
5.5: Understanding Blood Cholesterol and Heart Disease
- Page ID
- 21126
Learning Objectives
- Compare and contrast the roles of low-density lipoprotein (LDL) and high-density lipoprotein (HDL) in your body.
- Identify healthy blood lipid profile ranges.
You may have heard of the abbreviations LDL and HDL with respect to heart health. These abbreviations refer to low-density lipoprotein (LDL) and high-density lipoprotein (HDL). Lipoproteins are characterized by size, density, and composition; the various lipoproteins are described in more detail below.
Major Lipoproteins
Recall that chylomicrons are transporters of fats throughout the watery environment within the body. After about ten hours of circulating throughout the body, chylomicrons gradually release their triacylglycerols until all that is left of their composition is cholesterol-rich remnants. These remnants are used as raw materials by the liver to formulate specific lipoproteins. Following is a list of the various lipoproteins and their functions:
- VLDLs. Very low-density lipoproteins are made in the liver from remnants of chylomicrons and transport triacylglycerols from the liver to various tissues in the body. As the VLDLs travel through the circulatory system, lipoprotein lipase strips the VLDL of triacylglycerols. As triacylglycerol removal persists, the VLDLs become intermediate-density lipoproteins.
- IDLs. Intermediate-density lipoproteins transport a variety of fats and cholesterol in the bloodstream and are a little under half triacylglycerol in composition. While traveling in the bloodstream, cholesterol is gained from other lipoproteins while circulating enzymes strip its phospholipid component. When IDLs return to the liver, they are transformed into low-density lipoprotein.
- LDLs. Low-density lipoproteins are commonly known as “bad cholesterol”. LDLs carry cholesterol and other lipids from the liver to tissues throughout the body. LDLs are comprised of very small amounts of triacylglycerols, and contain over 50% cholesterol and cholesterol esters. As the LDLs deliver cholesterol and other lipids to the cells, each cell’s surface has receptor systems specifically designed to bind with LDLs. Circulating LDLs in the bloodstream bind to these LDL receptors and are brought into the cell. Once inside the cell, the LDL is taken apart and its cholesterol is released. A deficiency of these LDL receptors will leave a high quantity of cholesterol traveling in the bloodstream, which can lead to heart disease or atherosclerosis. Diets rich in saturated fats limit the number of LDL receptors and thus leave cholesterol in the bloodstream that could be deposited in arteries and block blood flow.
- HDLs. High-density lipoproteins are responsible for carrying cholesterol out of the bloodstream and into the liver, where it is either reused or removed from the body with bile. HDLs have a very large protein composition coupled with low cholesterol content compared to the other lipoproteins. Hence, these high-density lipoproteins are commonly called “good cholesterol.”
Contrasting LDL and HDL
Heart attacks and atherosclerosis are conditions often caused by cholesterol that has accumulated and thickened in the walls of arteries. HDLs and LDLs are directly connected to these life-threatening ailments. By comparing and contrasting the roles each of these lipoproteins serves in the health of heart and blood vessels, you will be able to construct and evaluate a plan of action for your personal health. Consider the following lipoprotein facts:
- LDL/HDL composition. LDL is approximately 25% protein and 75% cholesterol and other fats. LDL is bigger (yet lighter) and richer in cholesterol than HDL. HDL is 50% protein and 50% cholesterol and other fats. HDL is smaller, more dense, and richer in protein.
- LDL/HDL function. LDLs carry cholesterol into cells for normal usage, but LDLs can also deposit cholesterol into the walls of blood vessels, which can lead to harmful disease. HDLs scavenge excess cholesterol from the cells, tissues, and blood vessels and deliver these back to the liver, where these are either reused or excreted.
- LDL/HDL and inflammation. LDLs carry lipids that are pro-inflammatory and may contribute to heart disease. HDLs transport lipids that are anti-inflammatory and may reduce the occurrence of heart disease.
- LDL/HDL warnings. High LDL values warn of increased health risks for heart disease, while high HDL values indicate a reduced risk for heart disease.
- Oxidized LDL. LDLs become more dangerous when oxidized. Oxidation is defined as the loss of electrons between two substances via a chemical reaction. If LDL oxidation occurs, the oxidized LDL is left unstable. Oxidized LDL can speed up the process of plaque formation in the arteries. It is believed to hasten the deposition of cholesterol into the arterial walls and to induce a chronic inflammatory effect throughout the body’s vast network of vessels. This activity promotes atherosclerosis and significantly increases risks for heart attack or stroke.
