
9.5: Axial Muscles of the Abdominal Wall and Thorax
- Page ID
- 63430

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)- Identify the major skeletal muscles of the abdominal wall and thorax
- Identify the movements caused by these muscles
It is a complex job to balance the body on two feet and walk upright. The muscles of the vertebral column, thorax, and abdominal wall extend, flex, and stabilize different parts of the body’s trunk. The deep muscles of the core of the body help maintain posture as well as carry out other functions. The brain sends out electrical impulses to these various muscle groups to control posture by alternate contraction and relaxation. This is necessary so that no single muscle group becomes fatigued too quickly. If any one group fails to function, body posture will be compromised.
Muscles of the Abdomen
There are four pairs of abdominal muscles that cover the anterior and lateral abdominal region and meet at the anterior midline: the external obliques, the internal obliques, the transversus abdominis, and the rectus abdominis (Figure \(\PageIndex{1}\), Figure \(\PageIndex{2}\) and Table \(\PageIndex{1}\)).





There are three flat skeletal muscles in the antero-lateral wall of the abdomen. The external oblique, closest to the surface, extend inferiorly and medially, in the direction of sliding one’s four fingers into pants pockets. Perpendicular to it is the intermediate internal oblique, extending superiorly and medially, the direction the thumbs usually go when the other fingers are in the pants pocket. The deep muscle, the transversus abdominis, is arranged transversely around the abdomen, similar to the front of a belt on a pair of pants. This arrangement of three bands of muscles in different orientations allows various movements and rotations of the trunk. The three layers of muscle also help to protect the internal abdominal organs in an area where there is no bone.

| Muscle | Origin | Insertion | Movement | Image(s) |
|---|---|---|---|---|
| Internal oblique | Lumbar fascia, inguinal ligament and iliac crest | Linea alba, inferior rib surfaces 9-12, costal cartilages 8-10 |
Bilateral: Flexes vertebral column Unilateral: Lateral flexion and rotation of vertebral column |
 |
| External oblique | Ilium; ribs 5 - 12 | Ilium; linea alba; ribs 7 - 10 |
Bilateral: Flexes vertebral column Unilateral: Lateral flexion and rotation of vertebral column |
 |
| Rectus abdominis | Pubis | Ribs 5 and 7; sternum | Flexion of vertebral column |  |
| Transverse abdominus | Ilium; ribs 5 - 10 | Linea alba; pubis; sternum | Squeezing abdomen during forceful exhalations, defecation, urination, and childbirth |  |
Physical Therapist and Physical Therapy Assistant
Those who have a muscle or joint injury will most likely be sent to a physical therapist (PT) after seeing their regular doctor. PTs have a master’s degree or doctorate, and are highly trained experts in the mechanics of body movements. Many PTs also specialize in sports injuries.
If you injured your shoulder the first thing a physical therapist would do during your first visit is to assess the functionality of the joint. The range of motion of a particular joint refers to the normal movements the joint performs. The PT will ask you to abduct and adduct, circumduct, and flex and extend the arm. The PT will note the shoulder’s degree of function, and based on the assessment of the injury, will create an appropriate physical therapy plan. This plan can involve visits to the clinic to work with a Physical Therapy Assistant (PTA) who will help guide you through the appropriate exercises. Most likely, you also will be instructed to do a series of exercises to continue the therapy at home, followed by icing to decrease inflammation and swelling, which will continue for several weeks.
When physical therapy is complete, the PT will do an exit exam and send a detailed report on the improved range of motion and return of normal limb function to your doctor. Gradually, as the injury heals, the shoulder will begin to function correctly. Both Physical Therapists and Physical Therapy Assistants work closely with patients to help them get back to their normal level of physical activity.

 Sierra Stout, a physical therapist with Global Outreach Doctors teaches a mobility exercise to a boy with scoliosis at a temporary medical treatment site in Point Fortin, Trinidad, Sept. 7, 2019. Comfort is working with health and government partners in Central America, South America, and the Caribbean to provide care on the ship and at land-based medical sites, helping to relieve pressure on national medical systems. (U.S. Navy photo by Mass Communication Specialist Seaman Jordan R. Bair/Released to Public Domain)\
Sierra Stout, a physical therapist with Global Outreach Doctors teaches a mobility exercise to a boy with scoliosis at a temporary medical treatment site in Point Fortin, Trinidad, Sept. 7, 2019. Comfort is working with health and government partners in Central America, South America, and the Caribbean to provide care on the ship and at land-based medical sites, helping to relieve pressure on national medical systems. (U.S. Navy photo by Mass Communication Specialist Seaman Jordan R. Bair/Released to Public Domain)\Muscles of Respiration
The muscles of the chest serve to facilitate breathing by changing the size of the thoracic cavity (Table \(\PageIndex{2}\)). Movement of the ribs in a superior direction is called elevation of the ribs at both the sternocostal and vertebrocostal joints. Your chest expands drawing air into your lungs. Movement of the ribs in an inferior direction is called depression of the ribs, at the same joints. For your resting breathing no muscular contraction is necessary due to elasticity, but for deep exhalation muscles will pull the ribs downward and inward to decrease the size of the thoracic cavity.
| Muscle | Origin | Insertion | Movement |
|---|---|---|---|
| Diaphragm | Lumbar vertebrae; ribs 6 - 12; sternum | Central tendon | Inhalation; compression of abdominopelvic cavity |
| Internal intercostals | Rib inferior to each intercostal muscle | Rib superior to each intercostal muscle | Forced exhalation |
| External intercostals | Rib superior to each intercostal muscle | Rib inferior to each intercostal muscle | Inhalation; elevation of ribs |
| Scalenes | Transverse processes of cervical vertebrae | Superior surface of 1st and 2nd rib | Elevate 1st and 2nd rib during forced inhalation |
The change in volume of the thoracic cavity during breathing is due to the alternate contraction and relaxation of the diaphragm. It separates the thoracic and abdominal cavities, and is dome-shaped at rest (Figure \(\PageIndex{3}\)). The superior surface of the diaphragm is convex, creating the elevated floor of the thoracic cavity. The inferior surface is concave, creating the curved roof of the abdominal cavity. Defecating, urination, and even childbirth involve cooperation between the diaphragm and abdominal muscles (this cooperation is referred to as the “Valsalva maneuver”). You hold your breath by a steady contraction of the diaphragm; this stabilizes the volume and pressure of the peritoneal cavity. When the abdominal muscles contract, the pressure cannot push the diaphragm up, so it increases pressure on the intestinal tract (defecation), urinary tract (urination), or reproductive tract (childbirth).

