
7: Joints
- Page ID
- 12527
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Introduction
The adult human body has 206 bones, and with the exception of the hyoid bone in the neck, each bone is connected to at least one other bone. Joints are the location where bones come together. Many joints allow for movement between the bones. At these joints, the articulating surfaces of the adjacent bones can move smoothly against each other. However, the bones of other joints may be joined to each other by connective tissue or cartilage. These joints are designed for stability and provide for little or no movement. Importantly, joint stability and movement are related to each other. This means that stable joints allow for little or no mobility between the adjacent bones. Conversely, joints that provide the most movement between bones are the least stable.
Understanding the relationship between joint structure and function will help to explain why particular types of joints are found in certain areas of the body.
The articulating surfaces of bones at stable types of joints, with little or no mobility, are strongly united to each other. For example, most of the joints of the skull are held together by fibrous connective tissue and do not allow for movement between the adjacent bones. This lack of mobility is important, because the skull bones serve to protect the brain. Similarly, other joints united by fibrous connective tissue allow for very little movement, which provides stability and weight-bearing support for the body. For example, the tibia and fibula of the leg are tightly united to give stability to the body when standing. At other joints, the bones are held together by cartilage, which permits limited movements between the bones. Thus, the joints of the vertebral column only allow for small movements between adjacent vertebrae, but when added together, these movements provide the flexibility that allows your body to twist, or bend to the front, back, or side. In contrast, at joints that allow for wide ranges of motion, the articulating surfaces of the bones are not directly united to each other. Instead, these surfaces are enclosed within a space filled with lubricating fluid, which allows the bones to move smoothly against each other. These joints provide greater mobility, but since the bones are free to move in relation to each other, the joint is less stable. Most of the joints between the bones of the appendicular skeleton are this freely moveable type of joint. These joints allow the muscles of the body to pull on a bone and thereby produce movement of that body region. Your ability to kick a soccer ball, pick up a fork, and dance the tango depend on mobility at these types of joints.
Knee Joint
The knee joint is the largest joint of the body (Figure 7.1). It actually consists of three articulations. The femoropatellar joint is found between the patella and the distal femur. The medial tibiofemoral joint and lateral tibiofemoral joint are located between the medial and lateral condyles of the femur and the medial and lateral condyles of the tibia. All of these articulations are enclosed within a single articular capsule. The knee functions as a hinge joint, allowing flexion and extension of the leg. This action is generated by both rolling and gliding motions of the femur on the tibia. In addition, some rotation of the leg is available when the knee is flexed, but not when extended. The knee is well constructed for weight bearing in its extended position, but is vulnerable to injuries associated with hyperextension, twisting, or blows to the medial or lateral side of the joint, particularly while weight bearing.
At the femoropatellar joint, the patella slides vertically within a groove on the distal femur. The patella is a sesamoid bone incorporated into the tendon of the quadriceps femoris muscle, the large muscle of the anterior thigh. The patella serves to protect the quadriceps tendon from friction against the distal femur. Continuing from the patella to the anterior tibia just below the knee is the patellar ligament. Acting via the patella and patellar ligament, the quadriceps femoris is a powerful muscle that acts to extend the leg at the knee. It also serves as a “dynamic ligament” to provide very important support and stabilization for the knee joint.
The medial and lateral tibiofemoral joints are the articulations between the rounded condyles of the femur and the relatively flat condyles of the tibia. During flexion and extension motions, the condyles of the femur both roll and glide over the surfaces of the tibia. The rolling action produces flexion or extension, while the gliding action serves to maintain the femoral condyles centered over the tibial condyles, thus ensuring maximal bony, weight-bearing support for the femur in all knee positions. As the knee comes into full extension, the femur undergoes a slight medial rotation in relation to tibia. The rotation results because the lateral condyle of the femur is slightly smaller
than the medial condyle. Thus, the lateral condyle finishes its rolling motion first, followed by the medial condyle. The resulting small medial rotation of the femur serves to “lock” the knee into its fully extended and most stable position. Flexion of the knee is initiated by a slight lateral rotation of the femur on the tibia, which “unlocks” the knee. This lateral rotation motion is produced by the popliteus muscle of the posterior leg.
Located between the articulating surfaces of the femur and tibia are two articular discs, the medial meniscus and lateral meniscus (see Figure 7.1b). Each is a C-shaped fibrocartilage structure that is thin along its inside margin and thick along the outer margin. They are attached to their tibial condyles, but do not attach to the femur. While both menisci are free to move during knee motions, the medial meniscus shows less movement because it is anchored at its outer margin to the articular capsule and tibial collateral ligament. The menisci provide padding between the bones and help to fill the gap between the round femoral condyles and flattened tibial condyles.
