
2.2: Chapter 2 – Definitions, terms, and Classification Systems for Co-Occurring Disorders
- Page ID
- 16013
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)In This Chapter…
- Terms Related to Substance Use Disorders
- Terms Related to Mental Disorders
- Terms Related to Clients
- Terms Related to Treatment
- Terms Related to Programs
- Terms Related to Systems
Overview
This chapter reviews and defines many of the terms that are applied commonly to co-occurring substance use and mental disorders (COD). Discussion points include how different terms have emerged, the contexts in which various classification systems are likely to be used, and why many of the specific terms and classification systems used throughout this TIP were chosen.
After a review of basic terminology related to substance use (including the distinction between abuse and dependence) and a brief description of mental disorders, the chapter discusses terms related to clients. A key point is the importance of using person-centered terminology as a way of acknowledging each client’s individuality. The chapter notes the many terms that may be used to describe co-occurring disorders, reviews the terms related to treatment and programs, and concludes with an overview of terms that describe the systems of care within which treatment occurs and programs operate.
The addiction counselor should be aware that the terminology and classifications introduced in this chapter, though important and useful, were developed by different groups for different purposes. Therefore, these terms do not necessarily form a seamless picture or work smoothly together. Nevertheless, they are useful and appropriate when used in the intended context. The reader who becomes conversant with these terms and classifications will find it easier to navigate the discussion of treatment issues (chapter 3) and to follow the TIP’s narrative.
Finally, this chapter contains brief Advice to the Counselor boxes, which readers with basic backgrounds, such as addiction counselors or other practitioners, can refer to for the most immediate practical guidance. (For a full listing of these boxes see the table of contents.)
Terms Related to Substance Use Disorders
Substance abuse and substance dependence are two types of substance use disorders and have distinct meanings. The standard use of these terms derives from the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association [APA] 1994). Produced by the APA and updated periodically, DSM-IV is used by the medical and mental health fields for diagnosing mental and substance use disorders. This reference provides clinicians with a common language for communicating about these disorders. The reference also establishes criteria for diagnosing specific disorders.
Substance abuse, as defined in DSM-IV-TR (4th edition, Text Revision; APA 2000), is a “maladaptive pattern of substance use manifested by recurrent and significant adverse consequences related to the repeated use of substances” (APA 2000, p. 198). Individuals who abuse substances may experience such harmful consequences of substance use as repeated failure to fulfill roles for which they are responsible, legal difficulties, or social and interpersonal problems. It is important to note that the chronic use of an illicit drug still constitutes a significant issue for treatment even when it does not meet the criteria for substance abuse specified in the text box below.
For individuals with more severe or disabling mental disorders, as well as for those with developmental disabilities and traumatic brain injuries, even the threshold of substance use that might be harmful (and therefore defined as abuse) may be significantly lower than for individuals without such disorders. Further-more, the more severe the disability, the lower the amount of substance use that might be harmful.
Substance dependence is more serious than abuse. This maladaptive pattern of substance use includes such features as increased tolerance for the substance, resulting in the need for ever-greater amounts of the substance to achieve the intended effect; an obsession with securing the substance and with its use; or persistence in using the substance in the face of serious physical or mental health problems. See the text box on page 23 for more information.
Criteria for a Diagnosis of Substance Abuse
- A maladaptive pattern of substance use leading to clinically significant impairment or distress, as manifested by one (or more) of the following, occurring within a 12-month period:
- Recurrent substance use resulting in a failure to fulfill major role obligations at work, school, or home (e.g., repeated absences or poor work performance related to substance use; substance-related absences, suspensions, or expulsions from school; neglect of children or household)
- Recurrent substance use in situations in which it is physically hazardous (e.g., driving an automobile or operating a machine when impaired by substance use)
- Recurrent substance-related legal problems (e.g., arrests for substance-related disorderly conduct)
- Continued substance use despite having persistent or recurrent social or interpersonal problems caused by or exacerbated by the effects of the substance (e.g., arguments with spouse about consequences of intoxication, physical fights)
- The symptoms have never met the criteria for Substance Dependence for this class of substance.
Source: APA 2000, p. 199.
Criteria for a Diagnosis of Substance Dependence
A maladaptive pattern of substance use, leading to clinically significant impairment or distress, as manifested by three (or more) of the following, occurring at any time in the same 12-month period:
- Tolerance, as defined by either of the following:
- A need for markedly increased amounts of the substance to achieve intoxication or desired effect.
- Markedly diminished effect with continued use of the same amount of the substance.
- Withdrawal, as manifested by either of the following:
- The characteristic withdrawal syndrome for the substance (refer to the DSM-IV-TR, Criteria A and B of the criteria sets for withdrawal from the specific substances).
