
2.6: Meatoplasty
- Page ID
- 15438

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
MEATOPLASTY
Tashneem Harris & Thomas Linder
Meatoplasty is an operative technique to widen the lateral cartilaginous part of the external auditory canal. Cartilage displaced anteriorly from the cavum conchae of the pinna, as well as bulky underlying soft tissue can cause narrowing of the lateral part of the ear canal.1 The aim of a meatoplasty is to enlarge the lumen of the entrance of the ear canal by removing the obstructing cartilage of cavum conchae as well as the underlying soft tissue.
Indications for surgery
There are 2 clinical scenarios where a meatoplasty may be required i.e. as an integral part of another otological procedure, or where there is lateral stenosis of the external ear canal.
As integral part of other otological procedures
- Open mastoidoepitympanectomy (MET): Meatoplasty is an essential routine step at the end of an open MET to provide easy access for cleaning and to assist with ventilation of the mastoid cavity. Failure to do an adequate meatoplasty will result in a lifelong problem of a chronic draining ear. This type of meatoplasty is discussed in the chapter Mastoidectomy and Epitympanectomy
- Tympanoplasty, canalplasty, removal of exostosis (bony canal wall intact): In these procedures it may be mandatory to perform a meatoplasty to improve intraoperative surgical exposure.
For lateral stenosis of the external ear canal: Meatoplasty becomes necessary when wax impaction as a result of canal stenosis causes recurrent otitis externa or hearing loss and requires frequent visits to an otolaryngologist.
Canal stenosis may be a result of:
- Congenital stenosis
- Otitis externa
- Iatrogenic following surgery or irradiation
- Trauma
M-Meatoplasty
The authors favor the M-Meatoplasty technique first described by Mirck in 1966.2
Anesthesia
- Antibiotic prophylaxis is not required
- It is performed under local anesthesia as an outpatient procedure
- The retro-auricular skin behind the conchal cartilage and the underlying soft tissue are infiltrated with 1% lidocaine and 1: 100 0000 adrenaline
- The skin and subperichondrial layer of the conchal bowl as well as the posterior ear canal wall are infiltrated with the same solution
Creating the skin flaps

Figure 1: Microhook retracting tragus
- An assistant retracts the tragus using a microhook to improve exposure (Figure 1)
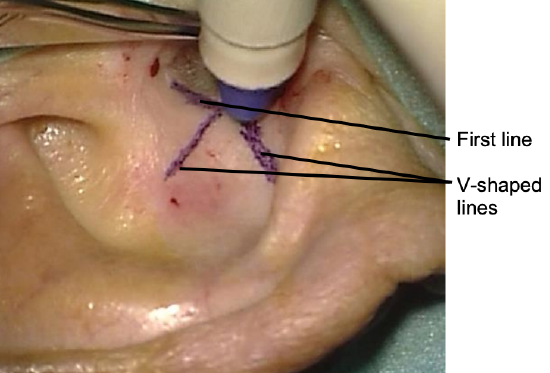
Figure 2: Marking the incisions
- The incisions are mapped out with a marking pen. (Figure 2)
- The first line is placed at the anterior border of the cavum conchae and at the entrance to the external auditory meatus (Figure 2)
- Two skin markings each measuring 1 cm in length and orientated as an inverted “V” are commenced in the center of the first skin marking (Figure 2)