Blood Cholesterol Recommendations
Desirable blood cholesterol levels for total cholesterol, LDL cholesterol, and HDL cholesterol are included in Table \(\PageIndex{1}\).1 More specifically, when looking at individual lipid profiles, a low amount of LDL and a high amount of HDL prevents excess buildup of cholesterol in the arteries and wards off potential health hazards. In other words, elevated LDL blood lipid profiles indicate an increased risk of heart attack, while elevated HDL blood lipid profiles indicate a reduced risk.
| Cholesterol Type | Category | mg/dL (milligrams per deciliter) |
|---|---|---|
|
Total Cholesterol |
Desirable Borderline High High |
less than 200 200-239 240 or higher |
| LDL Cholesterol |
Optimal Above Optimal Borderline High High Very High |
less than 100 100-129 130-159 160-189 190 or higher |
| HDL Cholesterol |
High Low |
60 or higher (considered protective) less than 40 |
Steps to Improving Blood Cholesterol Levels
Recommendations to improve blood lipid levels include:
- Maintain total fat intake within 20-35% of energy with an emphasis on monounsaturated and polyunsaturated fats
- Decrease saturated fat to less than 6% of total energy intake and avoiding trans fat2
- Increase omega-3 fats
- Consume the RDA for vitamin B6, B12, and folate
- Increase fruit, vegetable, and whole grain intake so fiber intake is 20-30 grams/day
- Don’t smoke2
- Be active for at least 150 minutes of moderate-intensity aerobic activity each week2
- Maintain a healthful body weight
Heart Disease
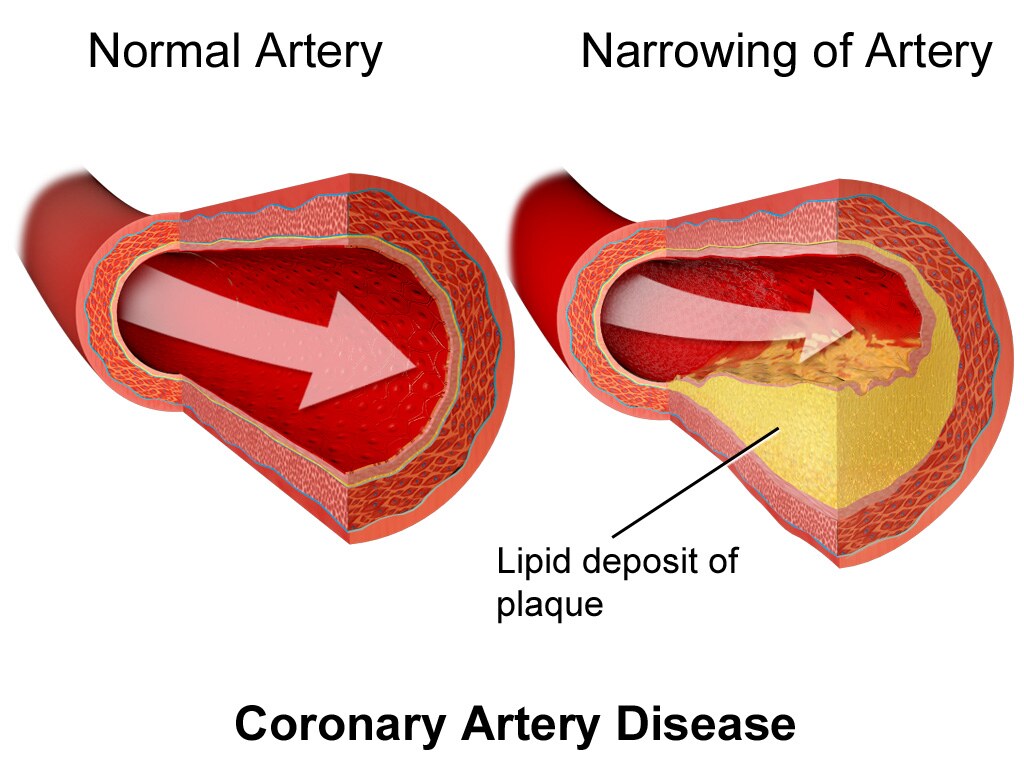
According to the Centers for Disease Control and Prevention (CDC), heart disease is the leading cause of death in the United States.3 The disease generally starts with atherosclerosis, or a hardening of the arteries. Arteries start to narrow and harden when fats accumulate along their inner walls and form plaques (Figure \(\PageIndex{1}\)). A plaque is made of fat, cholesterol, calcium, and other substances found in blood. The narrowing of the arteries causes the blood pressure to rise.
Plaque formation causes arteries to narrow and harden, which elevates blood pressure because the vessels can’t expand effectively to accommodate blood pulses. Higher blood pressure strains the heart and causes more damage. The plaques themselves can rupture due to a spike in blood pressure; the body responds to this perceived injury by forming blood clots. These clots are serious health threats, whether they are stationary (a thrombus) or moving (an embolus). A stable clot can slowly kill off surrounding tissue, or grow so big that it blocks blood circulation. When a moving clot becomes stuck in an artery too small for its passage, it cuts off blood flow and causes cell death. This is referred to as an embolism. Blood clots in heart and brain arteries can cause heart attacks or strokes.