- The same (or a closely related) substance is taken to relieve or avoid withdrawal symptoms.
- The substance is often taken in larger amounts or over a longer period than was intended.
- There is a persistent desire or unsuccessful efforts to cut down or control substance use.
- A great deal of time is spent in activities necessary to obtain the substance (e.g., visiting multiple doctors or driving long distances), use the substance (e.g., chain-smoking), or recover from its effects.
- Important social, occupational, or recreational activities are given up or reduced because of substance use.
- The substance use is continued despite knowledge of having a persistent or recurrent physical or mental health problem that is likely to have been caused or exacerbated by the substance (e.g., current cocaine use despite recognition of cocaine-induced depression, or continued drinking despite recognition that an ulcer was made worse by alcohol consumption).
Source: APA 2000, p. 197.
The term substance abuse has come to be used informally to refer to both abuse and dependence. Substance abuse treatment professionals commonly use the term “substance abuse” to describe any excessive use of addictive substances, whether the substance is alcohol or another drug. By and large the terms “substance dependence” and “addiction” have come to mean the same thing, though there is debate about the interchangeable use of these terms. When only those who are diagnosed as dependent are referenced, the specific term will be used.
Terms Related to Mental Disorders
The standard use of terms for non-substance use mental disorders, like the terms for substance use disorders, derive from the DSM-IVTR (APA 2000). These terms are used throughout the medical and mental health fields for diagnosing mental disorders. As with substance use disorders, this reference provides clinicians with a common language for communicating about these disorders. The reference also establishes criteria for diagnosing specific disorders. (See chapter 1, Figure 1-2 for an overview of the association between specific mental disorders and substance use disorders.)
The following section provides a brief introduction to some (not, by any means, all) of these disorders and offers advice to the addiction counselor and other practitioners for working with clients with these disorders. The consensus panel recognizes that addiction counselors are not expected to diagnose mental disorders. Clinicians in the substance abuse treatment field, however, should familiarize themselves with the mental disorders that co-occur with substance use disorders and/or that mimic symptoms of substance use disorders, particularly withdrawal or intoxication. The aim of providing this material is only to increase substance abuse treatment counselors’ familiarity with the mental disorders terminology and criteria necessary to provide advice on how to proceed with clients who demonstrate these disorders. (See chapter 8 and appendix D for more complete material on mental disorders co-occurring with substance use disorders.)
Personality Disorders
These are the disorders most commonly seen by the addiction counselor and in quadrant III substance abuse treatment settings (see Figure 2-1 for a depiction of the four quadrants). Individuals with personality disorders have symptoms and personality traits that are enduring and play a major role in most, if not all, aspects of the person’s life. These individuals have personality traits that are persistent and cause impairment in social or occupational functioning or cause personal distress. Symptoms are evident in their thoughts (ways of looking at the world, thinking about self or others), emotions (appropriateness, intensity, and range), interpersonal functioning (relationships and interpersonal skills), and impulse control.
Personality disorders are listed in the DSMIV under three distinct areas, referred to as “clusters.” The clusters are listed below with the types of symptoms or traits seen in that category. The specific personality disorders included in each cluster also are listed. For personality disorders that do not fit any of the specific disorders, the diagnosis of “personality disorder not otherwise specified” is used.
Cluster A: Hallmark traits of this cluster involve odd or eccentric behavior. It includes paranoid, schizoid, and schizotypal personality disorders.
Cluster B: Hallmark traits of this cluster involve dramatic, emotional, or erratic behavior. It includes antisocial, borderline, histrionic, and narcissistic personality disorders.
Cluster C: Hallmark traits of this cluster involve anxious, fearful behavior. It includes avoidant, dependent, and obsessive-compulsive personality disorders.
The prevalence of co-occurring substance abuse and antisocial personality disorder is high (Flynn et al. 1997). In fact, much of substance abuse treatment is targeted to those with antisocial personality disorders and substance abuse treatment alone has been especially effective for these disorders. Below is an Advice to the Counselor box on working with clients who have antisocial personality disorder; similar and more detailed advice boxes can be found throughout the TIP.
Advice to the Counselor:
Antisocial Personality Disorders
- Confront dishonesty and antisocial behavior directly and firmly.
- Hold clients responsible for the behavior and its consequences.
- Use peer communities to confront behavior and foster change.
Psychotic Disorders
The common characteristics of these disorders are symptoms that center on problems of thinking. The most prominent (and problematic) symptoms are delusions or hallucinations. Delusions are false beliefs that significantly hinder a person’s ability to function. For example, a client may believe that people are trying to hurt him, or he may believe he is someone else (a CIA agent, God, etc.). Hallucinations are false perceptions in which a person sees, hears, feels, or smells things that aren’t real (i.e., visual, auditory, tactile, or olfactory).
