatment systems and programs that are intent on improving care for clients with COD. One of the most critical of these is how to organize a system that will provide continuity of care for these clients, who, as noted previously, often have multifaceted needs and require long-term treatment plans. Another, of course, is how to access funding for program improvement. When treatment providers from different systems cooperate, equitable allocation of funds also becomes an issue. Finally, at every level there is the problem of how best to integrate research and practice to give clients the benefit of the proven treatment strategies. This section addresses each of these major concerns in turn.
Assessing the Agency’s Potential To Serve Clients With COD
Every agency that already is treating or planning to treat clients with COD should assess the current profile of its clients, as well as the estimated number and type of potential new clients in the community. It also must consider its current capabilities, its resources and limitations, and the services it wants to provide in the future.
Programs should consider performing a needs assessment to determine the prevalence of COD in their client population, the demographics of those clients, and the nature of the disorders and accompanying problems they present. These data help create a picture of client needs that can be useful not only to the agency itself, but also to other systems of care at various levels. All levels of government demand some form of needs assessment from provider agencies. Block grant requirements from the Federal government require a statewide needs assessment. In turn, States look to regional and county groups to perform a needs assessment focused on the local level. Local needs assessment information feeds back to the State level and is used to develop a statewide picture that, in turn, is provided to higher-level funding authorities. The data generated through needs assessments also can be used to demonstrate need in support of grant proposals for increasing service capacity prepared by the treatment agency.
Figure 3-4
The Co-Occurring Collaborative of Southern Maine
The Co-Occurring Collaborative of Southern Maine, a 501(c)(3) nonprofit corporation, is an alliance of member agencies, consumers, and family members in Cumberland County in southern Maine. Formed in 1992 through a State initiative on COD, the Collaborative provided the umbrella structure for a demonstration grant from The Bingham Program and The Robert Wood Johnson Foundation. It received additional support from Maine’s Office of Substance Abuse and Maine’s Medicaid Program for a project comparing the efficacy of integrated and coordinated care. The Collaborative has continued its work beyond the 3-year demonstration grant with funding from the Maine Office of Substance Abuse, becoming an integral part of the community’s efforts to address COD. In 1998, the Collaborative formalized its structure by becoming a Maine nonprofit corporation.
The number of member agencies has expanded from an initial dozen to more than 30, including consumer groups, family groups, and mental health, substance abuse, criminal justice, HIV, and public health service providers. Each member agency has an identified liaison who serves as the bridge between the Collaborative and the agency. Each member agency formally commits through a memorandum of understanding to do the following:
- Support the Collaborative’s mission.
- Examine and make changes to the services and organizational structures to support improved service provision for persons with COD.
- Exchange information, share resources, and alter activities to enhance the capacities of all agencies to improve services for persons with COD.
- Participate actively in, and share responsibility for, the Collaborative.
The Collaborative structure provides a mechanism for cross-agency and cross-disciplinary communication, coordination, training and education, creative interagency problemsolving, resource development for co-occurring recovery capacity, and advocacy. The Collaborative’s accomplishments to date include
- Promoting dual competence expectations in the workforce
- Obtaining grants and collaborating on grant submission
- Expanding consumer, family, and provider partnerships
- Developing the mutual self-help option of dual recovery
- Supporting diversion planning from the criminal justice system
- Supporting the creation of an Assertive Community Treatment team for individuals with COD
- Creating a community service consultation team
- Supporting transfer of knowledge to develop new clinical models for treatment of persons with personality and substance use disorders
To achieve success in forging a collaborative structure, the following were found to be critical elements:
- Inviting all relevant agencies to participate and air their concerns
- Nurturing one-to-one relationships among service providers across service sectors
- Creating and maintaining a shared knowledge base and a common vision
- Collaboration, support, and empowerment
- Early and frequent successes
- Encouraging participation in planning and decisionmaking
- Clarifying roles and process
- Ensuring ongoing consumer and family participation
- Conducting periodic self-review
- Having visionary, consistent, and effective leadership
It is important to determine what changes need to be made with respect to staff, training, accreditation, and other factors to provide effective services for clients with COD. The agency also should know what resources and services are already available within their local and State systems of care before deciding what services to provide. This assessment of community capacity and the resulting decisionmaking process should involve all stakeholders in the program. Whatever changes the provider decides to make will require an active commitment from all levels of staff as well as from members of the community, advocacy groups, and other interested parties.
The various classification systems described previously can be used to identify missing levels of care and gaps in specific services. Such tools permit clinicians to relate program services to clients’ needs for specific activities. They also enable planners to identify gaps in the current system of care and then to design programs that address these gaps. Figure 3-5 provides a list of domains and questions to guide agencies in assessing their potential to serve clients with COD. In doing so, it is assumed that each agency will use the best approach to each task that is possible, given its level of resources. It may, for example, need to use estimates rather than precise data in some instances.
Accessing Funding
System components and financing principles
Both mental health services and substance abuse treatment systems must face the challenge of obtaining funding that supports programming for clients with COD. For substance abuse treatment agencies, which are seeing more clients with COD and clients with more serious COD, it often is difficult to obtain funds to provide needed screening, assessment, specialized mental health service enhancement, and case management.
