
14.2: Chronic Myelogenous Leukemia (CML)
- Page ID
- 38849

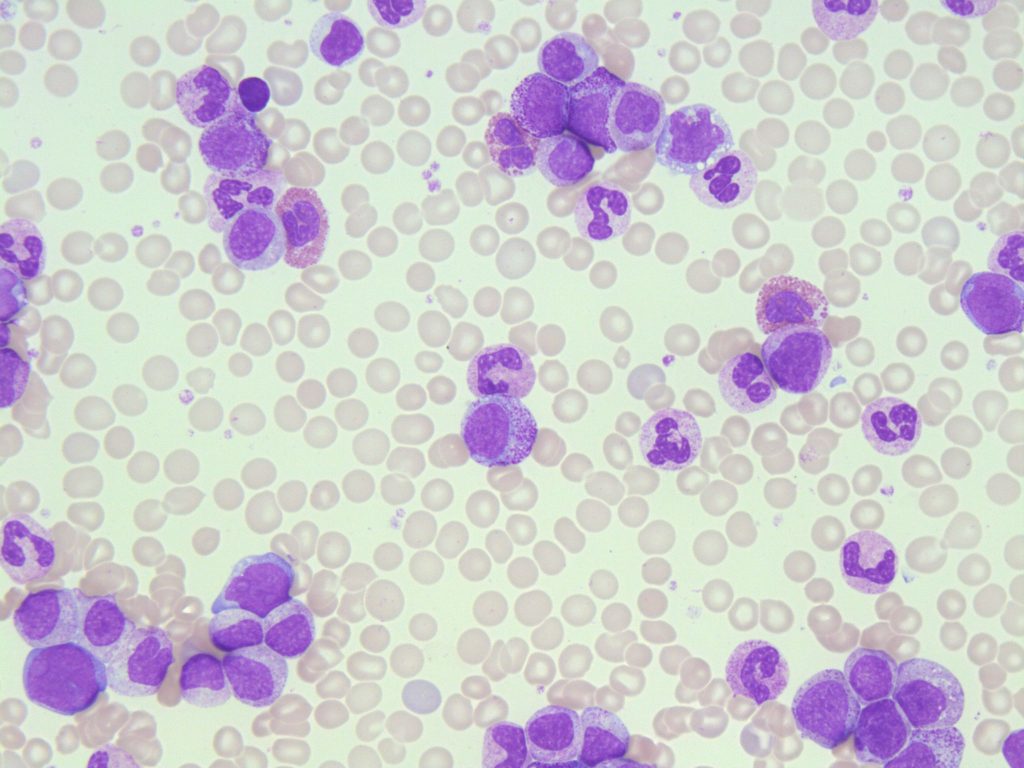
- An image from a peripheral blood smear demonstrating myeloid precursors and a few blasts seen in chronic myelogenous leukemia. 50x oil immersion. From MLS Collection, University of Alberta, https://doi.org/10.7939/R3NZ8155H
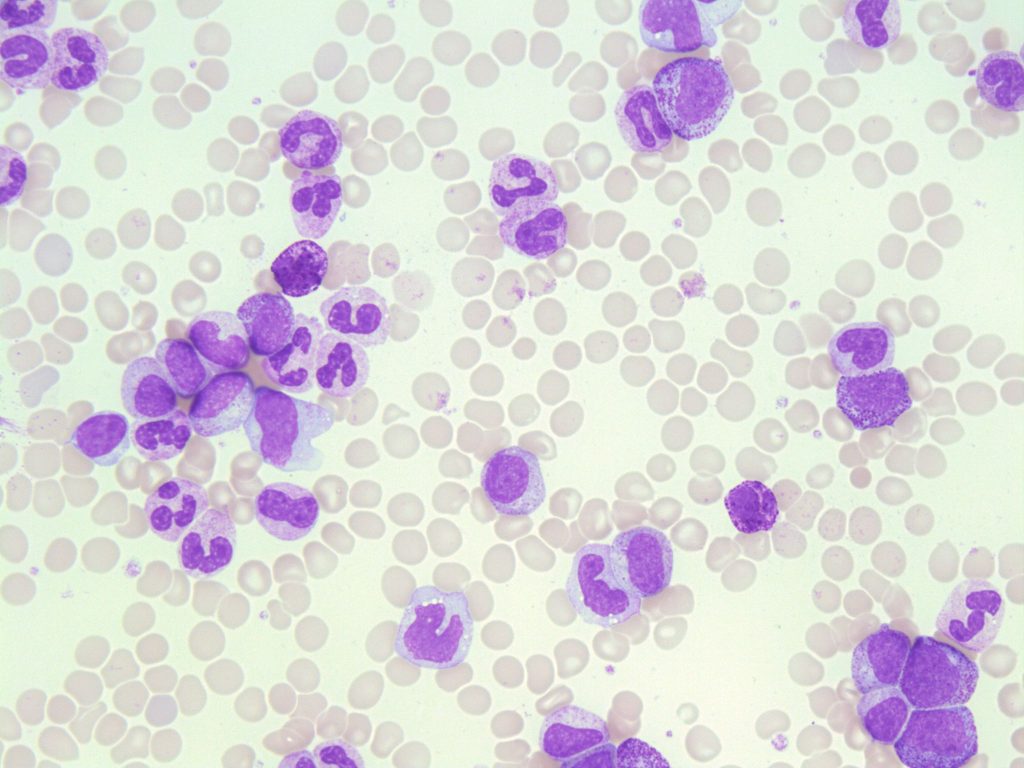
- An image from a peripheral blood smear demonstrating a neutrophilia and myeloid precursors seen in CML. 500x oil immersion. From MLS Collection, University of Alberta, https://doi.org/10.7939/R3SQ8QZ9V
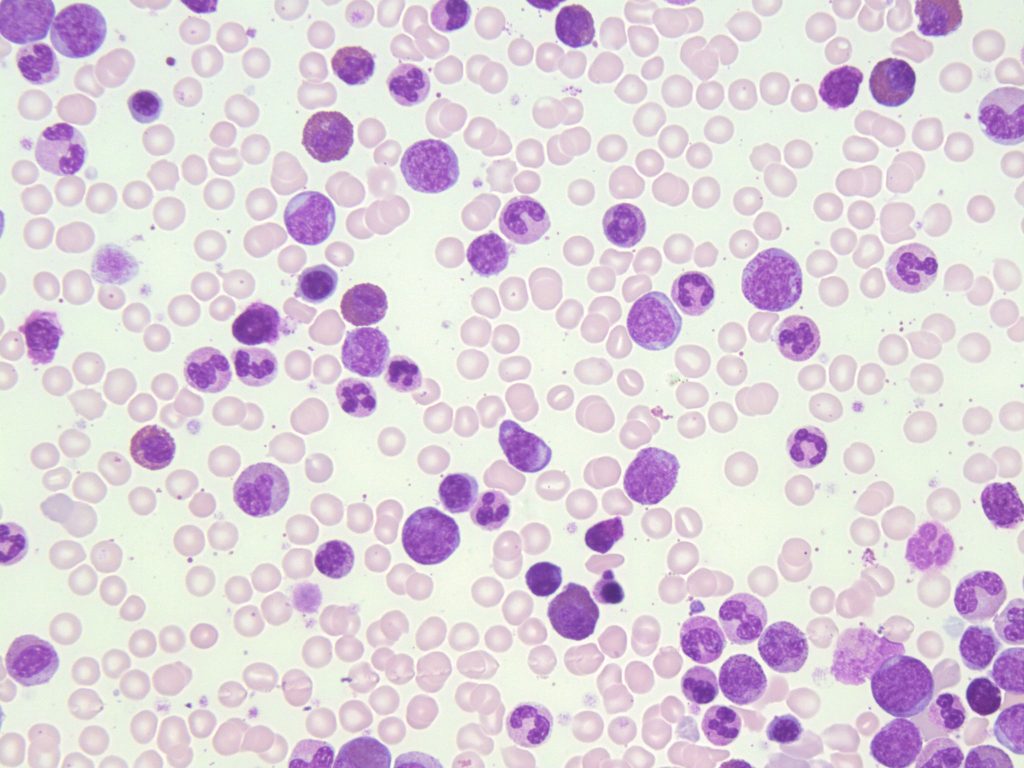
- An image from a bone marrow smear demonstrating myeloid hyperplasia and a few blasts seen in chronic myelogenous leukemia. Very few erythroid precursors are present. 50x oil immersion. From MLS Collection, University of Alberta, https://doi.org/10.7939/R38P5VR48
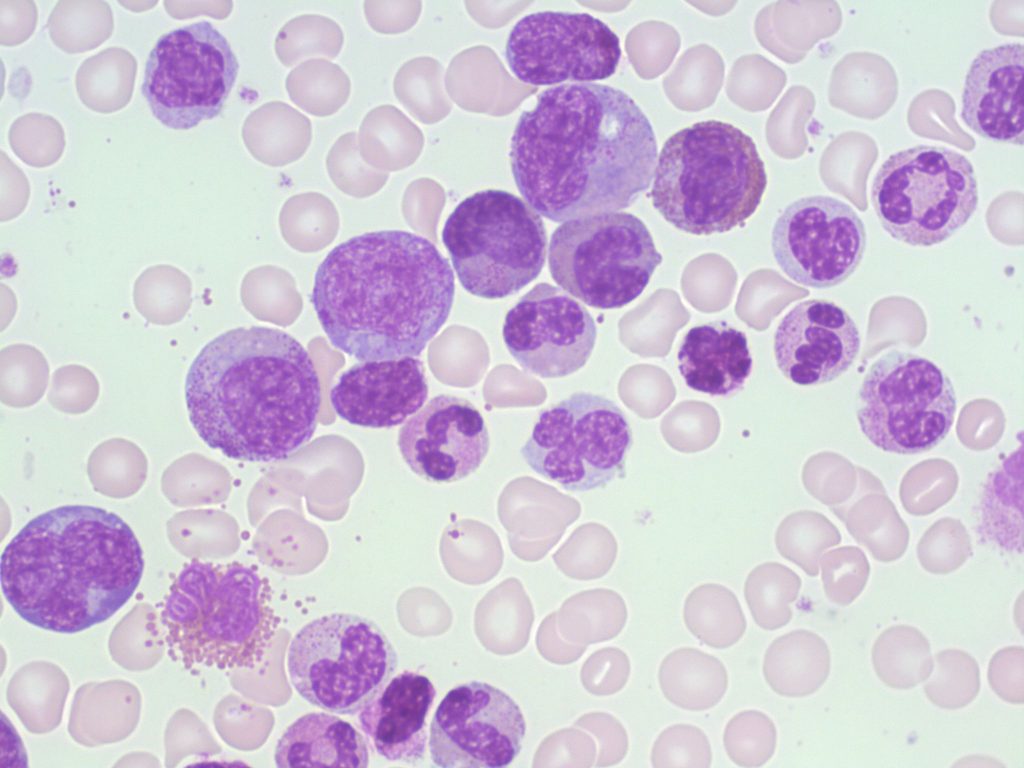
- An image from a bone marrow smear demonstrating myeloid hyperplasia in CML. 100x oil immersion. From MLS Collection, University of Alberta, https://doi.org/10.7939/R34X54Z0H
Affected Cell Line: Myeloid cell line (platelets and granulocytes are increased, however granulocyte production is most prominent).1,2