Psychotic disorders are seen most frequently in mental health settings and, when combined with substance use disorders, the substance disorder tends to be severe. Clients with psychotic disorders constitute what commonly is referred to as the serious and persistent mentally ill population. Increasingly, individuals with serious mental illness are present in substance abuse treatment programs (Gustafson et al. 1999).
Drugs (e.g., cocaine, methamphetamine, or phencyclidine) can produce delusions and/or hallucinations secondary to drug intoxication. Furthermore, psychotic-like symptoms may persist beyond the acute intoxication period.
Schizophrenia
This is one of the most common of the psychotic disorders and one of the most destructive in terms of the effect it has on a person’s life. Symptoms may include the following: hallucinations, delusions, disorganized speech, grossly disorganized or catatonic behavior, social withdrawal, lack of interest, and poor hygiene. The disorder has several specific types depending on what other symptoms the person experiences. In the paranoid type there is a preoccupation with one or more delusions or frequent auditory hallucinations. These often are experienced as threatening to the person. In the disorganized type there is a prominence of all of the following: disorganized speech, disorganized behavior, and flat or inappropriate affect (i.e., emotional expression).
Advice to the Counselor:
Psychotic Disorders
- Screen for psychotic disorders and refer identified clientsfor further diagnostic evaluation.
- Obtain a working knowledge of the signs and symptomsof the disorder.
- Educate the client and family about the condition.
- Help the client detect early signs of its re-occurrence byrecognizing the symptoms associated with the disorder.
Mood Disorders
The disorders in this category include those where the primary symptom is a disturbance in mood, where there may be inappropriate, exaggerated, or a limited range of feelings or emotions. Everyone feels “down” sometimes, and everybody experiences feelings of excitement or emotional pleasure. However, when a client has a mood disorder, these feelings or emotions are experienced to the extreme. Many people with substance use disorders also have a co-occurring mood disorder and tend to use a variety of drugs in association with their mood disorder. There are several types of mood disorders, including depression, mania,and bipolar disorder.
Advice to the Counselor:
Mood and Anxiety Disorders
- Differentiate between mood disorders, common- place expressions of depression, and depression associated with more serious mental illness.
- Conduct careful and continuous assessment since mood symptoms may be the result of substance abuse and not an underlying mental disorder.
- Combine addiction counseling with medication and mental health treatment.
Depression. Instead of just feeling“down,” the client might not be able to work or function at home, might feel suicidal, lose his or her appetite, and feel very tired or fatigued. Other symptoms can include loss of interest, weight changes, changes in sleep and appetite, feelings of worthlessness, loss of concentration, and recurrent thoughts of death.
Mania. This includes feelings that are toward the opposite extreme of depression. There might be an excess of energy where sleep is not needed for days at a time. The client may be feeling “on top of the world,” and during this time, the client’s decision making process might be significantly impaired and expansive and he may experience irritability and have aggressive outbursts, although he might think such outbursts are perfectly rational.
Bipolar. A person with bipolar disorder cycles between episodes of mania and depression. These episodes are characterized by a distinct period of abnormally elevated, expansive, or irritable mood. Symptoms may include inflated self-esteem or grandiosity, decreased need for sleep, being more talkative than usual, flight of ideas or a feeling that one’s thoughts are racing, distractibility, increase in goal-directed activity, excessive involvement in pleasurable activities that have a high potential for painful consequences (sexual indiscretions, buying sprees, etc.). Excessive use of alcohol is common during periods of mania.
Anxiety disorders. As with mood disorders, anxiety is something that everyone feels now and then, but anxiety disorders exist when anxiety symptoms reach the point of frequency and intensity that they cause significant impairment. In addiction treatment populations, the most common anxiety syndrome seen is that associated with early recovery, which can be a mix of substance withdrawal and learning to live without the use of drugs or alcohol. This improves with time and addiction treatment. However, other anxiety disorders that may occur, but need particular assessment and treatment, are social phobia (fear of appearing or speaking in front of groups), panic disorder (recurrent panic attacks that usually last a few hours, cause great fear, and make it hard to breathe), and posttraumatic stress disorders (which cause recurrent nightmares, anxiety, depression, and the experience of reliving the traumatic issues).