Developing a comprehensive system of care for people with COD requires committed leadership, joint planning, and the willingness and ability to find creative solutions to difficult problems. Financing a comprehensive system of care requires no less a commitment of time, creativity, and expertise. The process of continuing dialog between NASMHPD and NASADAD has identified key system development components and financing principles shown in Figure 3-6 (p. 52). Like the conceptual framework, these components and principles represent a set of flexible guidelines that can be adapted for use in any State or community.
Each of the six financing principles is a critical element of success and is described below:
- Plan To Purchase Together. It has been found that “in most successful demonstration programs for people with co-occurring disorders, the State mental health agency and the State alcohol and drug abuse agency jointly planned and purchased services” (NASMHPD and NASADAD 2000, pp. 19–20).
- Define the Population. Individuals with COD may fall into any of the four quadrants. Program services must target populations based on the severity of their mental or substance use disorders, among other considerations. However, it is important to keep in mind that due to the illegality of drug use denying services to those whose current condition is not severe may increase the severity of problems associated with that drug use, increasing severity by producing arrests, job loss, and conflicts with the child welfare system.
- Secure Financing. The following section of this chapter will provide some suggestions on this challenging and often complex task.
- Purchase Effective Services. It is important to purchase services that research has shown to be effective. Unfortunately, COD research tends to focus on those with serious mental disorders. As a result, guidance on which strategies are most cost-effective in treating persons with less serious mental disorders and co-occurring substance use disorders is not readily available.
- Purchase Performance. NASMHPD and NASADAD strongly recommend performance-based contracts that focus on outcomes. “A program’s effectiveness should be judged not only by how many people it serves or units of service it delivers, but rather by the level of real change it helps bring about in the lives of consumers who have co-occurring mental health and substance use disorders” (NASMHPD and NASADAD 2000).
- Evaluate and Improve. It is essential to evaluate performance. Findings help providers revise protocols to get better results and give them a vital two-way channel for communicating with key stakeholders (NASMHPD and NASADAD 2000).
Figure 3-5
Assessing the Agency’s Potential To Serve Clients With COD
- Describe the profile of current clients with COD and any potential changes anticipated.
- Estimate the prevalence of persons with COD among the agency’s clients. (One of the screening tools recommended in chapter 4 may be appropriate for this purpose.)
- What are the demographics of persons with COD?
- What functional problems do they have?
- Are there clients with COD who seek care at the agency who are referred elsewhere? What is the profile of these clients?
- Identify services needed by clients.
- What services are needed by existing and potential clients?
- Identify and assess resources available to meet client needs.
- What services are immediately available to the program?
- What services could be added within the program?
- What services are available from the community that would enhance care?
- How well are outside agencies meeting clients’ needs?
- Assess resource gaps.
- What resources are needed to enhance treatment for persons with COD?
- What can your agency, specifically, do to enhance its capacity to serve these clients?
- Assess capacity.
- Realistically assess the capacity of your agency to address these resource gaps.
- Develop a plan to enhance capacity to treat clients with COD.
- How can the skills of existing staff be increased?
- Can additional expertise be accessed through consulting agreements or similar arrangements?
- What additional programs or services can be offered?
- What sources of funding might support efforts to enhance capacity?
Figure 3-6
Financing a Comprehensive System of Care for People With COD
Key System Development Components
- Provide Leadership/Build Consensus
- Identify Resources
- Develop New Models/Train Staff
- Decide on Outcomes
- Evaluate Program
Financing Principles
- Plan To Purchase Together
- Define the Population
- Secure Financing
- Purchase Effective Services
- Purchase Performance
- Evaluate and Improve
Source: NASMHPD and NASADAD 2000, p. 19.
Federal funding opportunities
Federal funding opportunities include a variety of grants from diverse agencies. In its efforts to enhance services, the Substance Abuse and Mental Health Services Administration (SAMHSA) is currently emphasizing the use of strategies that have been demonstrated to be effective in research (“science to service”).
Other Federal agencies such as the National Institutes of Health (NIH), including the National Institute on Drug Abuse (NIDA) and the National Institute on Alcohol Abuse and Alcoholism (NIAAA), and the National Institute of Mental Health (NIMH), emphasize funds for research and likely will provide only modest funds for treatment—typically in conjunction with research projects. Overall, SAMHSA will focus on working with States and helping communities use the latest research findings to implement effective treatment and prevention programs, while NIH institutes will conduct research on best practices in substance abuse treatment, prevention, and mental health services. The reader can determine what funding opportunities are currently available by visiting funder Web sites (e.g., SAMHSA’s Web site at http://www.samhsa.gov, NIDA’s Web site at http://www.nida.nih.gov, NIAAA’s Web site at http://www.niaaa.nih.gov, and NIMH’s Web site at http://www.nimh.nih.gov).