The central of the diaphragm is its tendon. To the sides of the tendon are the skeletal muscle portions of the diaphragm, which insert into the tendon while having a number of origins including the xiphoid process of the sternum anteriorly, the inferior six ribs and their cartilages laterally, and the lumbar vertebrae and 12th ribs posteriorly. The central tendon of the diaphragm also includes three openings for the passage of structures between the thorax and the abdomen such as the inferior vena cava, aorta, and the esophagus.
Assisting the diaphragm during deep breathing are two sets of muscles, called intercostal muscles, that span each of the intercostal spaces. The principal role of the intercostal muscles is to assist in breathing by changing the dimensions of the rib cage (Figure \(\PageIndex{4}\)).


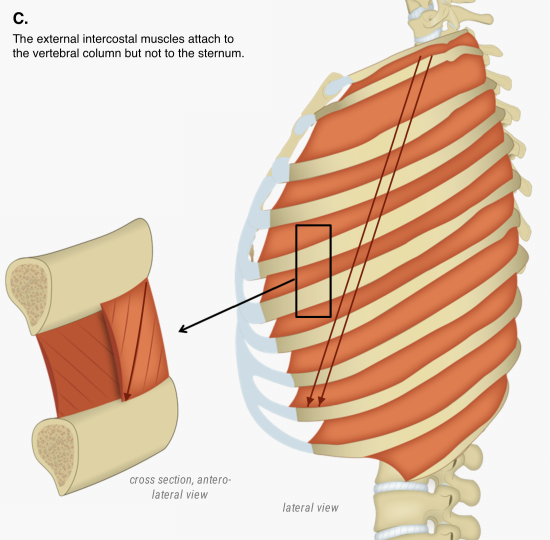
The 11 pairs of superficial external intercostal muscles aid in inspiration of air during breathing because when they contract, they raise the ribs, which expands the thoracic cavity. The 11 pairs of internal intercostal muscles, just deep to the externals, are used for forced (deep) expiration because they draw the ribs together to constrict the rib cage. The movement of the ribs caused by the intercostals is visualized using to analogies: a bucket handle and a pump handle.
To view animations of the movements of the thoracic cage during inhalation and exhalation visit UBC's Clinical Anatomy and select the pages "bucket handle effect" and "pump handle effect".

Muscles of the Pelvic Floor
The pelvic floor is a muscular sheet that defines the inferior portion of the pelvic cavity. The pelvic diaphragm, spanning anteriorly to posteriorly from the pubis to the coccyx, comprises the levator ani and the ischiococcygeus. Its openings include the anal canal and urethra, and the vagina in females.
The large levator ani consists of two skeletal muscles, the pubococcygeus and the iliococcygeus (Figure \(\PageIndex{5}\)). The levator ani is considered the most important muscle of the pelvic floor because it supports the pelvic viscera. It resists the pressure produced by contraction of the abdominal muscles so that the pressure is applied to the colon to aid in defecation and to the uterus to aid in childbirth (assisted by the ischiococcygeus, which pulls the coccyx anteriorly). This muscle also creates skeletal muscle sphincters at the urethra and anus. The posterior muscle of the of the pelvic floor is the coccygeus.


Concept Review
Made of skin, fascia, and four pairs of muscle, the anterior abdominal wall protects the organs located in the abdomen and moves the vertebral column. These muscles include the rectus abdominis, which extends through the entire length of the trunk, the external oblique, the internal oblique, and the transversus abdominus. The quadratus lumborum forms the posterior abdominal wall.
The muscles of the thorax play a large role in breathing, especially the dome-shaped diaphragm. When it contracts and flattens, the volume inside the pleural cavities increases, which decreases the pressure within them. As a result, air will flow into the lungs. The external and internal intercostal muscles span the space between the ribs and help change the shape of the rib cage and the volume-pressure ratio inside the pleural cavities during inspiration and expiration.
The perineum muscles play roles in urination in both sexes, ejaculation in men, and vaginal contraction in women. The pelvic floor muscles support the pelvic organs, resist intra-abdominal pressure, and work as sphincters for the urethra, rectum, and vagina.
Review Questions
Query \(\PageIndex{1}\)
Critical Thinking Questions
Query \(\PageIndex{2}\)
Query \(\PageIndex{3}\)
Glossary
Query \(\PageIndex{4}\)
Contributors and Attributions
OpenStax Anatomy & Physiology (CC BY 4.0). Access for free at https://openstax.org/books/anatomy-and-physiology