
4.1.2: FRAME 2- Analyze Cues
- Page ID
- 90008

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
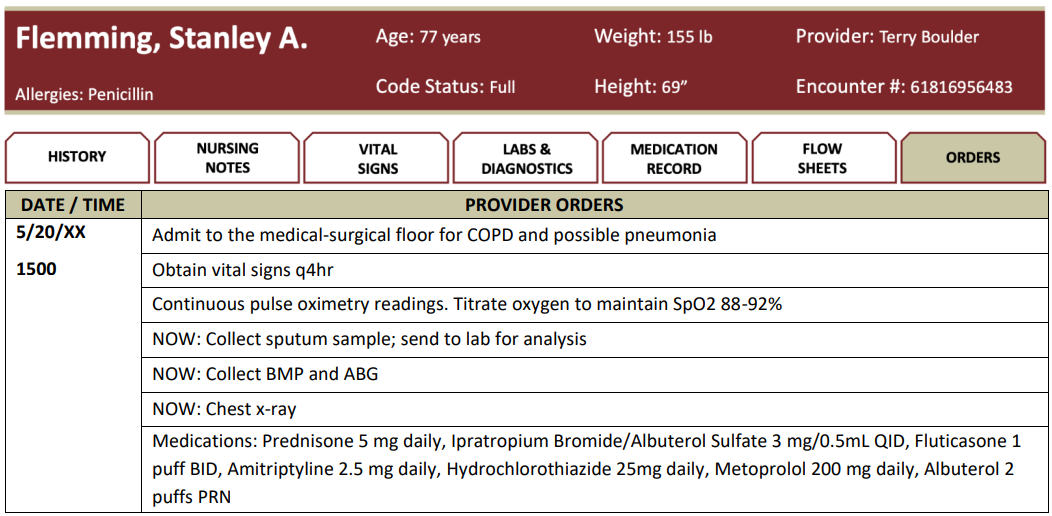
The nurse comes in to update Stanley that the provider has ordered a chest x-ray, labs, and sputum culture. The chest x-ray will be performed at the bedside, and a phlebotomist is on their way up to draw blood for the labs. The nurse provides education to Stanley about the process of collecting the sputum sample and asks him if he is able to produce some sputum. Stanley slides to the edge of the bed to better position himself in an upright position and puts his arms over the side table. After a few coughs, Stanley excretes a small amount of dark yellowish-green sputum into the cup. The nurse assists Stanley back to a comfortable, safe position.




QUESTION: Matrix Multiple Response Scoring Rule: +/-
Associate Stanley’s objective assessment findings with the corresponding respiratory condition. Each column must have at least one assessment piece. Some may have more than one respiratory condition associated with them.
| Objective Assessment | COPD | Pneumonia | Pulmonary Embolism | Asthma |
|---|---|---|---|---|
| Dyspnea | ||||
| Barrel chest appearance | ||||
| Expiratory wheezing | ||||
| Tachypnea | ||||
| Digital clubbing | ||||
| Productive cough | ||||
| Fever | ||||
| Abnormal ABG results |
Putting It All Together
DEBRIEF
Identifying respiratory conditions clinically manifested with dyspnea does not narrow down possible causes of a client’s condition. Nurses must utilize all clinical components when analyzing cues. Additionally, the nurse organizes, and links recognized cues to the client’s clinical presentation and considers potential issues. From there, the nurse narrows down what is the likely cause.
Clinical manifestations of COPD include dyspnea, increased anterior/posterior diameter (A/P diameter) or barrel chest appearance, expiratory wheezing, tachypnea, digital clubbing, and productive cough. An increased A/P diameter and clubbing of the digits are not clinical manifestations of pneumonia, pulmonary embolism, or asthma. Sudden shortness of breath and chest pain are common symptoms of a pulmonary embolism, while wheezing is rare, and if a cough is developed, often, it is dry or blood-tinged. Asthma is accompanied by shortness of breath and wheezing upon exhalation and is the most common sign in children with asthma. COPD requires a multidisciplinary approach, with healthcare professionals coordinating inputs and suitable therapies, medications, and monitoring equipment. Because COPD is a chronic and progressive disease, it is essential to promote patient empowerment.
Nurses have the unique ability to impact the client’s health education, early identification of decompensation, respiratory rehabilitation, and palliative care. Empowering nurse management of COPD clients through home visits and remote management with telemedicine is linked to achieving better outcomes in the day-to-day management of COPD and improving client’s knowledge of the disease (Aranburu-Imatz et al., 2022).
RECOGNIZING SOCIAL DETERMINANTS OF HEALTH (SDOH)
The SDOH domain, Neighborhood & Built Environment, is addressed in this case study when considering the causes of Stanley’s COPD and recurrent exacerbations. Both environmental and host factors should be considered. Environmental exposures, such as tobacco smoke and inhalation of particles, are the leading cause of COPD. Additional considerations may include occupational hazards, air quality, and genetic abnormalities. In addition, the exposures individuals occur at their workplaces can harm their health, such as secondhand smoke, unsafe air quality, and loud noises (Healthy People 2030). Stanley’s previous occupation exposed him to many years of fine dust particles, in addition to his smoking for many years. Recognizing the correlation of such risk factors is necessary when educating, advocating, and helping clients.
What Do You Think About?
- What other information would help establish the significance of cues for clients with pulmonary conditions?
- As the nurse, who else would you anticipate would need to be a part of a client with COPD healthcare’s team? What would a collaborative care team look like?
- What are some interventions and policy changes at the local, state, and federal level to help reduce health and safety risks and promote health?