Terms Related to Clients
Person-Centered Terminology
In recent years, consumer advocacy groups have expressed concerns related to how clients are classified. Many take exception to terminology that seems to put them in a “box” with a label that follows them through life, that does not capture the fullness of their identities. A person with COD also may be a mother, a plumber, a pianist, a student, or a person with diabetes, to cite just a few examples. Referring to an individual as a person who has a specific disorder—a person with depression rather than “a depressive,” a person with schizophrenia rather than “a schizophrenic,” or a person who uses heroin rather than “an addict”—is more acceptable to many clients because it implies that they have many characteristics besides a stigmatized illness, and therefore that they are not defined by this illness.
Terms for Co-Occurring Disorders
Many terms have been used in the field to describe the group of individuals who have COD (most of these terms do not reflect the “people-first” approach used in this TIP). Some of these terms represent an attempt to identify which problem or disorder is seen as primary or more severe. Others have developed in the literature in order to argue for setting aside funding for special services or to identify a group of clients who may benefit from certain interventions. These terms include
- MICA—mentally ill chemical abuser. This acronym is sometimes seen with two As (MICAA) to signify mentally ill chemically addicted or affected. There are regional differences in the meaning of this acronym. Many States use it to refer specifically to persons with serious mental disorders.
- MISA—mentally ill substance abuser.
- MISU—mentally ill substance using.
- CAMI—chemically abusing mentally ill, or chemically addicted and mentally ill.
- SAMI—substance abusing mentally ill.
- MICD—mentally ill chemically dependent.
- Dually diagnosed.
- Dually disordered.
- Comorbid disorders.
- ICOPSD—individuals with co-occurring psychiatric and substance disorders.
While all of these terms have their uses, many have developed connotations that are not helpful or that have become too broad or varied in interpretation to be useful. For example, “dual diagnosis” also can mean having both mental and developmental disorders. Readers who hear these terms should not assume they all have the same meaning as COD and should seek to clarify the client characteristics associated with a particular term. Readers also should realize that the term “co-occurring disorder” is not inherently precise and distinctive; it also may become distorted by popular use, with other conditions becoming included within the term. The issue here is that clients/consumers may have a number of health conditions that “co-occur,” including physical health problems. Nevertheless, for the purpose of this TIP, co-occurring disorders refers to substance use disorders and mental disorders.
Some clients’ mental health problems may not fully meet the strict definition of co-occurring substance use and mental disorders criteria for diagnoses in DSM-IV categories. However, many of the relevant principles that apply to the treatment of COD also will apply to these individuals. Careful assessment and treatment planning to take each disorder into account will still be important. Suicidal ideation is an excellent example of a mental health symptom that creates a severity problem, but alone doesn’t necessarily meet criteria for a formal DSM-IV condition since suicidality is a symptom and not a diagnosis. Substance-induced suicidal ideation can produce catastrophic consequences. Some individuals may exhibit symptoms that could indicate the existence of COD but could also be transitory; for example, substance-induced mood swings, which can mimic bipolar disorder, or amphetamine-induced hallucinations or paranoia, which could mimic schizophrenia. Depending on the severity of their symptoms, these individuals also may require the full range of services needed by those who meet the strict criterion of having both conditions independently, but generally for acute periods until the substance-induced symptoms resolve.
Terms Related to Treatment
Levels of Service
The American Society of Addiction Medicine’s Patient Placement Criteria (ASAM PPC-2R) (ASAM 2001) envisions treatment as a continuum within which there are five levels of care. These levels of care are as follows:
- Level 0.5: Early Intervention
- Level I: Outpatient Treatment
- Level II: Intensive Outpatient/Partial Hospitalization Treatment
- Level III: Residential/Inpatient Treatment
- Level IV: Medically Managed Intensive Inpatient Treatment
Each level of care includes several levels of intensity indicated by a decimal point. For example, Level III.1 refers to “Clinically Managed Low-Intensity Residential Treatment.” A client who has COD might be appropriately placed in any of these levels of service.
Substance abuse counselors also should be aware that some mental health professionals may use another system, the Level of Care Utilization System for Psychiatric and Addiction Services. This system also identifies levels of care, including
- Level 1: Recovery Maintenance Health Management
- Level 2: Low Intensity Community Based Services
- Level 3: High Intensity Community Based Services
- Level 4: Medically Monitored Non-Residential Services
- Level 5: Medically Monitored Residential Services
- Level 6: Medically Managed Residential Services
These levels, like the ASAM levels, use a variety of specific dimensions to describe a client in order to determine the most appropriate placement (see the section in chapter 4, “Assessment Step 5,” for more information about these dimensions).