Some areas of each meniscus lack an arterial blood supply and thus these areas heal poorly if damaged.
The knee joint has multiple ligaments that provide support, particularly in the extended position (see Figure 7.1c). Outside of the articular capsule, located at the sides of the knee, are two extrinsic ligaments. The fibular collateral ligament (lateral collateral ligament) is on the lateral side and spans from the lateral epicondyle of the femur to the head of the fibula. The tibial collateral ligament (medial collateral ligament) of the medial knee runs from the medial epicondyle of the femur to the medial tibia. As it crosses the knee, the tibial collateral ligament is firmly attached on its deep side to the articular capsule and to the medial meniscus, an important factor when considering knee injuries. In the fully extended knee position, both collateral ligaments are taut (tight), thus serving to stabilize and support the extended knee and preventing side-to-side or rotational motions between the femur and tibia.
The articular capsule of the posterior knee is thickened by intrinsic ligaments that help to resist knee hyperextension. Inside the knee are two intracapsular ligaments, the anterior cruciate ligament and posterior cruciate ligament. These ligaments are anchored inferiorly to the tibia at the intercondylar eminence, the roughened area between the tibial condyles. The cruciate ligaments are named for whether they are attached anteriorly or posteriorly to this tibial region. Each ligament runs diagonally upward to attach to the inner aspect of a femoral condyle. The cruciate ligaments are named for the X-shape formed as they pass each other (cruciate means “cross”). The posterior cruciate ligament is the stronger ligament. It serves to support the knee when it is flexed and weight bearing, as when walking downhill. In this position, the posterior cruciate ligament prevents the femur from sliding anteriorly off the top of the tibia. The anterior cruciate ligament becomes tight when the knee is extended, and thus resists hyperextension.
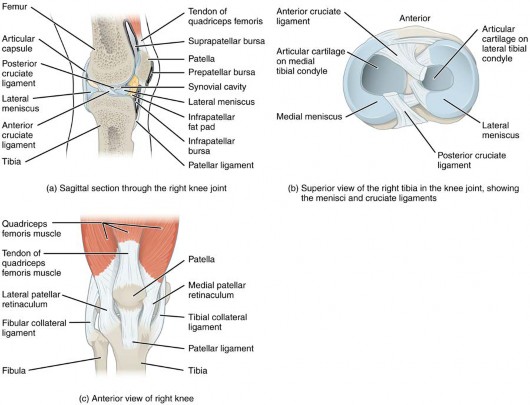
Figure 7.1 Knee Joint (a) The knee joint is the largest joint of the body. (b)–(c) It is supported by the tibial and fibular collateral ligaments located on the sides of the knee outside of the articular capsule, and the anterior and posterior cruciate ligaments found inside the capsule. The medial and lateral menisci provide padding and support between the femoral condyles and tibial condyles.
Elbow Joint
The elbow joint is a uniaxial hinge joint formed by the humeroulnar joint, the articulation between the trochlea of the humerus and the trochlear notch of the ulna. Also associated with the elbow are the humeroradial joint and the proximal radioulnar joint. All three of these joints are enclosed within a single articular capsule (Figure 7.2).
The articular capsule of the elbow is thin on its anterior and posterior aspects, but is thickened along its outside margins by strong intrinsic ligaments. These ligaments prevent side-to-side movements and hyperextension. On the medial side is the triangular ulnar collateral ligament. This arises from the medial epicondyle of the humerus and attaches to the medial side of the proximal ulna. The strongest part of this ligament is the anterior portion, which resists hyperextension of the elbow. The ulnar collateral ligament may be injured by frequent, forceful extensions of the forearm, as is seen in baseball pitchers. Reconstructive surgical repair of this ligament is referred to as Tommy John surgery, named for the former major league pitcher who was the first person to have this treatment.
The lateral side of the elbow is supported by the radial collateral ligament. This arises from the lateral epicondyle of the humerus and then blends into the lateral side of the annular ligament. The annular ligament encircles the head of the radius. This ligament supports the head of the radius as it articulates with the radial notch of the ulna at the proximal radioulnar joint. This is a pivot joint that allows for rotation of the radius during supination and pronation of the forearm.