Although SAMHSA and NIH probably will remain the main Federal funding sources for initiatives related to people with COD, other Federal agencies also may provide funding opportunities. Examples of such Federal agencies include the Health Resources and Services Administration within the U.S. Department of Health and Human Services, the U.S. Department of Justice, the U.S. Department of Labor, and so on. The reader can determine what funding opportunities are currently available by visiting the Web sites of these agencies or by searching the Catalog of Federal Domestic Assistance Web site (http://www.cfda.gov), which provides a database of all Federal programs available to State and local governments (including the District of Columbia); federally recognized Indian tribal governments; Territories (and possessions) of the United States; domestic public, quasi-public, and private profit and nonprofit organizations and institutions; specialized groups; and individuals.
State funding opportunities
Administrators or treatment professionals should be familiar with the funding mechanisms in their State. Information is also available through the National Association of State Alcohol/Drug Abuse Directors (http://www.nasadad.org) and the National Association of State Mental Health Program Directors (http://www.nasmhpd.org).
Private funding opportunities
Foundation matching funds can be used to leverage change within a system in specific areas and increasingly should be explored in the area of COD treatment. For example, Robert Wood Johnson Foundation funding has driven improved access to primary care within addiction services.
A wide variety of funding initiatives exist in health care, including in the area of substance abuse treatment. Eligibility and procedures for getting funding will vary depending on the specific foundation. The best procedure is to use the Web site of the Foundation Center (http://www.foundationcenter.org) to identify a possible funder, then call or write to ask for information on its current funding interests and application procedures. The Web site allows visitors to search profiles of more than 65,000 private and community foundations. The Foundation Center also produces a CD-ROM version of its database and print publications containing information on grants. Among the many foundations that have a broad interest in this field are the Ittleson Foundation, Inc., the van Ameringen Foundation, the Trull Foundation, the Carlisle Foundation, the Mary Owen Border Foundation, and the Chevron Corporation.
For the most part, private funding provides an opportunity to enhance existing larger programs with a specific “add-on” service, such as employment counseling or a substance abuse prevention group for children of people who abuse substances. Programs can be significantly strengthened through the aggressive pursuit of available grants and by combining several funding opportunities. Treatment providers seeking funding should not overlook the possibility that major businesses operating in their geographic area may have charitable foundations that could be tapped for promising program initiatives.
Attaining Equitable Allocation of Resources
It is recognized that the acquisition of adequate program resources is both a challenging and essential task. Moreover, though a number of advances have been made in recent years in the treatment of people with COD, systems of care across the country often have not improved accordingly. For example, while programs are now working to treat COD in an integrated manner, mental health services and substance abuse treatment still are funded separately. This can cause programs to spend significantly increased amounts of time in administrative tasks needed to acquire funds for a client’s treatment through multiple streams. Also, payors in many places continue to fund treatment using an acute care model, even though treatment providers recognize that clients can present with long-term disorders.
In addition to the amount of money spent on COD, it is important to address issues of efficiency. One study of the expenditures on COD found that annual spending per client with COD in 1997 was $5,000 to $11,000 (depending on the State), which is nearly twice as high as clients with mental disorders only and nearly four times as high as clients with substance use disorders only.
Clients with COD compared to clients with a single diagnosis receive more treatment services of the major types—hospital inpatient, residential, and outpatient services. While clients with COD do not remain in the hospital as long as clients with mental disorders only, they do stay longer in residential treatment than clients with single diagnoses.
Clients with COD have higher outpatient expenses. Those expenses are 40 to over 100 percent higher than those of clients with mental disorders only, and 200 to over 300 percent higher than those of clients with substance use disorders only. The average amount spent for outpatient treatment is $2,700 to $4,600 per client with COD.
In addressing COD, it is also important to look at medication costs when addressing the issue of equitable allocation of resources. In the three States reviewed, the estimated costs for those with mental disorders only and with COD was about $400 to $600 per person per year. However, clients with substance use disorders only generally do not get prescription medication therapy; their medication spending range was $100 to $200.
To be effective, resources must be used to implement the evidence-based practices most appropriate to the client population and the program needs.
When looking at the existing allocation of resources for clients with COD and the demographics of covered clients, the three-State estimated study found that they are more likely to be adults over the age of 18 and are more likely to be male, but less likely to be minorities,than are clients with single diagnoses.They are also more likely to be the exclusive responsibility of mental health or substance abuse agencies rather than Medicaid’s total responsibility; across the three States, 40 to 84 percent of clients with COD receive services only from mental health or substance abuse agencies.
The Expenditures on Treatment of Co-Occurring Mental and Substance Use Disorders reference study involved only three States: Delaware, Oklahoma, and Washington. However, the data presented raise the issue of efficiency and effectiveness rather than cost. For those with more serious mental illness, strategies that are more efficient may make the better use of the larger amounts spent on those with COD, rather than creating disturbances in the existing system by forcing the shifting of resources from the treatment of those with either substance use disorders or mental disorders only.
