
4.8: Transcultural Nursing Care Models
- Page ID
- 49275

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Cultural Competence Models
- Burchum JLR; Cultural competence: Evolutionary dimension.
- Campinha-Bacote J; Cultural competence in providing health care services: Culturally adequate care model.
- Cross T., Bazron B; Dennis K., Isaacs M.; Towards a culturally adequate care process: Effective services for minority children with emotionally serious illness.
- Kim-Godwin YS; Clarke PN & Barton L.; Providing culturally adequate public care model.
- Leininger MM; The differences in cultural care and the theory of universality.
- Leininger M; Cultural care theory and ethnocentric research method.
- Leininger M; Evaluation of culture care for appropriate and adequate practices.
- Orque M.; Orque’s ethnic/cultural system: Conceptual framework for ethnic nursing care.
- Pacquiao DF; Cultural competence in ethical decision making.
- Papadopoulos I. & Lees S; Training culturally competent researchers.
- Purnell LD. & Amp; Paulanka BJ; Ppur model for cultural competence.
- Suh EE; Cultural competence model through evolutionary concept analysis.
- Wells M; Beyond cultural competence: a model for individual and institutional cultural development [4, 46].
Cultural Assessment Models
- Giger JN. & Davidhizar RE; Transcultural nursing; Evaluation and intervention
- Spector RE; Cultural difference in health and disease.
Cultural Assessment Guidelines
- Andrews MM; Culturally adequate nursing care.
- Andrews MM; History of health and cultural competence in physical examination.
- Bloch B; Bloch’s assessment guide for ethnic/cultural diversity.
- Boyle JS & Andrews MM; Andrews/Boyle assessment guide.
- Spector RE; Cultural care: guidelines for inheritance, assessment and health traditions [4, 46].
The conceptualization of the cultural competence model in nursing has emerged after 1989. Leininger, Campinha-Bacote, Giger and Davidhizar, Orque, Purnell and Paulanka, Spector, Andrews and Boyle are regarded as the pioneers contributing to the accumulation of the relevant data. Orque is a leading figure in developing a cultural model for nursing with “the conceptual framework of the ethnic system”. The use of nursing theories and models in nursing researches offers unparalleled contribution to the health care system through the practices of the nurse as a professional. Cultural competence models developed by nurse researchers can be transferred not only to nursing but also to other disciplines.
Leininger describes transcultural nursing as a branch of nursing or nursing school based on comparative research and analysis of different cultures which provides cultural universalism and cultural independence in nursing care and focuses on comparative studies and analyzing differences in cultures around the world in a respectful manner in view of health, illness, care, beliefs and values [3, 5, 13].
The aims of transcultural nursing are to provide sensitive and effective nursing care to meet the cultural needs of individuals, families and groups, to integrate transcultural concepts, theories and practices into nursing education, research and clinical applications, to improve transcultural nursing knowledge, and to incorporate this knowledge into nursing practice.
The International Nurses Association (ICN) invited the nurses from the World Health Organization (WHO) member countries to work on adaptable models to their communities at the 1989 Seoul Conference. The studies conducted in Turkey show that the nurses need to have classification lists and guidelines to be used in care, and thus a more systematic care will be provided in less time for individual patients and more data will be collected. In Turkey internationally developed models and classification systems in nursing care are translated into Turkish, or new guidelines specific to clinics are developed and used. These include NANDA’s diagnosis, Gordon’s Functional Health Patterns, NIC, NOC and Daily Living Activities and the OMAHA system [55].
The use of transcultural nursing models, classification systems and guidelines is becoming widespread. These models focus on the relationship of nursing to concepts and theories related to life, health, disease and society, facilitate organizing their thoughts, and provide a common language among professional members.
While there has been an increased awareness of the importance of cultural care and collecting cultural data in recent years in Turkey, no models or guides have been developed in Turkey [55].
These Models
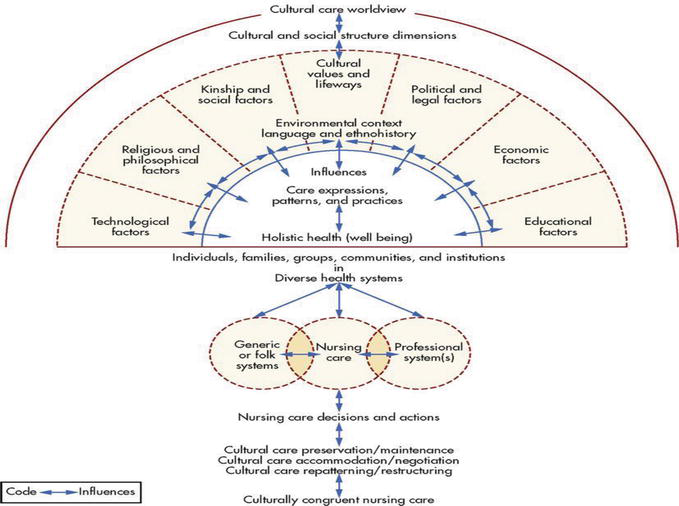
Leininger’s Sunrise Model
The “Culture Care Diversity and Universality” theory developed by Leininger in 1960, the first nurse who made the first work in this field and received the title of anthropologist, is the first theory developed in the field of transcultural nursing and still used worldwide. This theory focuses on exploring different and universal cultures and providing comparative care. It adopts a multi-factorial approach affecting health and care such as environmental conditions, ethnography, language, gender, class, racism, social structuring, belief, politics, economics, kinship, technology, culture and philosophy. This model includes technological, religious and philosophical, kinship and social factors, cultural values and lifestyle, political and legal, economic and social factors [50], which have been used in many studies in the west and in other countries since 1960 (Figure 4.8.1).
