
17.3: Cardiac Muscle and Electrical Activity
- Page ID
- 63479
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
- Describe the structure of cardiac muscle tissue and cells
- Identify and describe the components of the conducting system that distributes electrical impulses through the heart
Recall that cardiac muscle shares a few characteristics with both skeletal muscle and smooth muscle, but it has some unique properties of its own. Not the least of these exceptional properties is its ability to initiate an electrical potential at a fixed rate that spreads rapidly from cell to cell to trigger the contractile mechanism. This property is known as autorhythmicity. Skeletal muscle can not do this. Even though cardiac muscle has autorhythmicity, heart rate is modulated by the endocrine and nervous systems.
Structure of Cardiac Muscle Tissue and Cells
Compared to the giant cylinders of skeletal muscle, cardiac muscle cells, or cardiomyocytes, are considerably shorter with much smaller diameters. Cardiac muscle also demonstrates striations, the alternating pattern of dark A bands and light I bands attributed to the precise arrangement of the myofilaments and fibrils that are organized in sarcomeres along the length of the cell (Figure \(\PageIndex{1}\).a). These contractile elements are virtually identical to skeletal muscle. T (transverse) tubules penetrate from the surface plasma membrane, the sarcolemma, to the interior of the cell, allowing the electrical impulse to reach the interior. The T tubules are only found at the Z discs, whereas in skeletal muscle, they are found at the junction of the A and I bands. Therefore, there are one-half as many T tubules in cardiac muscle as in skeletal muscle. In addition, the sarcoplasmic reticulum of cardiomyocytes stores few calcium ions, so most of the calcium ions must come from outside the cells. The result is a slower onset of contraction. Mitochondria are plentiful, providing energy for the cross-bridge cycling responsible for contractions of the heart. Typically, cardiomyocytes have a single, central nucleus, but two or more nuclei may be found in some cells. Cardiac muscle undergoes aerobic respiration patterns, primarily metabolizing lipids and carbohydrates. Myoglobin, lipids, and glycogen are all stored within the cytoplasm.
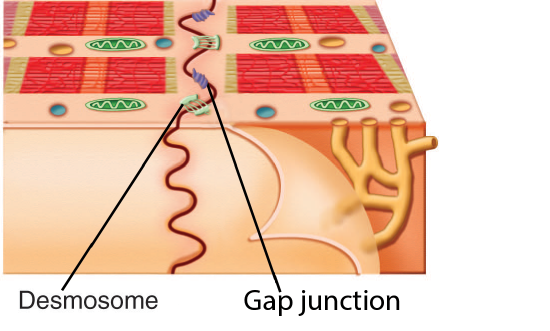
Cardiac muscle cells branch freely. A junction between two adjoining cells is marked by a critical structure called an intercalated disc, which helps support the synchronized contraction of the muscle and structurally links the cells together (Figure \(\PageIndex{1}\)). Intercalated discs are formed by regions of sarcolemma with specialized integral membrane proteins. These form desmosomes, fasciae adherens, and large numbers of gap junctions. Desmosomes and fasciae adherens anchor the cells together. Fasciae adherens also anchor actin filaments of the sarcomere directly to the sarcolemma. Gap junctions allow the passage of ions from cell-to-cell through their sarcoplasm, a feature essential to producing synchronized contractions (Figure \(\PageIndex{1}\)). Intercellular connective tissue also helps to bind the cells together. The importance of strongly binding these cells together is necessitated by the forces exerted by contraction; unlike skeletal muscle in which cells are the length of the organ to pull collectively on a bone via collagenous connective tissue attachments, smaller cardiac muscle cells pull on each other and ultimately on the dense connective tissue of the cardiac skeleton when they contract.

There are two major types of cardiac muscle cells: myocardial contractile cells and myocardial conducting cells. The myocardial contractile cells constitute the bulk (99 percent) of the cells in the myocardium of the atria and ventricles. Myocardial contractile cells are autorhythmic, but they are primarily responsible for the strong, synchronized contractions necessary to pump blood through the body. The myocardial conducting cells (1 percent of the cells) are generally much smaller than the contractile cells and have fewer myofibrils for contraction. Myocardial conducting cells are specialized to initiate and propagate the electrical activity that travels throughout the heart and triggers the contractions of the myocardial contractile cells that propel the blood. If embryonic heart cells are separated into a Petri dish and kept alive, each is capable of generating its own electrical impulse (also referred to as a wave of depolarization or an action potential) that is followed by contraction (the capability that is described as autorhythmicity). When two independently beating embryonic cardiac muscle cells are placed together, the cell with the faster inherent rate sets the pace, and the impulse spreads from the faster to the slower cell to trigger a contraction in such rapid succession that they appear to contract in unison. As more cells are joined together, the fastest cell continues to assume control of the rate. A fully developed adult heart maintains the capability to generate its own electrical activity, triggered by the fastest cells. The fastest cells are the myocardial conducting cells. The slower cells (which are also stronger) are the myocardial contractile cells.