Ultimately, we are challenged not only to advocate on behalf of our own programs and clients, but for systemic change. Effective advocacy will help ensure that resources are allocated in a manner that takes appropriate cognizance of the needs of our clients and the complexity of the treatment field for clients with COD. However, in any advocacy caution against unintended consequences must be taken; with the deinstitutionalization of patients hospitalized for severe and persistent mental illnesses, the expected reallocation of funds did not occur as expected.
Any savings that could come from integrated treatment must not be diverted into general revenues. Any efficiencies that result from more effective treatment of those without COD, but with mental disorders or substance use disorders alone, should be invested into integrated treatment. Any transformation of the existing system of care that results in a decrease in access to substance abuse treatment for those without COD will only create stresses in the criminal justice, workplace, and child welfare systems.
Integrating Research and Practice
To be effective, resources must be used to implement the evidence-based practices most appropriate to the client population and the program needs. The importance of the transfer of knowledge and technology has come to be well understood. Conferences to explore “bridging the gap” between research and field practice are now common.
Although not specific to COD, these efforts have clear implications for our attempts to share knowledge of what is working for clients with COD. As emphasized in the 1998 report by Lamb and colleagues, Bridging the Gap Between Research and Practice, there is a need for, and value in, “enhancing collaborative relationships between the drug abuse research community and the world of community-based treatment programs” (Lamb et al. 1998, p. v). Brown (1998) has underscored the fundamental importance of making research relevant to practice, emphasizing the need for new government initiatives that focus on interpersonal contacts to achieve organizational change and that promote technology transfer as a significant area of investigation.
Several recent government initiatives highlight this effort and are described in Changing the Conversation (CSAT 2000a). They include
- Practice Improvement Collaboratives (SAMHSA/CSAT)
- Clinical Trials Network Program (NIH/NIDA)
- Improving the Delivery of Alcohol Treatment and Prevention Services (NIH/NIAAA)
- Evidence-based Practice Centers (Agency for Healthcare Research and Quality)
- The Addiction Technology Transfer Centers (SAMHSA/CSAT)
- The Knowledge Application Program (SAMHSA/CSAT)
- Researcher in Residence Program (NIH/NIAAA)
CSAT’s Practice Improvement Collaboratives
Knowledge exchange is one of the most critical elements in efforts to move best practices in substance abuse treatment to community programs working on the front lines of substance abuse interventions. Formerly known as the Practice/Research Collaboratives, the Practice Improvement Collaboratives program—designed, in part, to achieve this goal—supports the development of collaborations among a broad spectrum of substance abuse treatment organizations (including, but not limited to, community-based treatment organizations, units of government, colleges, universities, and other public research entities). Key objectives of the program include the following:
- To develop and sustain community involvement in, and commitment to, practice improvement in the delivery of substance abuse treatment services.
- To improve the quality of substance abuse treatment through the adoption of evidence-based practices in community-based treatment organizations.
- To identify successful methods and models for implementing evidence-based practices in community-based treatment organizations.
Workforce Development and Staff Support
This section focuses on some key issues providers face in developing a workforce able to meet the needs of clients with COD. These include
- The attitudes and values providers must have to work successfully with these clients
- Essential competencies for clinicians (basic, intermediate, and advanced)
- Opportunities for continuing professional development
- Ways to avoid burnout and reduce turnover—common problems for any substance abuse treatment provider, but particularly so for those who work with clients who have COD
The consensus panel underscores the importance of an investment in creating a supportive environment for staff that encourages professional development to include skill acquisition, values clarification, training, and competency attainment equal to an investment in new COD program development. An organizational commitment to both is necessary for successful implementation of programs. Examples of staff support may include standards of practice related to consistent high-quality supervision, favorable tuition reimbursement and release time policies, helpful personnel policies related to bolstering staff wellness practices, and incentives or rewards for work-related achievement, etc. Together these elements help in the creation of needed infrastructure for quality of service.
Attitudes and Values
Attitudes and values guide the way providers meet client needs and affect the overall treatment climate. They not only determine how the client is viewed by the provider (thereby generating assumptions that could either facilitate or deter achievement of the highest standard of care), but also profoundly influence how the client feels as he or she experiences a program. Attitudes and values are particularly important in working with clients with COD since the counselor is confronted with two disorders that require complex interventions.
The essential attitudes and values for working with clients with COD shown in Figure 3-7 are adapted from Technical Assistance Publication 21, Addiction Counseling Competencies: The Knowledge, Skills, and Attitudes of Professional Practice (Center for Substance Abuse Treatment 1998a). The consensus panel believes these attitudes and values also are consistent with the attitudes and values of the vast majority of those who commit themselves to the challenging fields of substance abuse treatment and mental health services.
Clinicians’ Competencies
Clinicians’ competencies are the specific and measurable skills that counselors must possess. Several States, university programs, and expert committees have defined the key competencies for working with clients with COD. Typically, these competencies are developed by training mental health and substance abuse treatment counselors together, often using a case-based approach that allows trainees to experience the insights each field affords the other.