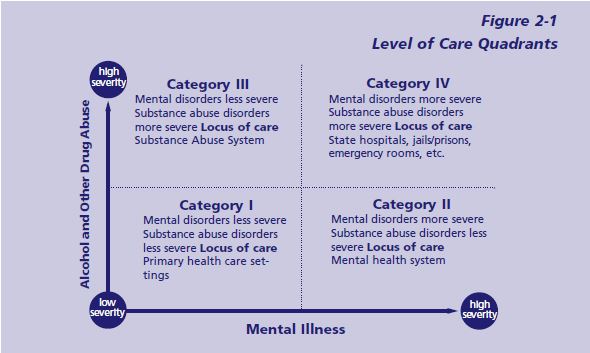
Quadrants of Care
The quadrants of care are a conceptual framework that classifies clients in four basic groups based on relative symptom severity, not diagnosis.
- Category I: Less severe mental disorder/ less severe substance disorder
- Category II: More severe mental disorder/ less severe substance disorder
- Category III: Less severe mental disorder/ more severe substance disorder
- Category IV: More severe mental disorder/ more severe substance disorder (National Association of State Mental Health Program Directors [NASMHPD] and
National Association of State Alcohol and Drug Abuse Directors [NASADAD] 1999)
For a more detailed description of each quadrant, see Figure 2-1 and text box on p. 30.
The quadrants of care were derived from a conference, the National Dialogue on Co-Occurring Mental Health and Substance Abuse Disorders, which was supported by the Substance Abuse and Mental Health Services Administration (SAMHSA) and two of its centers—the Center for Substance Abuse Treatment (CSAT) and the Center for Mental Health Services—and co-sponsored by NASMHPD and NASADAD. The quadrants of care is a model originally developed by Ries (1993) and used by the State of New York (NASMHPD and NASADAD 1999; see also Rosenthal 1992).
The four-quadrant model has two distinct uses:
- To help conceptualize an individual client’s treatment and to guide improvements in system integration (for example, if the client has acute psychosis and is known to the treatment staff to have a history of alcohol dependence, the client will clearly fall into Category IV—that is, severe mental disorder and severe substance use disorder). However, the severity of the client’s needs, diagnosis, symptoms, and impairments all determine level of care placement.
- To guide improvements in systems integration, including efficient allocation of resources. The NASMHPD–NASADAD National Dialogue recognized that currently “there is no single locus of responsibility for people with COD. The mental health and substance abuse treatment systems operate independently of one another, as separate cultures, each with its own treatment philosophies, administrative structures, and funding mechanisms. This lack of coordination means that neither consumers nor providers move easily among service settings” (NASMHPD and NASADAD 1999, p. ii).
Although the chapters of this TIP are not organized around the four-quadrant framework, most of the material in chapters 3 through 7 is directed primarily to addiction counselors working in quadrant III settings and other practitioners working in quadrant II settings.
Interventions
Intervention refers to the specific treatment strategies, therapies, or techniques that are used to treat one or more disorders. Interventions may include psychopharmacology, individual or group counseling, cognitive–behavioral therapy, motivational enhancement, family interventions, 12-Step recovery meetings, case management, skills training, or other strategies. Both substance use and mental disorder interventions are targeted to the management or resolution of acute symptoms, ongoing treatment, relapse prevention, or rehabilitation of a disability associated with one or more disorders, whether that disorder is mental or associated with substance use.
Integrated Interventions
Integrated interventions are specific treatment strategies or therapeutic techniques in which interventions for both disorders are combined in a single session or interaction, or in a series of interactions or multiple sessions. Integrated interventions can include a wide range of techniques. Some examples include
- Integrated screening and assessment processes
- Dual recovery mutual self-help meetings
- Dual recovery groups (in which recovery skills for both disorders are discussed)
- Motivational enhancement interventions (individual or group) that address issues related to both mental health and substance abuse or dependence problems
- Group interventions for persons with the triple diagnosis of mental disorder, substance use disorder, and trauma, or which are designed to meet the needs of persons with COD and another shared problem such as homelessness or criminality
- Combined psychopharmacological interventions, in which an individual receives medication designed to reduce cravings for substances as well as medication for a mental disorder
Integrated interventions can be part of a single program or can be used in multiple program settings.
Level of Care Quadrants
Quadrant I: This quadrant includes individuals with low severity substance abuse and low severity mental disorders. These low severity individuals can be accommodated in intermediate outpatient settings of either mental health or chemical dependency programs, with consultation or collaboration between settings if needed. Alternatively, some individuals will be identified and managed in primary care settings with consultation from mental health and/or substance abuse treatment providers.
Quadrant II: This quadrant includes individuals with high severity mental disorders who are usually identified as priority clients within the mental health system and who also have low severity substance use disorders (e.g., substance dependence in remission or partial remission). These individuals ordinarily receive continuing care in the mental health system and are likely to be well served in a variety of intermediate level mental health programs using integrated case management.
