
14.3: Polycythemia Vera (PV)
- Page ID
- 38850

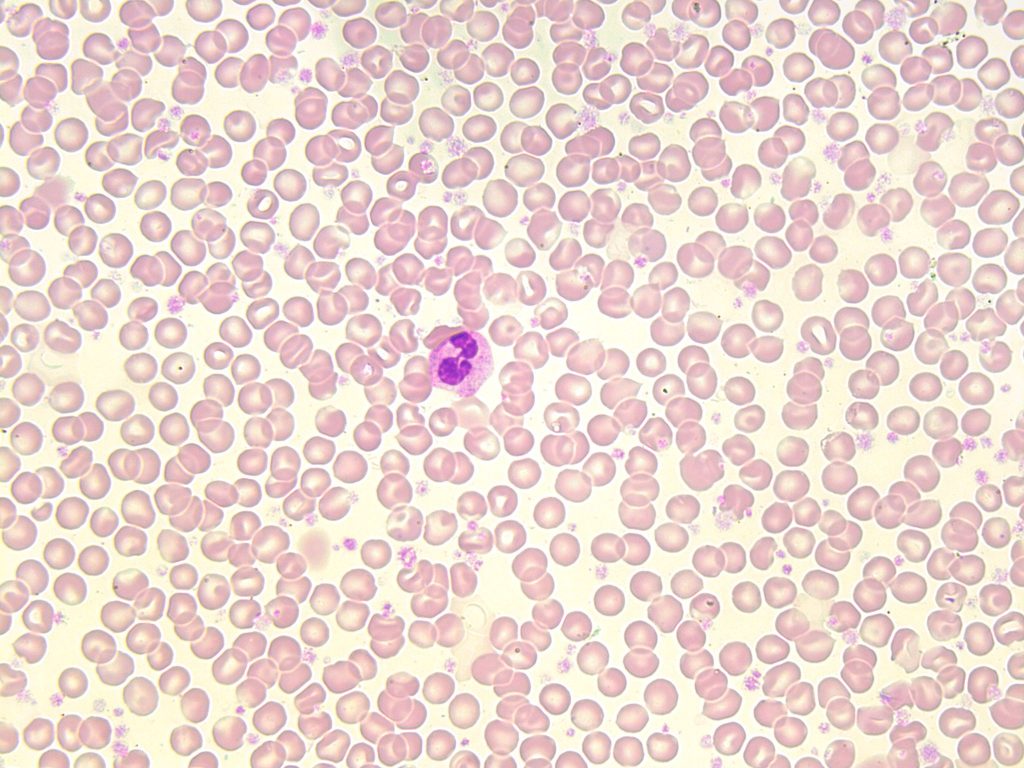
- An image from a peripheral blood smear showing a thick smear with an abundant red blood cells and platelets often seen in polycythemia vera, 100x oil immersion. From MLS Collection, University of Alberta, https://doi.org/10.7939/R3WH2DW3X
Affected Cell Line: Mainly erythrocytes, though tri-lineage growth (“panmyelosis”) is seen in the bone marrow.1,2
Mutation:
JAK 2 exon 12 and JAK 2 V617F gene mutations have been associated with PV.1,3
Age Group Affected: Average age of diagnosis is 60 years old.3
Features:
PV involves the proliferation of erythrocytes independent of normal erythropoiesis regulating mechanisms (e.g. erythropoietin). There is also an a proliferation of granulocytes and megakaryocytes (resulting in “panmyelosis”) but the proliferation of erythrocytes is most prominent.3-5
Unlike CML, PV does not readily transform into acute leukemia but may result in fibrosis over time.3 Splenomegaly is commonly seen.
Laboratory Findings for PV:2,4,5
|
CBC: RBC: Increased WBC: Increased PLT: Increased Hb: Increased Hct: Increased MCV: Increased RETIC: Normal to increased |
PBS: RBCs are normochromic/normocytic, though iron stores may be exhausted, leading to hypo/micro RBCs PBS appears crowded with RBCs (thick smears are due to the elevated Hct) A left shift and basophilia may be seen |
BM: M:E ratio: Normal to decreased Hypercellular due to increased proliferation in all cell lines Megakaryocytes are increased in number and may be enlarged and exhibit lobulated nuclei Iron stores: decreased to absent |
|
Other Tests: Erythropoietin: Low or normal |
Secondary Polycythemia
Secondary polycythemia is a condition that occurs when there is an increased production of erythrocytes due an increased level of erythropoietin. Bone marrow shows an erythroid hyperplasia.5
Causes include: Hypoxia, Inappropriate use of erythropoietin, Familial polycythemia, neonatal polycythemia.5
Relative Polycythemia
Polycythemia that occurs due to a decrease in plasma volume, resulting in an elevated hematocrit, RBC count, and hemoglobin. There is no actual increased production of erythrocytes.5 The decrease in plasma volume is often the result of dehydration.
Hemoglobin and hematocrit appear increased but other CBC parameters such as white blood cell and platelet counts are normal. The bone marrow is also normal in terms of iron stores, cellularity and number of megakaryocytes.5
Table 1. Comparison between the different Polycythemias.5
| Laboratory Finding | PV | Secondary | Relative |
| Hct | Increased | Increased | Increased |
| Hb | Increased | Increased | Increased |
| WBC | Increased | Normal | Normal |
| PLT | Increased | Normal | Normal |
| Erythropoietin | Decreased | Increased | Normal |
| Bone Marrow | Panmyelosis | Erythroid hyperplasia | Normal |
| Chromosomal Abnormalities | JAK 2 exon 12 and JAK 2 V617F | None | None |
References:
1. Choi CW, Bang S-M, Jang S, Jung CW, Kim H-J, Kim HY, et al. Guidelines for the management of myeloproliferative neoplasms. Korean J Intern Med [Internet]. 2015 Nov 30 [cited 2018 Jul 9];30(6):771–88. Available from: http://kjim.org/journal/view.php?doi=10.3904/kjim.2015.30.6.771
2. Schaub CR. Chronic Myeloproliferative disorders I: chronic myelogenous leukemia. In: Clinical hematology and fundamentals of hemostasis. 5th ed. Philadelphia: F.A. Davis Company; 2009. p. 371-84.
3. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. editors. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues Volume 2. 4th ed. International Agency for Research on Cancer (IARC); 2008.
4. Randolph TR. Myeloproliferative neoplasms. In: Rodak’s hematology clinical applications and principles. 5th ed. St. Louis, Missouri: Saunders; 2015. p.561-90.
5. Randolph TR. Myeloproliferative neoplasms. In: Clinical laboratory hematology. 3rd ed. New Jersey: Pearson; 2015. p. 450-78.