One challenge of training is to include culturally sensitive methods and materials that reflect consideration for the varying levels of expertise and background of participants. The consensus panel recommends viewing competencies as basic, intermediate, and advanced to foster continuing professional development of all counselors and clinicians in the field of COD. This classification does not crosswalk with the program classification system using the same terminology illustrated in Figure 3-2 (p. 44) and is derived from various sources. Clearly, the sample competencies listed within each category cannot be completely separated from each other (e.g., competencies in the “basic” category may require some competency in the “intermediate” category). Some of the categorizations may be debatable, but the grouping within each category reflects, on the whole, different levels of clinician competency.
Providers in the field face unusual challenges and often provide effective treatment while working within their established frameworks. In fact, research studies previously cited have established the effectiveness of substance abuse treatment approaches in working with persons who have low- to moderate-severity mental disorders. Still, the classification of competencies supports continued professional development and promotes training opportunities.
Basic competencies
Every substance abuse treatment and mental health service program should require counselors to have certain basic skills. In keeping with the principle that there is “no wrong door,” the consensus panel recommends that clinicians working in substance abuse treatment settings should be able to carry out the mental-health–related activities shown in Figure 3-8 (p. 58).
Figure 3-7
Essential Attitudes and Values for Clinicians Who Work With Clients Who Have COD
- Desire and willingness to work with people who have COD
- Appreciation of the complexity of COD
- Openness to new information
- Awareness of personal reactions and feelings
- Recognition of the limitations of one’s own personal knowledge and expertise
- Recognition of the value of client input into treatment goals and receptivity to client feedback
- Patience, perseverance, and therapeutic optimism
- Ability to employ diverse theories, concepts, models, and methods
- Flexibility of approach
- Cultural competence
- Belief that all individuals have strengths and are capable of growth and development (added by consensus panel)
- Recognition of the rights of clients with COD, including the right and need to understand assessment results and the treatment plan
Intermediate competencies
Intermediate competencies encompass skills in engaging substance abuse treatment clients with COD, screening, obtaining and using mental health assessment data, treatment planning, discharge planning, mental health system linkage, supporting medication, running basic mental disorder education groups, and implementing routine and emergent mental health referral procedures. In a mental health unit, mental health providers would exhibit similar competencies related to substance use disorders. The consensus panel recommends the intermediate level competencies shown in Figure 3-9 (p. 59), developed jointly by the New York State Office of Mental Health and the New York State Office of Alcohol and Substance Abuse Services.
Advanced competencies
At the advanced level, the practitioner goes beyond an awareness of the addiction and mental health fields as individual disciplines to a more sophisticated appreciation for how cooccurring disorders interact in an individual. This enhanced awareness leads to an improved ability to provide appropriate integrated treatment. Figure 3-10 (p. 60) gives examples of advanced skills.
Continuing Professional Development
The consensus panel is aware that many providers in the substance abuse treatment and mental health services fields have performed effectively the difficult task of providing services for clients with COD, until recently without much guidance from an existing body of knowledge or available systematic approaches. The landscape has changed and a solid knowledge base is now available to the counselor, although that knowledge typically is scattered through many journals and reports. This TIP makes an effort to integrate the available information. Counselors reading this TIP can review their own knowledge and determine what they need to continue their professional development.
At the time of this writing, Arizona, Connecticut, Illinois, New Mexico, New York, and Pennsylvania have developed consensus guidelines that define the competencies substance abuse treatment counselors should have to claim expertise in this area. Others are in the process of identifying mechanisms for licensing or certifying expertise in COD. Counselors may check with their States’ certification bodies to determine whether training leading to formal credentials in counseling persons with co-occurring disorders is available. Appendix I identifies some resources counselors can use to enhance their professional knowledge and development.
Figure 3-8
Examples of Basic Competencies Needed for Treatment of Persons With COD
- Perform a basic screening to determine whether COD might exist and be able to refer the client for a formal diagnostic assessment by someone trained to do this.
- Form a preliminary impression of the nature of the disorder a client may have, which can be verified by someone formally trained and licensed in mental health diagnosis.
- Conduct a preliminary screening of whether a client poses an immediate danger to self or others and coordinate any subsequent assessment with appropriate staff and/or consultants.
- Be able to engage the client in such a way as to enhance and facilitate future interaction.
- De-escalate the emotional state of a client who is agitated, anxious, angry, or in another vulnerable emotional state.
- Manage a crisis involving a client with COD, including a threat of suicide or harm to others. This may involve seeking out assistance by others trained to handle certain aspects of such crises; for example, processing commitment papers and related matters.
- Refer a client to the appropriate mental health or substance abuse treatment facility and follow up to ensure the client receives needed care.
- Coordinate care with a mental health counselor serving the same client to ensure that the interaction of the client’s disorders is well understood and that treatment plans are coordinated.
Education and training
Discipline-specific education
Staff education and training are fundamental to all substance abuse treatment programs. Although there have been improvements in the past decade, there are still very few university-based programs that offer a formal curriculum on COD. Numerous observers have commented on the lack of adequate discipline-based training for professionals in the substance abuse treatment field (Brown 1996; Galanter 1989; Miller and Brown 1997).