Quadrant III: This quadrant includes individuals who have severe substance use disorders and low or moderate severity mental disorders. They are generally well accommodated in intermediate level substance abuse treatment programs. In some cases there is a need for coordination and collaboration with affiliated mental health programs to provide ongoing treatment of the mental disorders.
Quadrant IV: Quadrant IV is divided into two subgroups. One subgroup includes individuals with serious and persistent mental illness (SPMI) who also have severe and unstable substance use disorders. The other subgroup includes individuals with severe and unstable substance use disorders and severe and unstable behavioral health problems (e.g., violence, suicidality) who do not (yet) meet criteria for SPMI. These individuals require intensive, comprehensive, and integrated services for both their substance use and mental disorders. The locus of treatment can be specialized residential substance abuse treatment programs such as modified therapeutic communities in State hospitals, jails, or even in settings that provide acute care such as emergency rooms (see chapter 7 for an example in an emergency room setting).
Episodes of Treatment
An individual with COD may participate in recurrent episodes of treatment involving acute stabilization (e.g., crisis intervention, detoxification, psychiatric hospitalization) and specific ongoing treatment (e.g., mental-health–supported housing, mental-health day treatment, or substance abuse residential treatment). It is important to recognize the reality that clients engage in a series of treatment episodes, since many individuals with COD progress gradually through repeated involvement in treatment.
Integrated Treatment
Integrated treatment refers broadly to any mechanism by which treatment interventions for COD are combined within the context of a primary treatment relationship or service setting. Integrated treatment is a means of actively combining interventions intended to address substance use and mental disorders in order to treat both disorders, related problems, and the whole person more effectively.
Culturally Competent Treatment
One definition of cultural competence refers to “the capacity of a service provider or of an organization to understand and work effectively with the cultural beliefs and practices of persons from a given ethnic/racial group” (Castro et al. 1999, p. 504). Treatment providers working with individuals with COD should view these clients and their treatment in the context of their language, culture, ethnicity, geographic area, socioeconomic status, gender, age, sexual orientation, religion, spirituality, and any physical or cognitive disabilities. For a full discussion of cultural issues in treatment for persons with substance use disorders, see the forthcoming TIP Improving Cultural Competence in Substance Abuse Treatment (CSAT in development a).
Cultural factors that may have an impact on treatment include heritage, history and experience, beliefs, traditions, values, customs, behaviors, institutions, and ways of communicating. The client’s culture may include distinctive ways of understanding disease or disorder, including mental and substance use disorders, which the provider needs to understand. Referencing a model of disease that is familiar to the client can help communication and enhance treatment. The counselor acquires cultural knowledge by becoming aware of the cultural factors that are important to a particular ethnic group or client.
Cultural competence may be viewed as a continuum on which, through learning, the provider increases his or her understanding and effectiveness with different ethnic groups. Various researchers have described the markers on this continuum (Castro et al. 1999; Cross 1988; Kim et al. 1992). The continuum moves from cultural destructiveness, in which an individual regards other cultures as inferior to the dominant culture, through cultural incapacity and blindness to the more positive attitudes and greater levels of skill described below:
- Cultural sensitivity is being “open to working with issues of culture and diversity” (Castro et al. 1999, p. 505). Viewed as a point on the continuum, however, a culturally sensitive individual has limited cultural knowledge and may still think in terms of stereotypes.
- Cultural competence, when viewed as the next stage on this continuum, includes an ability to “examine and understand nuances” and exercise “full cultural empathy.” This enables the counselor to “understand the client from the client’s own cultural perspective” (Castro et al. 1999, p. 505).
- Cultural proficiency is the highest level of cultural capacity. In addition to understanding nuances of culture in even greater depth, the culturally proficient counselor also is working to advance the field through leadership, research, and outreach (Castro et al. 1999, p. 505).
It is important to remember that clients, not counselors, define what is culturally relevant to them. It is possible to damage the relationship with a client by making assumptions, however well intentioned, about the client’s cultural identity. For example, a client of Hispanic origin may be a third-generation United States citizen, fully acculturated, who feels little or no connection with her Hispanic heritage. A counselor who assumes this client shares the beliefs and values of many Hispanic cultures would be making an erroneous generalization. Similarly, it is helpful to remember that all of us represent multiple cultures. Clients are not simply African– American, white, or Asian. A client who is a 20-year-old African-American man from the rural south may identify, to some extent, with youth, rural south, or African-American cultural elements—or may, instead, identify more strongly with another cultural element, such as his faith, that is not readily apparent. Counselors are advised to open a respectful dialog with clients around the cultural elements that have significance to them.