Mutation: Philadelphia Chromosome, t(9;22), resulting in the BCR-ABL1 fusion gene.3 The gene is characterized by a translocation between chromosomes 9 and 22 which is expressed as t(9;22).1
Age Group Affected: Seen commonly in middle aged adults, 46 to 53 years old.1
Clinical Features:
The onset of CML is insidious and in some patients may be asymptomatic.3 Other patients may have complications associated with frequent infections, infiltration of leukocytes, bleeding, weight loss, fever, fatigue, and anemia.1,4
Extramedullary hematopoiesis may occur, resulting in organomegaly.1
The course of CML occurs in three phases:
1. Chronic Phase
Peripheral blood: leukocytosis (usually >100 x109/L), thrombocytosis (Up to >1000 x109/L).3
Bone Marrow: hypercellularity due to increased granulopoiesis. Megakaryocytes are increased and may appear small and hypolobulated.3
2. Accelerated Phase
The bone marrow is hypercellular and often myelodysplastic features are seen. Additionally, there is an increased number of myeloblasts, and a dropping platelet count resulting in thrombocytopenia. Total white blood cell count continues to increase.3,4
3. Blast Phase (Acute Leukemia)
CML has transformed into an acute leukemia, either ALL or AML, and prognosis becomes poor even with treatment.4