Repair and Replacement of Cardiac Muscle
Damaged cardiac muscle cells have extremely limited abilities to repair themselves or to replace dead cells via mitosis. Recent evidence indicates that at least some stem cells remain within the heart that continue to divide and at least potentially replace these dead cells. However, newly formed or repaired cells are rarely as functional as the original cells, and cardiac function is reduced. In the event of a heart attack or myocardial infarction (MI), dead cells are often replaced by patches of scar tissue in a process called fibrosis. Autopsies performed on individuals who had successfully received heart transplants show some proliferation of original cells. If researchers can unlock the mechanism that generates new cells and restore full mitotic capabilities to heart muscle, the prognosis for heart attack survivors will be greatly enhanced. To date, myocardial cells produced within the patient (in situ) by cardiac stem cells seem to be nonfunctional, although those grown in Petri dishes (in vitro) do beat. Perhaps soon this mystery will be solved, and new advances in treatment will be commonplace.
Conducting System of the Heart
The myocardial conducting cells are concentrated in specific areas of the heart that make up the Conducting System. The components of the cardiac conducting system include the sinoatrial node, the atrioventricular node, the atrioventricular bundle, the atrioventricular bundle branches, and the Purkinje fibers (Figure \(\PageIndex{3}\)).

Figure \(\PageIndex{3}\): Conducting System of the Heart. Specialized conducting components of the heart include the sinoatrial node, the atrioventricular node, the atrioventricular bundle, the right and left bundle branches, and the Purkinje fibers. (Image credit: "Conducting System of the Heart" by BlueLink is licensed under CC BY-NC 4.0 with notification of the original authors.)
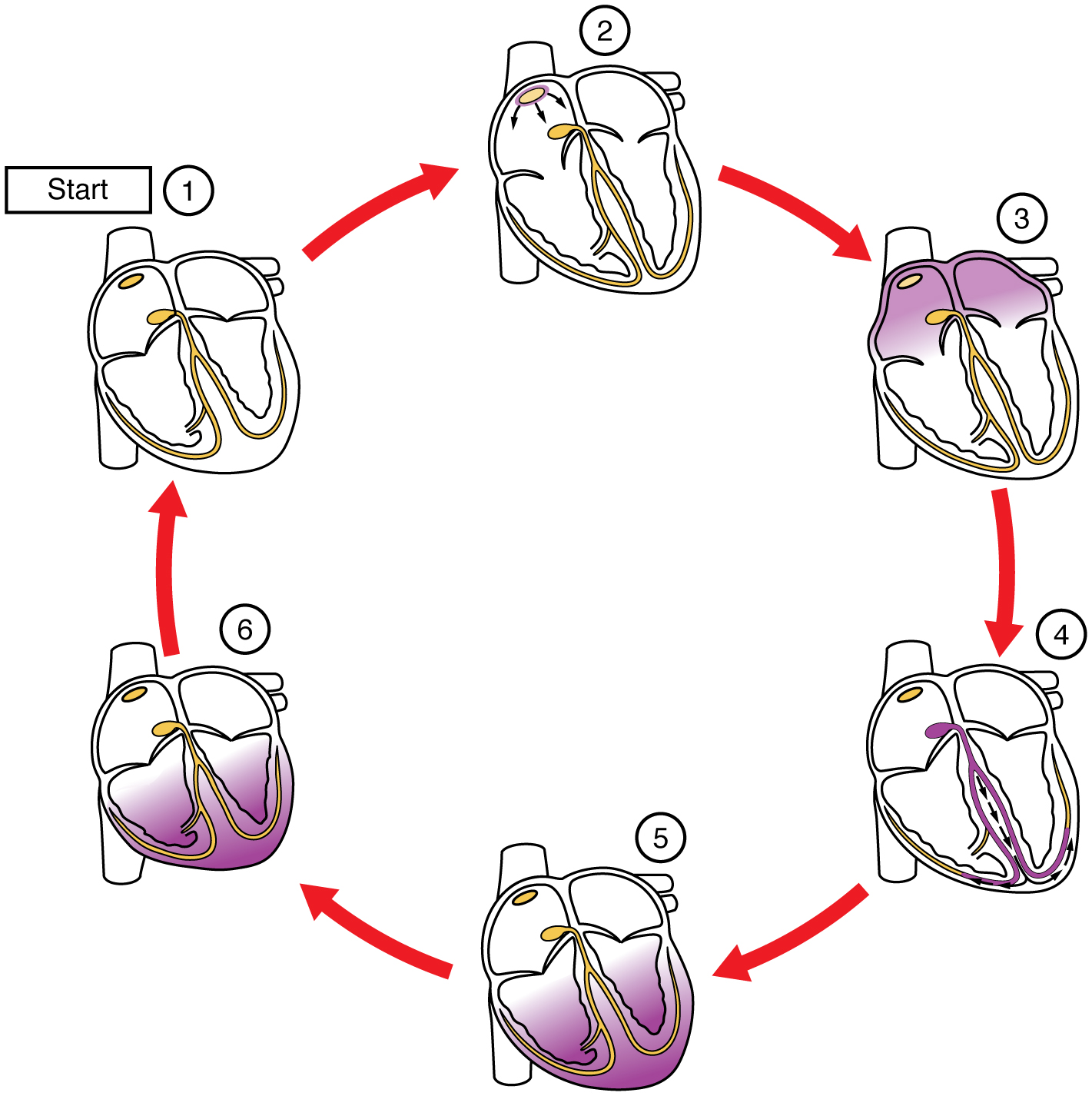
Normal cardiac rhythm is established by the sinoatrial (SA) node, a specialized clump of myocardial conducting cells located in the posterosuperior walls of the right atrium in close proximity to the orifice of the superior vena cava. The myocardial conducting cells of the SA node have the highest inherent rate of electrical signal initiation, so the SA node is known