Integrated Counselor Competencies
A counselor has integrated competencies if he or she has the specific attitudes, values, knowledge, and skills needed to provide appropriate services to individuals with COD in the context of his or her actual job and program setting.
Just as other types of integration exist on a continuum, so too does integrated competency. Some interventions and/or programs require clinicians only to have basic competency in welcoming, screening, assessing, and identifying treatment needs of individuals with COD. Other interventions, programs, or job functions (e.g., those of supervisory staff) may require more advanced integrated competency. The more complex or unstable the client, the more formal mechanisms are required to coordinate the various staff members working with that client in order to provide effective integrated treatment.
A number of service delivery systems are moving toward identification of a required basic level of integrated competency for all clinicians in the mental health and substance abuse treatment systems. Many States also are developing curricula for initial and ongoing training and supervision to help clinicians achieve these competencies. Other State systems (e.g., Illinois) have created career ladders and certification pathways to encourage clinicians to achieve higher levels of integrated competency and to reward them for this achievement. (See chapter 3 for a full discussion of counselor competencies.)
Terms Related to Programs
A program is a formally organized array of services and interventions provided in a coherent manner at a specific level or levels of care in order to address the needs of particular target populations. Each program has its own staff competencies, policies, and procedures. Programs may be operated directly by public funders (e.g., States and counties) or by privately funded agencies. An individual agency may operate many different programs. Some agencies operate only mental health programs, some operate only substance abuse treatment programs, and some do both. An individual, licensed healthcare practitioner (such as a psychiatrist or psychologist) may offer her or his own integrated treatment services as an independent practitioner.
Key Programs
Mental health-based programs
A mental health program is an organized array of services and interventions with a primary focus on treating mental disorders, whether by providing acute stabilization or ongoing treatment. These programs may exist in a variety of settings, such as traditional outpatient mental health centers (including outpatient clinics and psychosocial rehabilitation programs) or more intensive inpatient treatment units.
Many mental health programs treat significant numbers of individuals with COD. Programs that are more advanced in treating persons with COD may offer a variety of interventions for substance use disorders (e.g., motivational interviewing, substance abuse counseling, skills training) within the context of the ongoing mental health treatment.
Substance abuse treatment programs
A substance abuse treatment program is an organized array of services and interventions with a primary focus on treating substance use disorders, providing both acute stabilization and ongoing treatment.
Substance abuse treatment programs that are more advanced in treating persons with COD may offer a variety of interventions for mental disorders (e.g., psychopharmacology, symptom management training) within the context of the ongoing substance abuse treatment.
Program Types
The ASAM PPC-2R (ASAM 2001) describes three different types of programs for people with COD:
- Addiction only services. This term refers to programs that “either by choice or for lack of resources, cannot accommodate patients who have mental illnesses that require ongoing treatment, however stable the illness and however well-functioning the patient” (ASAM 2001, p. 10).
- Dual diagnosis capable (DDC) programs are those that “address co-occurring mental and substance-related disorders in their policies and procedures, assessment, treatment planning, program content and discharge planning” (ASAM 2001, p. 362). Even where such programs are geared primarily to treat substance use disorders, program staff are “able to address the interaction between mental and substance-related disorders and their effect on the patient’s readiness to change—as well as relapse and recovery environment issues— through individual and group program content” (ASAM 2001, p. 362).
- Dual diagnosis enhanced programs have a higher level of integration of substance abuse and mental health treatment services. These programs are able to provide primary substance abuse treatment to clients who are, as compared to those treatable in DDC programs, “more symptomatic and/or functionally impaired as a result of their co-occurring mental disorder” (ASAM 2001, p. 10). Enhanced-level services “place their primary focus on the integration of services for mental and substance-related disorders in their staffing, ser-vices and program content” (ASAM 2001, p. 362).
See chapter 3 for a discussion of program terminology proposed by the consensus panel that works well for both the substance abuse and mental health fields (i.e., “basic,” “intermediate,” and “advanced”) and for a crosswalk of this terminology with the ASAM program types.
A system is a means of organizing a number of different treatment programs and related services to implement a specific mission and common goals.
Terms Related to Systems
For the purposes of this TIP, a system is a means of organizing a number of different treatment programs and related services to implement a specific mission and common goals. A basic example of a system is SAMHSA. Single State Agencies are systems that organize statewide services. There may also be county, city, or local systems in various areas. A system executes specific functions by providing services and related activities. It is often, but not always, a government agency. Systems may be defined according to a number of different characteristics: a section of government, a geographic entity, or a payor (e.g., the Medicaid system of care).