Blast Phase is diagnosed when either: Bone marrow shows ≥20% blasts or when extramedullary blast proliferation is present.3,4
Laboratory Findings for CML:1,3,4
|
CBC: RBC: Decreased WBC: Increased (Average: >100 x109/L) PLT: Increased to Normal to Decreased (depending on phase) Hb: Decreased RETIC: Normal to Decreased |
PBS: +/- NRBCs Neutrophilia, Eosinophilia, Basophilia +/- Micromegakaryocytes Left shift Dysplastic features may be present in granulocytes and platelets |
BM: M:E ratio: Increased Hypercellular Myeloid Hyperplasia Megakaryocytes: Increased, may be dysplastic Fibrosis in later stages |
|
Other Tests: LAP: Decreased Cytogenetics Hyperuricemia Uricosuria (May lead to gout) PLT Function: Abnormal |
Leukemoid Reaction
A leukemoid reaction is a response to different stress events such as infections, inflammation, hemorrhage, or other malignant disorders that has a similar presentation to CML where there is an increase in the number of white blood cells and a left shift.4,5
A leukemoid reaction should NOT be confused with CML.
Table 1. Comparison of CML and Leukemoid Reaction.4,5
| Laboratory Finding | CML | Leukemoid Reaction |
| PBS |
Left shift (Very Immature) Neutrophilia Eosinophilia Basophilia Dysplastic Features |