Figure 3: Three skin incisions
- Skin incisions along these lines are made using a #15 blade resulting in three triangular skin flaps (Figure 3)
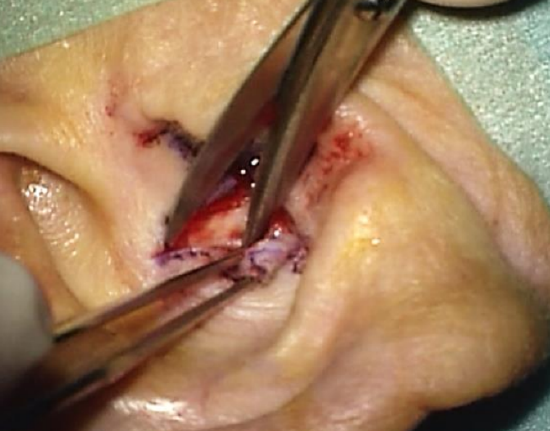
Figure 4: Elevating skin flaps
- Skin flaps are developed by separating the skin from the underlying cavum cartilage using sharp-pointed scissors (Figure 4)
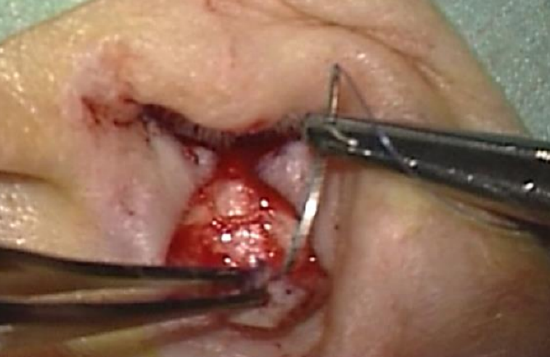
Figure 5: Guide suture being inserted into posterior flap
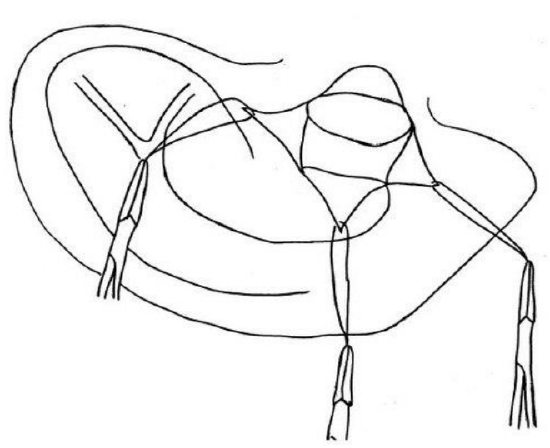
Figure 6: Guide sutures in all 3 flaps
- Guide sutures are placed at the apices of the 3 triangular skin flaps and mosquito clamps placed at the end of each suture to hold the skin flaps aside (Figure 5 & 6)
Excision of obstructing cavum cartilage and underlying soft tissue

Figure 7: Circle cut out of cavum cartilage
- A circle of about 1 cm diameter is cut out of the cavum cartilage (Figure 7)

Figure 8: Subcutaneous tissue is excised
- The underlying subcutaneous tissue is often bulky and is also excised (Figure 8)
V-Y plasty
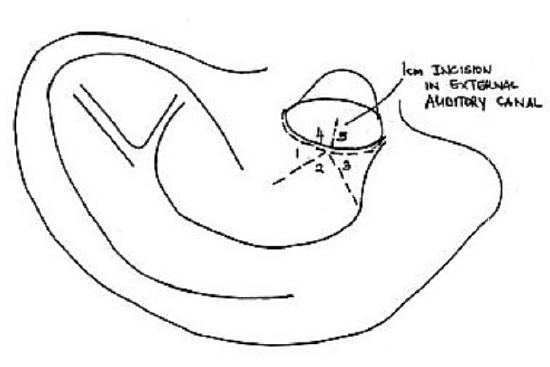
Figure 9
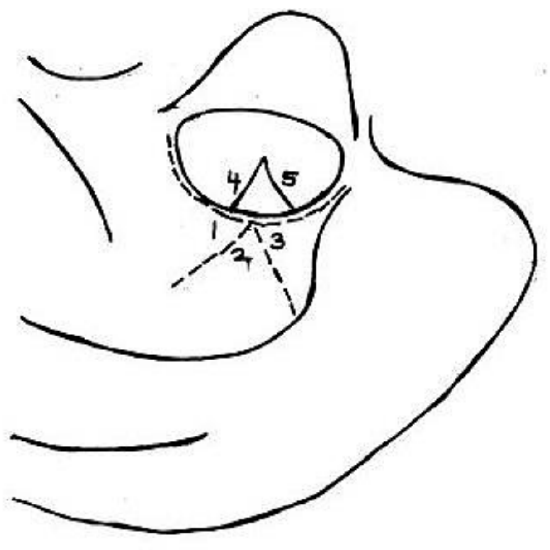
Figure 10
- A fourth 1 cm transverse incision is made in the posterior canal wall, thus creating two intrameatal skin flaps (Figure 9 & 10)
- 6/0 Nylon sutures are used to suture the skin flaps as follows:
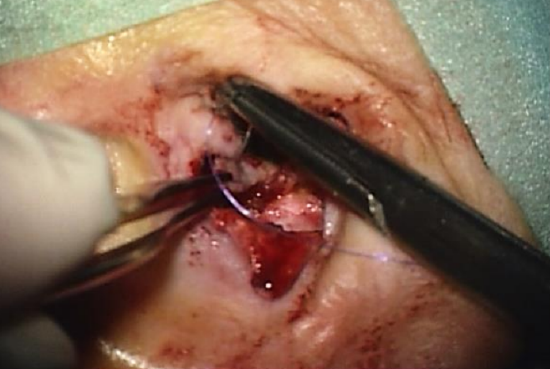
Figure 11: Sutures placed between ends of the intrameatal skin flaps