as the pacemaker of the heart. It initiates the sinus rhythm, or normal electrical pattern followed by contraction of the heart. This impulse spreads from its initiation in the SA node throughout the atria and to the atrioventricular node. As the wave spreads across the atria they will contract and push blood into the ventricles.The atrioventricular (AV) node is a second clump of specialized myocardial conducting cells, located in the inferior portion of the right atrium within the atrioventricular septum. The septum contains the dense irregular connective tissue of the cardiac skeleton that prevents the impulse from spreading directly to the ventricles without passing through the AV node.
Arising from the AV node, the atrioventricular bundle, or bundle of His, proceeds into the interventricular septum before dividing into two atrioventricular bundle branches, commonly called the left and right bundle branches. The left bundle branch supplies the left ventricle, and the right bundle branch the right ventricle. Both descend and reach the apex of the heart where they connect with the Purkinje fibers (see Figure \(\PageIndex{3}\)), which then spread the impulse to the myocardial contractile cells in the ventricles. They extend throughout the myocardium from the apex of the heart toward the atrioventricular septum and the base of the heart at the top of the ventricles. Figure \(\PageIndex{4}\) show the spread of the electrical wave through these structures and the myocardial contractile cells.
Cardiovascular System: Conduction Block
A heart block refers to an interruption in the normal conduction pathway. The nomenclature for these is very straightforward:
- SA nodal blocks occur within the SA node.
- AV nodal blocks occur within the AV node.
- Infra-Hisian blocks involve the bundle of His.
- Bundle branch blocks occur within either the left or right atrioventricular bundle branches.
Clinically, the most common types are the AV nodal and infra-Hisian blocks.
When arrhythmias become a chronic problem, the heart maintains the rhythm of the AV node. In order to speed up the heart rate and restore full sinus rhythm, a cardiologist can implant an artificial pacemaker, which delivers electrical impulses to the heart muscle to ensure that the heart continues to contract and pump blood effectively.