Many professional organizations are promoting the development of competencies and practice standards for intervening with substance abuse problems, including the Council on Addictions of the American Psychiatric Association; the American Academy of Addiction Psychiatry; the American Osteopathic Academy of Addiction Medicine; American Psychological Association; the American Society of Addiction Medicine; the Association for Medical Education and Research on Substance Abuse; the American Association of Obstetricians and Gynecologists; the Alcohol, Tobacco and Other Addictions Section of the National Association of Social Workers; and the International Nurses Society on Addictions. They are also specifically encouraging faculty members to enhance their knowledge in this area so they can better prepare their students to meet the needs of clients with COD. The consensus panel encourages all such organizations to identify standards and competencies for their membership related to COD and to encourage the development of training for specific disciplines.
Since the consequences of both addiction and mental disorders can present with physical or psychiatric manifestations, it is equally important for medical students, internal medicine and general practice residents, and general psychiatry residents to be educated in the problems of COD. Too few hours of medical education are devoted to the problems of addiction and mental disorders. Since pharmacologic therapies play a critical role in the treatment of those with COD, it is important to have adequately trained physicians who can manage the medication therapies for those clients.
Figure 3-9
Six Areas of Intermediate-Level Competencies Needed for the Treatment of Persons With COD
- Competency I: Integrated Diagnosis of Substance Abuse and Mental Disorders. Differential diagnosis, terminology (definitions), pharmacology, laboratory tests and physical examination, withdrawal symptoms, cultural factors, effects of trauma on symptoms, staff self-awareness
- Competency II: Integrated Assessment of Treatment Needs. Severity assessment, lethality/risk, assessment of motivation/readiness for treatment, appropriateness/treatment selection
- Competency III: Integrated Treatment Planning. Goal-setting/problemsolving, treatment planning, documentation, confidentiality[1], legal/reporting issues, documenting issues for managed care providers
- Competency IV: Engagement and Education. Staff self-awareness, engagement, motivating, educating
- Competency V: Early Integrated Treatment Methods. Emergency/crisis intervention, knowledge and access to treatment services, when and how to refer or communicate
- Competency VI: Longer Term Integrated Treatment Methods. Group treatment, relapse prevention, case management, pharmacotherapy, alternatives/risk education, ethics, confidentiality[2], mental health, reporting requirements, family interventions
Continuing education and training
Many substance abuse treatment counselors learn through continuing education and facility-sponsored training. Continuing education and training involves participation in a variety of courses and workshops from basic to advanced level offered by a number of training entities (see appendix I). The strength of continuing education and training courses and workshops is that they provide the counselor with the opportunity to review and process written material with a qualified instructor and other practitioners.
Continuing education is useful because it can respond rapidly to the needs of a workforce that has diverse educational backgrounds and experience. To have practical utility, competency training must address the day-to-day issues that counselors face in working with clients with COD. The educational context must be rich with information, culturally sensitive, designed for adult students, and must include examples and role models. It is optimal if the instructors have extensive experience as practitioners in the field. Figure 3-11 (p. 61) provides an example description for one of many possible continuing education courses in this dynamic field.
Continuing education is essential for effective provision of services to people with COD, but it is not sufficient in and of itself. Counselors must have ongoing support, supervision, and opportunity to practice new skills if they are to truly integrate COD content into their practice.
Figure 3-10
Examples of Advanced Competencies in the Treatment of Clients With COD
- Use the current edition of criteria from the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (American Psychiatric Association 2000) to assess substance-related disorders and Axis I and Axis II mental disorders.
- Comprehend the effects of level of functioning and degree of disability related to both substance-related and mental disorders, separately and combined.
- Recognize the classes of psychotropic medications, their actions, medical risks, side effects, and possible interactions with other substances.
- Use integrated models of assessment, intervention, and recovery for persons having both substance-related and mental disorders, as opposed to parallel treatment efforts that resist integration.
- Apply knowledge that relapse is not considered a client failure but an opportunity for additional learning for all. Treat relapses seriously and explore ways of improving treatment to decrease relapse frequency and duration.
- Display patience, persistence, and optimism.
- Collaboratively develop and implement an integrated treatment plan based on thorough assessment that addresses both/all disorders and establishes sequenced goals based on urgent needs, considering the stage of recovery and level of engagement.
- Involve the person, family members, and other supports and service providers (including peer supports and those in the natural support system) in establishing, monitoring, and refining the current treatment plan.
- Support quality improvement efforts, including, but not limited to consumer and family satisfaction surveys, accurate reporting and use of outcome data, participation in the selection and use of quality monitoring instruments, and attention to the need for all staff to behave respectfully and collaboratively at all times.
Source: Adapted from Minkoff 1999.
Cross-training
Cross-training is the simultaneous provision of material and training to more than one discipline at a time (e.g., substance abuse and social work counselors; substance abuse counselors and corrections officers). Counselors who have primary expertise in either substance abuse or mental health will be able to work far more effectively with clients who have COD if they have some degree of cross-training in the other field. The consensus panel recommends that counselors of either field receive at least basic level cross-training in the other field to better assess, refer, understand, and work effectively with the large number of clients with COD. Cross-trained individuals who know their primary field of training well, and also have an appreciation for the other field, provide a richness of capacity that cannot be attained using any combination of personnel familiar with one system alone.