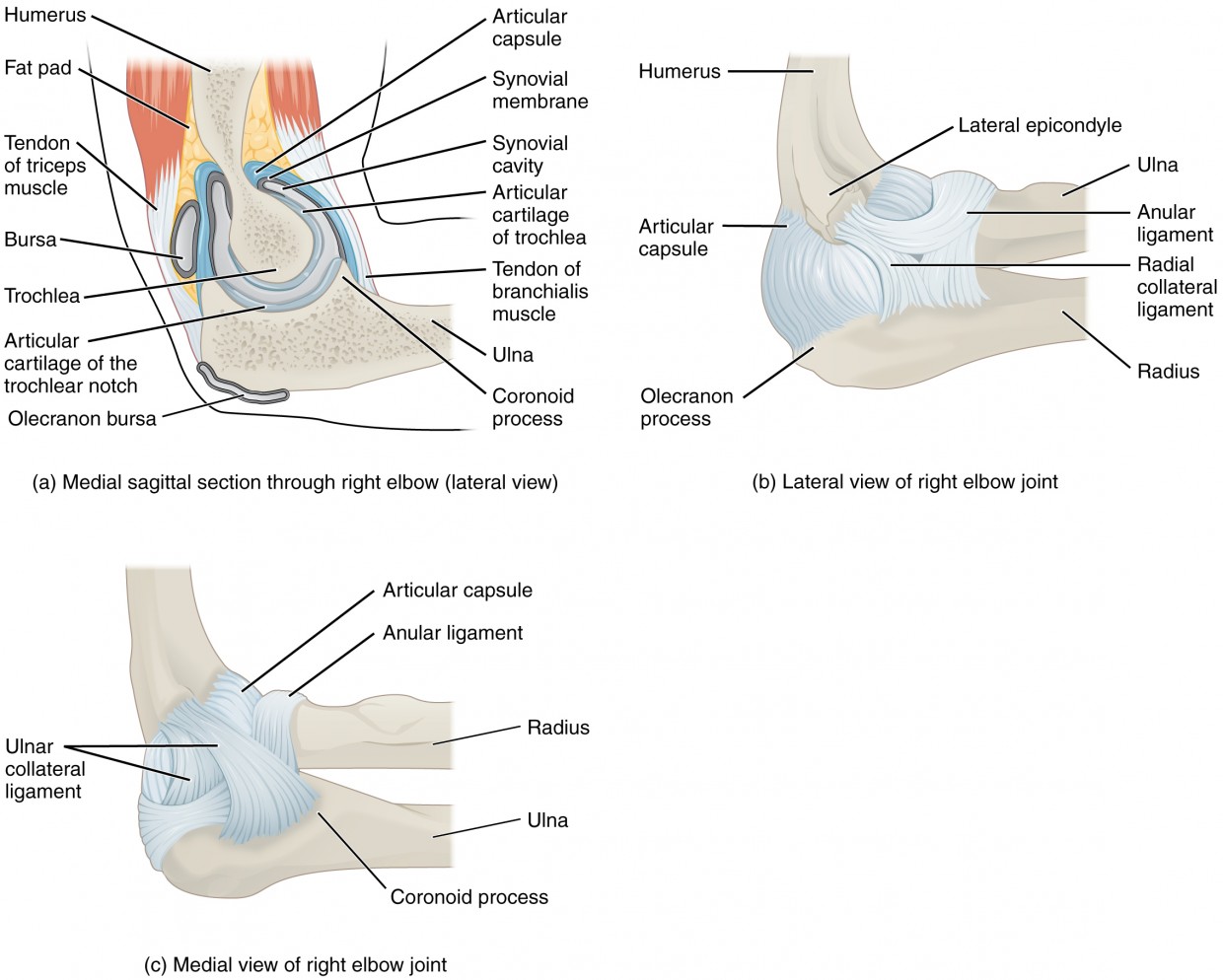
Figure 7.2 Elbow Joint (a) The elbow is a hinge joint that allows only for flexion and extension of the forearm. (b) It is supported by the ulnar and radial collateral ligaments. (c) The annular ligament supports the head of the radius at the proximal radioulnar joint, the pivot joint that allows for rotation of the radius. (CC BY 4.0; OpenStax).
Shoulder Joint
The shoulder joint is called the glenohumeral joint. This is a ball-and-socket joint formed by the articulation between the head of the humerus and the glenoid cavity of the scapula (Figure 7.3). This joint has the largest range of motion of any joint in the body. However, this freedom of movement is due to the lack of structural support and thus the enhanced mobility is offset by a loss of stability.