Left shift (mild) Neutrophilia Absent eosinophilia Absent Basophilia Toxic changes are often present |
| WBC | 20-500 x109/L | Rarely >60 x109/L |
| PLT | Increased | Normal |
| Anemia | Present | Absent |
| LAP Score | Low | High |
| Chromosomal Abnormality | Philadelphia Chromosome/BCR-ABL1 | None |
References:
1. Randolph TR. Myeloproliferative neoplasms. In: Rodak’s hematology clinical applications and principles. 5th ed. St. Louis, Missouri: Saunders; 2015. p.561-90.
2. Schaub CR. Chronic Myeloproliferative disorders I: chronic myelogenous leukemia. In: Clinical hematology and fundamentals of hemostasis. 5th ed. Philadelphia: F.A. Davis Company; 2009. p. 371-84.
3. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. editors. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues Volume 2. 4th ed. International Agency for Research on Cancer (IARC); 2008.
4. Randolph TR. Myeloproliferative neoplasms. In: Clinical laboratory hematology. 3rd ed. New Jersey: Pearson; 2015. p. 450-78.
5. Bain BJ. Disorders of white cells. In: Blood cells: a practical guide [Internet]. 5th ed. Chichester, UK: John Wiley & Sons, Ltd; 2015 [cited 2018 Jul 10]:416-81. Available from: http://doi.wiley.com/10.1002/9781118817322