Narayanasamy’s ACCESS Model
Narayanasamy described the model in 1998 with the letters ACCESS (Assessment, Communication, Cultural negotiations and Compromise, Establishing respect, Sensitivity and Safety) to form the framework of cultural care practices [42] (Table 1).
| Transkültürel Hemşirelik | |
|---|---|
| Assessment | Culturally focusing on the patient’s life style, beliefs and practices related to health |
| Communication | Awareness of the variety of verbal and nonverbal reactions |
| Cultural Negotiation and Compromise | Becoming more aware of the other people’s cultures and exploring their problems as well as understanding the patient’s opinion, |
| Respect | Describing therapeutic relationship relevant to the patient’s cultural beliefs and consensus values |
| Sensitivity | Applying the sensitive care model to culturally different groups |
| Safety | Making the patient feel safe in the culturally sensitive care |
Table 1: Narayanasamy’s ACCESS model (1998).
Reference: [2].
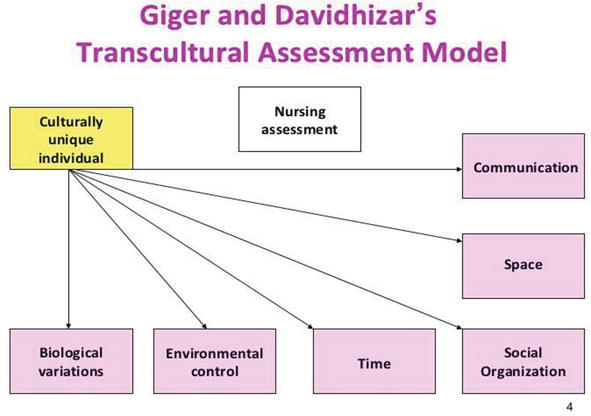
Giger and Davidhizar’s Trans-cultural Assessment Model
The model developed in 1988 was first published in 1990. This model is a tool developed to assess cultural values and their effects on health and disease behavior [33] (Figure 4.8.2).
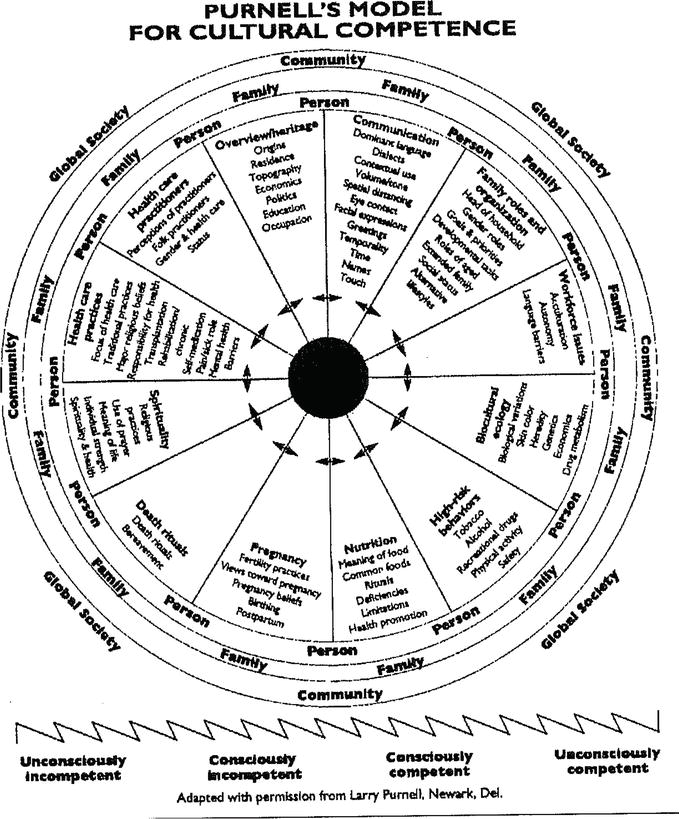
Purnell’s Cultural Competence Model
This ethnographic model created to promote cultural understanding of people’s status in the context of health promotion and illness is based on ethical perspectives of individual, family and community. It can be used in primary, secondary and tertiary protection stages [56] (Figure 4.8.3).
Nurses’ Competence to Provide Trans-cultural Care
- Having the ability to understand complex cultural dimensions,
- Assuming a holistic approach to care instead of biophysical approach,
- Showing efforts to reach rapidly increasing cultural beliefs and activities that are unique to distinct groups and individuals
- Being able to change the idea of believing that individuals’ own race is superior to others,
- Being able to make cultural evaluations,
- Developing communicative and scientific language skills,
- Being able to deal with cultural differences in real terms and make interpretations,
- Being able to use appropriate cultural teaching techniques
- Compromising cultural beliefs and studies with the general state of provision of health care,
- Respecting for the sociocultural diversity of women, newborn babies and their families [8, 57].