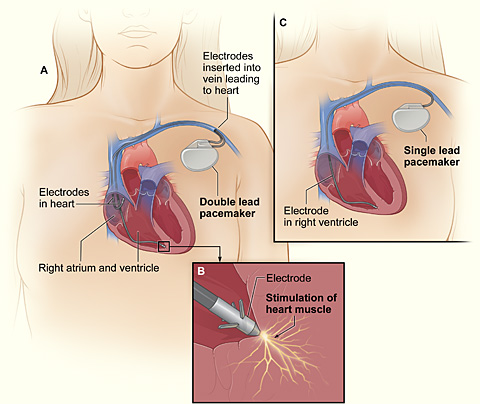
A traditional pacemaker generator is placed outside of the heart, either in the chest or abdomen. It connects via wires to electrodes inside one to three heart chambers: single- and double-lead pacemakers send pulses to the right side of the heart and biventricular pacemakers sends pulses to both ventricles and an atrium. Wireless, or leadless, pacemakers are smaller than traditional types because the pulse generator and electrodes are all in one device. This type of pacemaker is placed inside the heart from where it then sends pulses to the right ventricle.
Concept Review
The heart is regulated by both neural and endocrine control, yet it initiates its own electrical impulse at an intrinsic rate followed by muscular contraction. The myocardial conducting cells within the heart establish the heart rate and transmit it through the myocardium. The myocardial contractile cells contract and propel the blood. The normal path of transmission for the conductive cells is the sinoatrial (SA) node, atrioventricular (AV) node, atrioventricular (AV) bundle, bundle branches, and Purkinje fibers.
Review Questions
Q. Which of the following distinguishes cardiac muscle cells from skeletal muscle cells?
A. Only cardiac muscle contains a sarcoplasmic reticulum.
B. Only cardiac muscle has striations.
C. Only cardiac muscle is capable of autorhythmicity.
D. Only cardiac muscle has a high concentration of mitochondria.
- Answer
-
Answer: C
Q. Which component of the heart's conducting system is considered the pacemaker of the heart?
A. atrioventricular node
B. atrioventricular bundle
C. bundle branches
D. sinoatrial node
- Answer
-
Answer: D
Critical Thinking Questions
Q. How do intercalated discs aid contraction of the heart?
- Answer
-
A. Intercalated discs consist of desmosomes, fasciae adherens, and gap junctions. Desmosomes and fasciae adherens create strong connections between adjacent cardiac muscle cells that will contract against one another. Gap junctions within the intercalated discs allow impulses to spread from one cardiac muscle cell to another, allowing ions to flow between adjacent cells, propagating the electrical impulse to contract, and ensuring coordinated contractions.
Glossary
- artificial pacemaker
- medical device that transmits electrical signals to the heart to ensure that it contracts and pumps blood to the body
- atrioventricular bundle
- (also, bundle of His) group of specialized myocardial conductile cells that transmit the impulse from the AV node through the interventricular septum; form the left and right atrioventricular bundle branches
- atrioventricular bundle branches
- (also, left or right bundle branches) specialized myocardial conductile cells that arise from the bifurcation of the atrioventricular bundle and pass through the interventricular septum; lead to the Purkinje fibers and also to the right papillary muscle via the moderator band
- atrioventricular (AV) node
- clump of myocardial cells located in the inferior portion of the right atrium within the atrioventricular septum; receives the impulse from the SA node, pauses, and then transmits it into specialized conducting cells within the interventricular septum
- autorhythmicity
- ability of cardiac muscle to initiate its own electrical impulse that triggers the mechanical contraction that pumps blood at a fixed pace without nervous or endocrine control
- bundle of His
- (also, atrioventricular bundle) group of specialized myocardial conductile cells that transmit the impulse from the AV node through the interventricular septum; form the left and right atrioventricular bundle branches
- heart block
- interruption in the normal conduction pathway
- intercalated disc
- physical junction between adjacent cardiac muscle cells; consisting of desmosomes, specialized linking proteoglycans, and gap junctions that allow passage of ions between the two cells
- myocardial conducting cells
- specialized cells that transmit electrical impulses throughout the heart and trigger contraction by the myocardial contractile cells
- myocardial contractile cells
- bulk of the cardiac muscle cells in the atria and ventricles that conduct impulses and contract to propel blood
- pacemaker
- cluster of specialized myocardial cells known as the SA node that initiates the sinus rhythm
- Purkinje fibers
- (also, subendocardial conducting network) specialized myocardial conducting fibers that arise from the bundle branches and spread the impulse to the myocardial contraction fibers of the ventricles
- sinoatrial (SA) node
- known as the pacemaker, a specialized clump of myocardial conducting cells located in the superior portion of the right atrium that has the highest inherent rate of depolarization that then spreads throughout the heart
- sinus rhythm
- normal contractile pattern of the heart
Contributors and Attributions
OpenStax Anatomy & Physiology (CC BY 4.0). Access for free at https://openstax.org/books/anatomy-and-physiology