
4.3.5: FRAME 5- Take Action
- Page ID
- 90025

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
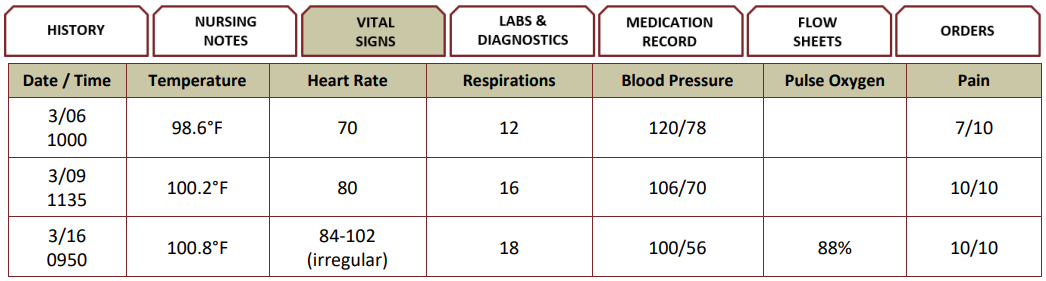
Six hours later, Rhys is completely unresponsive. He demonstrates Cheyne-Stokes respirations in a crescendo-diminuendo pattern with periods of apnea. He is hypotensive with tachypnea and tachycardia. He has been anuric for six hours.



QUESTION: Matrix Multiple Choice
Scoring Rule: 0/1
| Nursing Actions | Appropriate | Not Appropriate |
|---|---|---|
| Administer Morphine 10 mg orally | ||
| Administer Acetaminophen 650 mg rectal suppository | ||
| Inform family of transition | ||
| Suction secretions | ||
| Allow family time alone with client | ||
| Create comforting environment low stimuli | ||
| Offer culturally appropriate spiritual support |
Putting It All Together
DEBRIEF
Breathing patterns often change from a normal rate and rhythm to a new pattern, including periods of apnea and Cheyne-Stokes breathing. CheyneStokes breathing is indicative of impending death, generally minutes to hours (National Institute on Aging, 2022). Because death is imminent for Rhys, comfort care should not include medications such as morphine or acetaminophen. When clients are in their final hours and minutes of life, humanistic care is imperative when considering medication administration. Nursing actions should focus on the transition and supporting the family by creating a comforting, low stimuli environment, offering culturally appropriate end-of-life support, and providing time alone with the client. Suctioning the person during transition is not recommended. The irritation from the plastic tube can cause more secretions to be produced.
During end-of-life, it is important for the nurse to engage and maintain a therapeutic relationship with the family and communicate the signs and symptoms during the end-of-life transition.
Care for the family may need support and coaching as death approaches. Care continues through the death pronouncement, family notification of the death, and bereavement support (Harman et al., 2023). Many hospice programs offer bereavement services for families 12 months following the death of their loved one.
RECOGNIZING SOCIAL DETERMINANTS OF HEALTH (SDOH)
End-of-life care is complex and incorporates lessening untoward physical symptoms as well as providing emotional, spiritual, and social support. The perspective of what is valued will vary depending on the client and family’s culture, race/ethnicity, socioeconomic status, geographic location (urban/rural), insurance coverage, health literacy, and social support. Some cultures view death of a loved one as part of the natural cycle of life (Purnell, 2019, p. 116); in other cultures, death is perceived as a time of crisis (Purnell, 2019, p. 268).
What Do You Think About?
- What other signs or symptoms are common with end-of-life transition?
- What nursing actions could be considered?
- How will medication administration be altered in the final hours of life?
| Sign/Symptom | Nursing Actions |
|---|---|
| Change in Breathing |
Reassure family a change in breathing pattern is common and indicates decrease circulation. Non-pharmacologic Interventions: Elevate head of bed or turn client on their side. Pharmacologic Intervention: Morphine can help with breathing and respiratory congestion by decreasing fluid in the lungs and altering how the brain responds to pain. |
| Respiratory Congestion |
Reassure family respiratory congestion is not uncommon and does indicate pain. Non-pharmacologic Interventions: Gently turn client head to the side to drain secretions. Wipe their mouth with a cool cloth. Pharmacologic Intervention: Morphine can help with breathing and respiratory congestion by decreasing fluid in the lungs and altering how the brain responds to pain. |
| Fever |
Reassure the family that a fever is not uncommon with end-of-life transition. Non-pharmacologic Interventions: Apply a cool moist compress to forehead or neck, cooling blankets or sponging. Focus on core temp, not peripheral temps due to impaired perfusion. Pharmacologic Intervention: Assess need for analgesic or NSAID. |
| Sleeping or Unresponsiveness |
Reassure the family that increased amount of time sleeping is common. The client may become unresponsive, uncommunicative, or difficult to arouse are not uncommon responses. Non-pharmacologic Interventions: Comfort client by holding their hand, being present, speak in a normal voice. |
| Changes in color and temperature of hands and feet |
Reassure family that changes in the color and temperature is not uncommon. The skin may become grey, pallor, purple, mottled, and cool to touch. Changes in color and temperature of hands are due to impaired perfusion. Non-pharmacologic Interventions: Keep client warm and comfortable with soft blankets floating heals in bed or on pillow. |
| Restlessness |
Reassure the family that restlessness is not uncommon during the end-of-life transition. Restlessness is in part due to decreased oxygen and impaired circulation. Non-pharmacologic Interventions: Avoid restraining the client or interfering with the movements. Soft natural light, speaking in a calming voice, light massage to forehead, or soothing music are examples of therapeutic interventions for restlessness. Pharmacologic Intervention: Lorazepam can help the client to relax if they are experiencing apprehension, agitation, and/or restlessness. |
| Confusion |
Reassure the family that confusion is not uncommon during the end-of-life transition. Do not correct the client. These can present of delusion, or hallucinations symbolic language or actions. Non-pharmacologic Interventions: identify yourself before you speak, explain actions before you implement the plan, speak normally and clearly. |