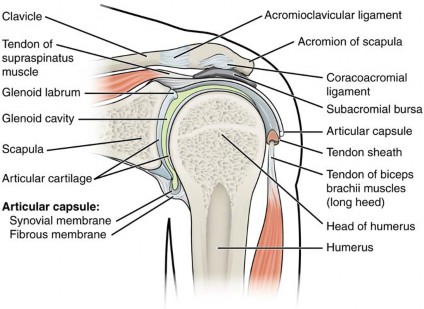
Figure 7.3 Glenohumeral Joint The glenohumeral (shoulder) joint is a ball-and-socket joint that provides the widest range of motions. It has a loose articular capsule and is supported by ligaments and the rotator cuff muscles.
The large range of motions at the shoulder joint is provided by the articulation of the large, rounded humeral head with the small and shallow glenoid cavity, which is only about one third of the size of the humeral head. The socket formed by the glenoid cavity is deepened slightly by a small lip of fibrocartilage called the glenoid labrum, which extends around the outer margin of the cavity. The articular capsule that surrounds the glenohumeral joint is relatively thin and loose to allow for large motions of the upper limb. Some structural support for the joint is provided by thickenings of the articular capsule wall that form weak intrinsic ligaments. These include the coracohumeral ligament, running from the coracoid process of the scapula to the anterior humerus, and three ligaments, each called a glenohumeral ligament, located on the anterior side of the articular capsule. These ligaments help to strengthen the superior and anterior capsule walls.
However, the primary support for the shoulder joint is provided by muscles crossing the joint, particularly the four rotator cuff muscles. These muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) arise from the scapula and attach to the greater or lesser tubercles of the humerus. As these muscles cross the shoulder joint, their tendons encircle the head of the humerus and become fused to the anterior, superior, and posterior walls of the articular capsule. The thickening of the capsule formed by the fusion of these four muscle tendons is called the rotator cuff. Two bursae, the subacromial bursa and the subscapular bursa, help to prevent friction between the rotator cuff muscle tendons and the scapula as these tendons cross the glenohumeral joint. In addition to their individual actions of moving the upper limb, the rotator cuff muscles also serve to hold the head of the humerus in position within the glenoid cavity. By constantly adjusting their strength of contraction to resist forces acting on the shoulder, these muscles serve as “dynamic ligaments” and thus provide the primary structural support for the glenohumeral joint.
Injuries to the shoulder joint are common. Repetitive use of the upper limb, particularly in abduction such as during throwing, swimming, or racquet sports, may lead to acute or chronic inflammation of the bursa or muscle tendons, a tear of the glenoid labrum, or degeneration or tears of the rotator cuff. Because the humeral head is strongly supported by muscles and ligaments around its anterior, superior, and posterior aspects, most dislocations of the humerus occur in an inferior direction. This can occur when force is applied to the humerus when the upper limb is fully abducted, as when diving to catch a baseball and landing on your hand or elbow.
Inflammatory responses to any shoulder injury can lead to the formation of scar tissue between the articular capsule and surrounding structures, thus reducing shoulder mobility, a condition called adhesive capsulitis (“frozen shoulder”)
B
LAB 7 EXERCISES 7-1
A
Match the following: Joint cavity * Articular cartilages * Fibrous capsule * Synovial membrane.
Organize the following types of joints into a diagram or table: Ball & socket * Cartilaginous * Condylar * Fibrous * Hinge * Pivot * Plane * Saddle * Suture * Synovial * Synchondrosis * Symphysis
2
1
3
4
LAB 7 EXERCISES 7-2

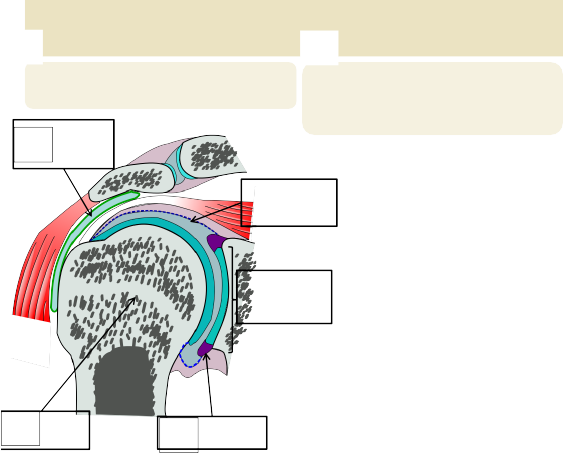

IDENTIFY THE COMPONENTS OF THE SHOULDER & HIP JOINT
A
B
1
Match the following: Bursa * Glenoid labrum * Synovial membrane * Head (of humerus) * Glenoid cavity of scapula
Draw & Label the following on this hip socket cross-section: Articular cartilage * Acetabular labrum * Ligamentum teres * Synovial membrane * Synovial cavity * Joint capsule.