When training is offered in this manner, interaction and communication between the counselors from each discipline is facilitated. This helps to remove barriers, increase understanding, and promote integrated work. Cross-training is particularly valuable for staff members who will work together in the same program. Consensus panel members have found cross-training very valuable in mental health, substance abuse, and criminal justice settings.
Program orientation and ongoing supervision
Orientation. Staff education and training have two additional components: (1) a statement of program orientation that clearly presents the mission, values, and aims of service delivery, and (2) strong, ongoing supervision. The orientation can use evidence-based initiatives as well as promising practices. Successful program orientation for working with clients with COD will equip staff members with skills and decisionmaking tools that will enable them to provide optimal services in real-world environments.
Supervision. Many agree that relational skills are requisite for staff working in COD programs (Gerber and Basham 1999; Martino et al. 2000; Miller 2000b), skills that are best learned though direct supervision. Active listening, interviewing techniques, the ability to summarize, and the capacity to provide feedback are all skills that can be best modeled by a supervisor. Strong, active supervision of ongoing cases is a key element in assisting staff to develop, maintain, and enhance relational skills.
National training resources
Training resources. Curricula and other forms of educational materials are available through Addiction Technology Transfer Centers (ATTCs), universities, State entities, and private consultants. These materials can help enhance the ability of substance abuse treatment counselors to work with clients who have mental disorders, as well as to enable mental health personnel to improve their efforts with persons with substance use disorders. ATTCs offer workshops, courses, and online remote location courses. (See appendix I for training sources.)
Figure 3-11
Treatment Planning and Documentation Issues for Mental and Substance Use Disorders
Description
This course provides an opportunity for participants to review the principles of collaborative treatment planning, including working from a comprehensive assessment; identifying and mutually setting long- and short-term goals; identifying steps for accomplishing goals, the persons responsible for collaborative treatment planning, and a defined timeline; and reviewing and altering such plans when necessary. Progress tracking is reviewed, including how to write clear and concise notes, and the principles for their review. This course focuses on effective treatment principles and the practices of writing and reviewing plans.
Course Objectives
By the end of this course, participants will be able to
- Review the principles and processes that support thorough and accurate assessment and diagnosis, including strengths-based interviewing skills and cultural diversity issues.
- Examine each step in treatment/service planning, its rationale, and the similarities and differences in service and treatment planning.
- Describe the importance of the person with COD having active involvement and real choice in all post-acute treatment planning processes (and some means for incorporating these features in acute care settings).
- Identify means of writing brief and useful progress notes that support movement toward positive outcomes.
- Discuss means of using progress notes with the person as a useful piece of the ongoing treatment/service process.
Source: Supplied by consensus panelist Donna McNelis, Ph.D.
Listservs and discussion lists. There are a number of e-mail listservs and Internet discussion groups on the topic of COD (e.g., Co-Occurring Dialogues, The Dual Diagnosis Listserv, The Dual Diagnosis Bulletin Board, The Dual Diagnosis Pages: Colleagues List, and MIDAS: A Discussion Group). These online communication networks offer members the opportunity to post suggestions or questions to a large number of people at the same time. Listservs are generally geared more toward professionals and are more closely monitored. Discussion groups usually are open to anyone, and may not be monitored closely. (See appendix I for more detailed descriptions of the listservs and discussion groups mentioned above.)
COD certification in health disciplines
The disciplines of medicine and psychology have recognized subspecialties in COD with a defined process for achieving a certificate in this area. Figure 3-12 summarizes current information on certification by discipline.
Avoiding Burnout and Reducing Staff Turnover
Burnout
Often, substance abuse and mental health clinicians are expected to manage growing and more complex caseloads. “Compassion fatigue” may occur when the pressures of work erode a counselor’s spirit and outlook and begin to interfere with the counselor’s personal life (see TIP 36, Substance Abuse Treatment for Persons With Child Abuse and Neglect Issues [CSAT 2000d], p. 64.) Assisting clients who have COD is difficult and emotionally taxing; the danger of burnout is considerable. It is especially important that program administrators maintain awareness of the problem of burnout and the benefits of reducing turnover. It is vital that staff feel that program administrators are interested in their well-being in order to sustain morale and esprit de corps.
To lessen the possibility of burnout when working with a demanding caseload that includes clients with COD, the consensus panelists for TIP 36, Substance Abuse Treatment for Persons With Child Abuse and Neglect Issues (CSAT 2000d, p. 64) suggest that program directors and supervisors assist counselors to
- Work within a team structure rather than in isolation.
- Build in opportunities to discuss feelings and issues with other staff who handle similar cases.
- Develop and use a healthy support network.
- Maintain the caseload at a manageable size.
- Incorporate time to rest and relax.
- Separate personal and professional time.