Heart Disease Risk
Risk factors for heart disease include unmodifiable risk factors (that you can't change) and modifiable risk factors that you can change (Table \(\PageIndex{2}\)).
| Unmodifiable Risk Factors | Modifiable Risk Factors |
|---|---|
|
|
Steps to Reducing Heart Disease Risk
Diet and nutrition can play a significant role in reducing the risk of heart disease. It is helpful to limit consumption of saturated fat and trans fat which have negative impacts on blood cholesterol levels and promote plaque formation. Increasing consumption of dietary fiber can help improve blood cholesterol levels and may be helpful in maintaining or achieving a healthy weight. Being more active can help improve blood cholesterol levels and weight status.
High Blood Pressure
Chronic high blood pressure, also known as hypertension, is a significant health hazard affecting almost half of the adults in the United States.4 This chronic condition is a major cause of heart attacks and strokes, yet it has no symptoms until blood pressure reaches very high levels, which is why it is known as “the silent killer”. The only way to find out if you have high blood pressure is to get an accurate reading of your resting blood pressure rate, which is best done by a medical professional and should be monitored regularly.
High blood pressure is such an important factor in cardiovascular disease, that keeping it within a healthy range is important. Blood pressure is the force of moving blood against arterial walls. Blood pressure readings consist of two numbers and is reported as systolic pressure/diastolic pressure (e.g., 130/90). The top number measures systolic pressure (when the heart contracts) and the bottom number measures diastolic pressure (when the heart is at rest). The results are recorded in millimeters of mercury (mm Hg). The key blood pressure numbers to keep in mind are shown in Table \(\PageIndex{3}\).5 High blood pressure is characterized by above-average blood pressure readings (systolic blood pressure at or above 130 mm Hg or diastolic blood pressure at or above 80 mm Hg). Optimal systolic blood pressure is less than 120 mm Hg; optimal diastolic blood pressure is less than 80 mm Hg.
| Blood Pressure Category | Systolic mm Hg (upper number) | Diastolic mm Hg (lower number) |
|---|---|---|
|
Normal |
less than 120 and |
less than 80 |
| Elevated |
120-129 and |
less than 80 |
| High Blood Pressure (Hypertension) - Stage 1 |
130-139 or |
80-89 |
| High Blood Pressure (Hypertension) - Stage 2 | 140 or higher or | 90 or higher |
| Hypertensive Crisis (consult your doctor immediately) | higher than 180 and/or | higher than 120 |
Steps to Reducing the Risk of High Blood Pressure
Techniques to reduce blood pressure include being physically active, maintaining a healthy weight, reducing sodium intake to less than 2,300 mg per day, using alcohol moderately, and following the DASH eating plan. The DASH eating plan recommends:
- Eating vegetables, fruits, and whole grains
- Including fat-free or low-fat dairy products, fish, poultry, beans, nuts, and vegetable oils in the diet
- Limiting foods that are high in saturated fat, such as fatty meats, full-fat dairy products, and tropical oils such as coconut, palm kernel, and palm oils
- Limiting sugar-sweetened beverages and sweets.
Key Takeaways
- Some of the major lipoproteins are VLDL, IDL, LDL, and HDL.
- VLDL delivers triacylglycerols and other lipids to the body’s tissues and slowly becomes IDL. The liver uses IDL to create LDL, the main transporter of cholesterol.
- LDL, or “bad” cholesterol, has low protein composition and high cholesterol content. High levels of LDL have been shown to increase the risks for heart disease.
- HDL or “good’’ cholesterol has a larger proportion of protein and a small cholesterol composition. HDL scavenges excess cholesterol and returns it to the liver for reuse or disposal. A high level of HDL reduces the risk for heart disease.
- It is important to maintain a healthy lipid profile within recommended values in order to minimize the risk of heart disease.
- Heart disease risk factors include age, family history, obesity, physical inactivity, and undesirable blood cholesterol levels.
- Limiting saturated and trans fat intake while also increasing dietary fiber intake can help reduce heart disease risk.
- High blood pressure is a risk factor for heart disease.
References
- National Cholesterol Education Program. ATP III Guidelines At-A-Glance Quick Desk Reference. https://www.nhlbi.nih.gov/health-topics/all-publications-and-resources/atp-iii-glance-quick-desk-reference. Accessed June 17, 2020.
- Prevention and Treatment of High Cholesterol (Hyperlipidemia). https://www.heart.org/en/health-topics/cholesterol/prevention-and-treatment-of-high-cholesterol-hyperlipidemia. Accessed March 26, 2024.
- Heart Disease. FastStats - Heart Disease. cdc.gov. https://www.cdc.gov/nchs/fastats/heart-disease.htm. Accessed March 18, 2022.
- Facts About Hypertension. cdc.gov. https://www.cdc.gov/bloodpressure/facts.htm. Accessed June 18, 2020.
- Understanding Blood Pressure Readings. heart.org. https://www.heart.org/en/health-topics/high-blood-pressure/understanding-blood-pressure-readings. Accessed June 18, 2020.