4
5
2
3
LAB 7 EXERCISES 7-3
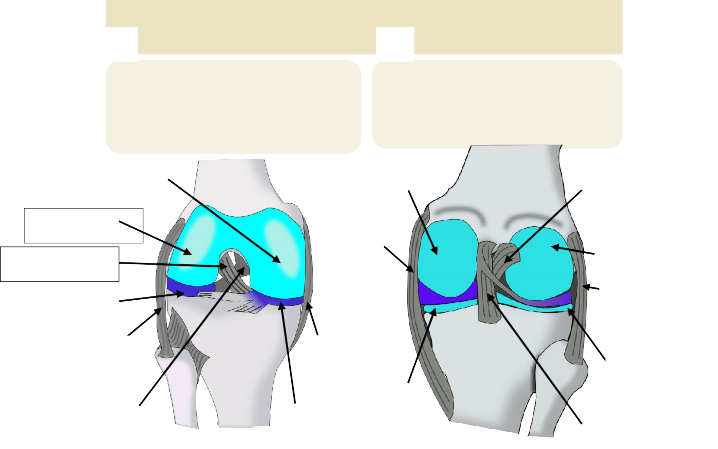
IDENTIFY THE COMPONENTS OF THE KNEE JOINT
A
B
Label the following: Medial condyle * Lateral condyle * Medial collateral ligament *
Lateral collateral ligament * Medial meniscus * Lateral meniscus * Anterior cruciate ligament * Posterior cruciate ligament.
Label the following: Anterior cruciate ligament * Posterior cruciate ligament * Medial collateral ligament * Lateral collateral ligament * Medial meniscus * Lateral meniscus * Medial condyle * Lateral condyle.
1
8
12
3
2
9
13
4
14
5
10
15
6
7
11
16
Ventral view Dorsal view
LAB 7 EXERCISES 7-4
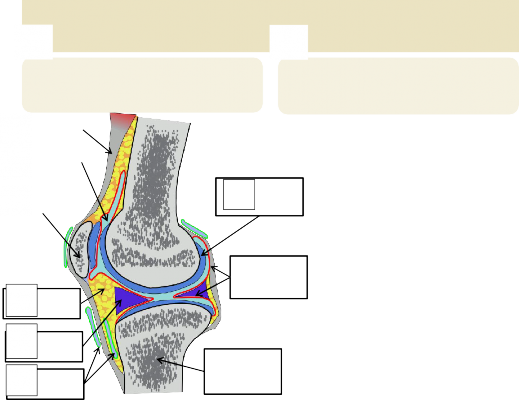
IDENTIFY THE COMPONENTS OF THE KNEE JOINT
A
B
6
5
7
9
13
8
Match the following: Quadriceps femoris tendon * Patella * Bursae * Fat pad * Joint cavity * Synovial membrane * Meniscus * Tibia * Articular cartilage
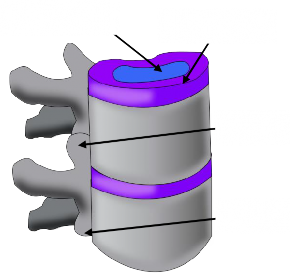
Label the following: Nucleus pulposis * Annulus fibrosus * Superior articular process * Inferior articular process.
|
1 |
|
|
2 |
|
|
3 |
10
11
4
12
Models: Knee, Shoulder, Hip and Spine
Knee joint:
- Anterior cruciate ligament
- Posterior cruciate ligament
- Fibular (Lateral) collateral ligament
- Tibial (Medial) collateral ligament
- Lateral meniscus
- Medial meniscus
- Quadriceps tendon
Elbow joint:
- Fibrous capsule
- Ulnar collateral ligament
- Annular ligament of radius
- Radial collateral ligament
Shoulder joint
- Fibrous capsule
- Coraco-humeral ligament
- Coraco-acromial ligament
- Gleno-humeral ligaments
- Transverse humeral ligament
Vertebral column
- Vertebral disc
Skeletal structures to review:
- Acromion
- Acetabulum
- Capitulum
- Clavicle
- Coracoid process
- Femur
- Fibula
- Glenoid cavity
- Head of humerus
- Head of femur
- Humerus
- Lateral condyle of femur
- Medial condyle of femur
- Olecranon
- Olecranon fossa
- Patella
- Popliteal surface
- Radius
- Radial fossa
- Scapula
- Trochlea
- Ulna