Most important, supervision should be supportive, providing guidance and technical knowledge.
Farmer (1995) found that much of the perceived stress among substance abuse treatment counselors was attributable to workload factors and factors relating to management— for example, authoritarian and controlling management styles that allow staff too little autonomy and command over their own work. Performance goals should be realistic and clearly understood. Supervision should be not only a means of ensuring standards of practice, but also a way of encouraging and enabling professional growth.
Grosch and Olsen (1994) suggest that when professionals begin to exhibit signs of boredom or malaise, varying the nature of the job is a helpful strategy. This can be accomplished via a negotiated dialog with the supervisor that is initiated by a staff member who requests an opportunity to try new or differing activities.
Some programs have proactively addressed the issue of burnout among staff to help staff morale, improve care, and reduce turnover in their program. Pavillon International, an addiction treatment residential program in North Carolina, proactively addresses burnout by placing high values on staff well-being; routinely discussing well-being issues; providing activities such as retreats, weekend activities, yoga, and other healing activities at the work site; and creating a network of ongoing support.
Turnover
The issue of staff turnover is especially important for staff working with clients with COD because of the limited workforce pool and the high investment of time and effort involved in developing a trained workforce. It matters, too, because of the crucial importance of the treatment relationship to successful outcomes. Rapid turnover disrupts the context in which recovery occurs. Clients in such agencies may become discouraged about the possibility of being helped by others.
Turnover sometimes results from the unique professional and emotional demands of working with clients with COD. On the other hand, most providers in this area are unusually dedicated and find the work to be rewarding. Figure 3-13 (p. 64) provides some methods for reducing staff turnover.
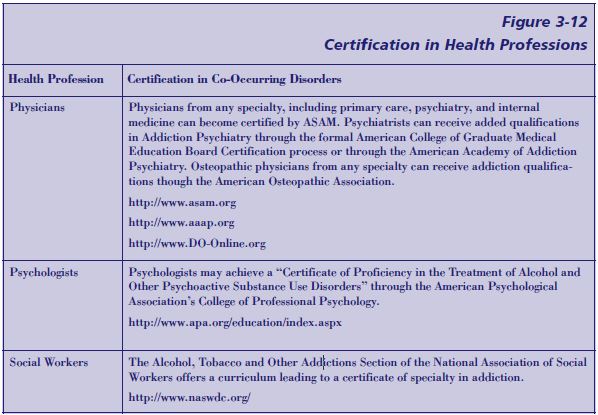
Conclusion: Workforce Development
In concluding this section on workforce development, the consensus panel strongly encourages counselors to acquire the competencies needed to work effectively with clients who have COD. The difficulty of juggling a high and demanding workload and the desire for continued professional development should be recognized and accommodated. To the extent possible, education and training efforts should be customized—in terms of content, schedule, and location—to meet the needs of the counselors in the field. That is, bring the training to the counselor. Agency and program administrators, including both line-level and clinical supervisors, are urged to demonstrate support and encouragement for the continuing education and training of the workforce, as well as develop COD competencies themselves.
Rewards can include both salary and advancement tied to the counselor’s efforts to increase his or her effectiveness in serving clients with COD, as demonstrated by job performance. Naturally, non-counselor clinicians working in primary care settings, community mental health centers, or private mental health offices also should enhance their knowledge of alcohol and drug use in clients with mental health issues.
Figure 3-13
Reducing Staff Turnover in Programs for Clients With COD
To decrease staff turnover, whenever possible, programs should
- Hire staff members who have familiarity with both substance abuse and mental disorders and have a positive regard for clients with either disorder.
- Hire staff members who are critically minded and can think independently, but who are also willing to ask questions and listen, remain open to new ideas, maintain flexibility, work cooperatively, and engage in creative problemsolving.
- Provide staff with a framework of realistic expectations for the progress of clients with COD.
- Provide opportunities for consultation among staff members who share the same client (including medication providers).
- Ensure that supervisory staff members are supportive and knowledgeable about issues specific to clients with COD.
- Provide and support opportunities for further education and training.
- Provide structured opportunities for staff feedback in the areas of program design and implementation.
- Promote sophistication about, and advocacy for, COD issues among administrative staff, including both those in decisionmaking positions (e.g., the director and clinical director) and others (e.g., financial officers, billing personnel, and State reporting monitors).
- Provide a desirable work environment through adequate compensation, salary incentives for COD expertise, opportunities for training and for career advancement, involvement in quality improvement or clinical research activities, and efforts to adjust workloads.
- Confidentiality is governed by the Federal “Confidentiality of Alcohol and Drug Abuse Patient Records” regulations (42 C.F.R. Part 2) and the Federal “Standards for Privacy of Individually Identifiable Health Information” (45 C.F.R. Parts 160 and 164). ↵
- Confidentiality is governed by the Federal “Confidentiality of Alcohol and Drug Abuse Patient Records” regulations (42 C.F.R. Part 2) and the Federal “Standards for Privacy of Individually Identifiable Health Information” (45 C.F.R. Parts 160 and 164). ↵