Figure 12: Sutures placed between ends of the intrameatal skin flaps
- Sutures are placed between the pointed ends of the two intrameatal skin flaps and either side of the base of the central triangular skin flap (Figures 11 & 12)

Figure 13: Suture placed at beginning of the intrameatal skin incision and apex of middle triangular skin flap
- A suture is placed at the beginning of the intrameatal skin incision and the apex of the middle triangular skin flap. This step widens the entrance of the external ear canal (Figure 13)
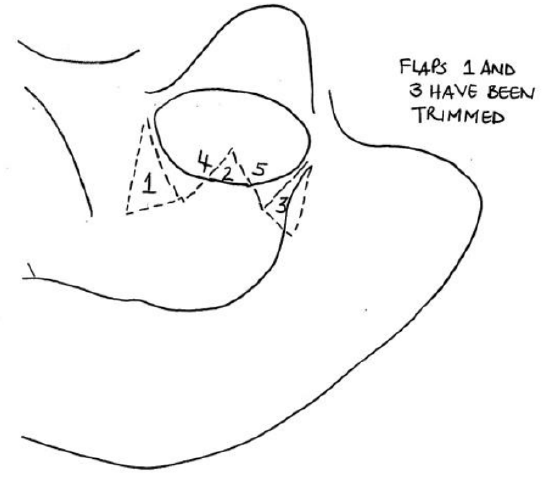
Figure 14

Figure 15

Figure 16
- The two redundant triangular skin flaps are excised, and sutures are placed between the remaining edges of skin of the cavum concha and the intrameatal skin flaps. (Figure 14,15,16)

Figure 17
- This results in a scar shaped like an “M” (Figure 17)
- A Terracortril (ointment containing a steroid and antiseptic agent) gauze is placed in the external ear canal for 5 days
- Sutures are removed after 1 week
References
- Fisch U, May J, Linder T. Tympanoplasty, Mastoidectomy, and Stapes Surgery. New York: Thieme; 2008.
- Mirck PG. The M-meatoplasty of the external auditory canal. Laryngoscope. 1996; 106(3):367-69.
Author
Tashneem Harris MBChB, FCORL, MMED (Otol), Fisch Instrument Microsurgical Fellow
ENT Specialist
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
harristasneem@yahoo.com
Senior Author
Prof Thomas Linder, M.D.
Chairman and Head of Department of Otorhinolaryngology, Head, Neck and Facial Plastic Surgery
Lucerne Canton Hospital, Switzerland
thomas.linder@ksl.ch
Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za