Systems work with other systems in a variety of ways and with different degrees of integration. The primary systems with which people with COD interact are the substance abuse treatment and mental health services systems. Other systems that frequently come into play are health care, criminal justice, and social services. Systems are usually the entities that determine funding, standards of care, licensing, and regulation.
Substance Abuse Treatment System
The substance abuse treatment system encompasses a broad array of services organized into programs intended to treat substance use disorders (including illegal substances, such as marijuana and methamphetamine, and legal substances, such as alcohol for adults over 21 years of age). It also includes services organized in accord with a particular treatment approach or philosophy (e.g., methadone treatment for opioid dependence or therapeutic communities). A system may be defined by a combination of administrative leadership (e.g., through a designated director of substance abuse treatment services), regulatory oversight (e.g., all programs that have substance abuse treatment licenses), or funding (e.g., all programs that receive categorical substance abuse funding, or, more rarely, bill third-party payors for providing substance abuse services).
In most substance abuse treatment systems, the primary focus is on providing distinct treatment episodes for the acute stabilization, engagement, active treatment, ongoing rehabilitation of substance use disorders, and relapse prevention. More intensive services are almost invariably targeted to the treatment of substance dependence. The primary focus of intervention is abstinence from illicit drugs for those who use illicit drugs and from alcohol for those who use alcohol excessively.
Mental Health Service System
The mental health service system includes a broad array of services and programs intended to treat a wide range of mental disorders. Like the substance abuse treatment system, the coherence of the mental health system is defined by a combination of administrative leadership (e.g., through a designated director of mental health services), regulatory oversight (e.g., all programs which have mental health licenses), and funding (e.g., all programs which receive categorical mental health funding or that primarily bill third party payors for providing mental health services).
In most mental health systems, services are provided for a wide range of mental disorders; however, in many publicly financed mental health programs, the priority is on acute crisis intervention and stabilization and on the provision of ongoing treatment and rehabilitative services for individuals identified as having SPMI. Typically, the mental health system identifies a cohort of priority clients (identified by a State’s definition of SPMI) for which it assumes continuing responsibility, often by providing continuing case management, psychiatric rehabilitation services, and/or housing support services.
Interlinking Systems
Depending on the life area affected at a given moment, individuals with COD may present themselves at different venues. For example, a person who experiences an array of problems in addition to the COD—such as homelessness, legal problems, and general medical problems—may first be seen at a housing agency or medical clinic. Historically, the distinctive boundaries maintained between systems have impeded the ability of individuals with COD to access needed services (Baker 1991; Schorske and Bedard 1989).
Intersystem linkages are essential to a comprehensive service delivery system. Fundamental to effective linkage is the collaboration between substance abuse treatment and mental health systems, because they are the primary care systems for persons with COD. The coordination of these systems enhances the quality of services by removing barriers that impede access to needed services. For example, access to care and quality of care have been impeded historically by the failure to address issues of language and culture. Intersystem coordination can lead to cohesive and coordinated delivery of program and services, where the burden is not on the individual to negotiate services and the system’s resources are used more effectively. The criminal justice system now plays a central role in the delivery of treatment for both mental health and substance use disorders, especially for those persons with COD, so it is important to ensure coordination with this system as well. Community health centers and other primary health providers also play critical roles in substance use disorder treatment and mental health treatment.
Comprehensive Continuous Integrated System of Care
The Comprehensive Continuous Integrated System of Care model (CCISC) is a model to bring the mental health and substance abuse treatment systems (and other systems, potentially) into an integrated planning process to develop a comprehensive, integrated system of care. The CCISC is based on the awareness that COD are the expectation throughout the service system. The entire system is organized in ways consistent with this assumption. This includes system-level policies and financing, the design of all programs, clinical practices throughout the system, and basic clinical competencies for all clinicians. This model derives from the work of the SAMHSA Managed Care Initiative Consensus Panel on developing standards of care for individuals with COD (Center for Mental Health Services 1998; Minkoff 2001a). CCISCs are grounded in the following assumptions:
- The four-quadrant model is a valid model for service planning.
- Individuals with COD benefit from continuous, integrated treatment relationships.
- Programs should provide integrated primary treatment for substance use and mental disorders in which interventions are matched to diagnosis, phase of recovery, stage of change, level of functioning, level of care, and the presence of external supports and/or contingencies.
This model has been identified by SAMHSA as an exemplary practice and is at various stages of implementation in a number of States. States in various stages of implementing the CCISC model include Alabama, Alaska, Arizona, Maine, Maryland, Massachusetts, Montana, and New Mexico, as well as the District of Columbia. Regional projects are underway in Florida, Louisiana, Michigan, Oregon, Texas, and Virginia.