
15.4: Vaginal Pressaries




- Last updated
- Sep 28, 2020
- Save as PDF

( \newcommand{\kernel}{\mathrm{null}\,}\)
Pessaries have been manufactured from many materials including silicone, rubber, clear plastic, soft plastic and latex. Most pessaries today are made of silicone and as a result are non allergic ,do not absorb odours or secrete substances. Silicone is resistant to breakdown with repeated cleansing and autoclaving. Pessaries are often used in pregnant patients, the elderly and in patients who do not want or are too frail to undergo surgery. Pessaries may also be used to facilitate preoperative healing of vaginal and cervical ulcers in patients who present with a procidentia. Another useful Pessaries have been manufactured from many materials including silicone, rubber, clear plastic, soft plastic and latex. Most pessaries today are made of silicone and as a result are non allergic, do not absorb odours or secrete substances. Silicone is resistant to breakdown with repeated cleansing and autoclaving. Pessaries are often used in pregnant patients, the elderly and in patients who do not want or are too frail to undergo surgery. Pessaries may also be used to facilitate preoperative healing of vaginal and cervical ulcers in patients who present with a procidentia. Another useful to ensure that the integrity of the silicone is intact .The vagina should also be examined for signs of constant pressure.
Patients should be advised that intercourse may be possible with a ring in situ. She should be aware that it may cause some discomfort to both partners in the beginning but this often settles as the patient and her partner become comfortable with it. Women who are able to remove and reinsert the pessary should be encouraged to do so prior to intercourse.
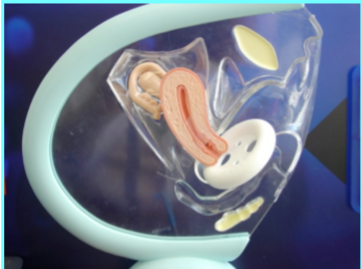
Figure 15.4.1: A simulated picture depicting the position and placement of the pessary
Contraindications to Pessary Insertion
- Severe untreated vaginal atrophy
- Vaginal bleeding of unknown origin
- Pelvic inflammatory disease
- Abnormal pap smear
- Dementia without possibility of dependable follow-up care
- Expected non-compliance with follow-up
Types of Pessaries
Often referred to as the “incontinence ring” since it has been designed for use in women with stress incontinence.
- Has a membrane to support prolapse.
- Has holes for drainage.
- Knob applies pressure to the urethra against the pubic bone.

Figure 15.4.2:
Soft silicone, donut shaped.
- Occludes upper vagina and supports a uterine prolapse
- Useful for cystocele or rectocele
- May be used for vault prolapse
- Adequate tone of the introitus is necessary for the pessary to remain in place

Figure 15.4.3:
White silicon cube
Indications: Third-degree prolapse, cystocele or rectocele, with or without good vaginal tone.
- Often this is the only satisfactory support for women with a complete prolapse
- Excellent for vaginal wall prolapse in that it keeps the vaginal walls from collapsing at the six pressure points.
- May be used by an athlete and removed after exercise.
- Mucosa molds to the concavities creating a negative pressure

Figure 15.4.4:
Incontinence Dish
- Dish-shaped pessary with holes to allow for drainage.
- The flexible membrane of the dish supports and elevates a mild cystocele.
- Used in patients with stress urinary incontinence with 1st or 2nd degree prolapse, or a mild cystocele.

Figure 15.4.5:
Arch Heel Gehrung
- U-shaped device that provides support to the anterior vaginal wall. The heel rests flat on the vaginal floor.
- It avoids pressure on the rectum while supporting the anterior wall.
- It is malleable and can be shaped to suit the shape of the vagina.
- Creates a “bladder bridge.”

Figure 15.4.6:
Ring - with and without support
- Helps support the urethra and bladder neck.
- Membrane provides additional support for a cystocele.
- Useful for a first or mild second-degree uterine prolapse associated with a mild cystocele.
Complications of pessaries
All authors listed vaginal discharge and odor as the most common complication. Other complications which may occur are pelvic pain, bleeding and development of urinary incontinence. Failure to retain a pessary in the vagina, or failure of the pessary to hold the prolapse properly is an obvious disadvantage. Flood and Hanson described erosions of the vaginal wall as being a common problem. They state that early intervention using an estrogen-based cream or vaginal lubricant are essential to proper pessary care. Severe complications such as vesico-vaginal fistulae, hydronephrosis, sepsis, and even small bowel incarceration were cited in the literature as the result of inadequate follow-up. Poma, reports in a review of 2,341 vaginal cancers, that 10.1% were associated with a pessary .It is debatable if this is a risk factor for vaginal malignancy.
Conclusion
There is paucity of good randomized controlled trails that evaluate the use of conservative methods for the management of pelvic organ prolapse. Perhaps with the POP Q scoring system for prolapse and renewed interest in non surgical management, this will change in the future.