
10.9: Large Intestine
- Page ID
- 84063

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
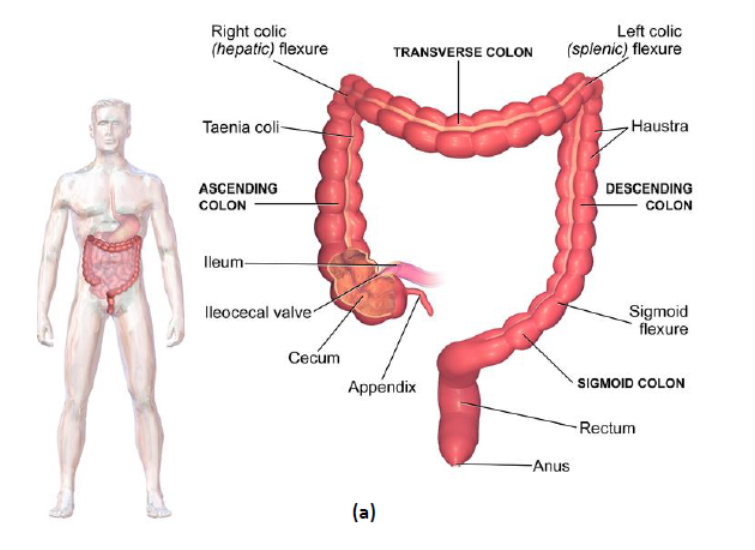
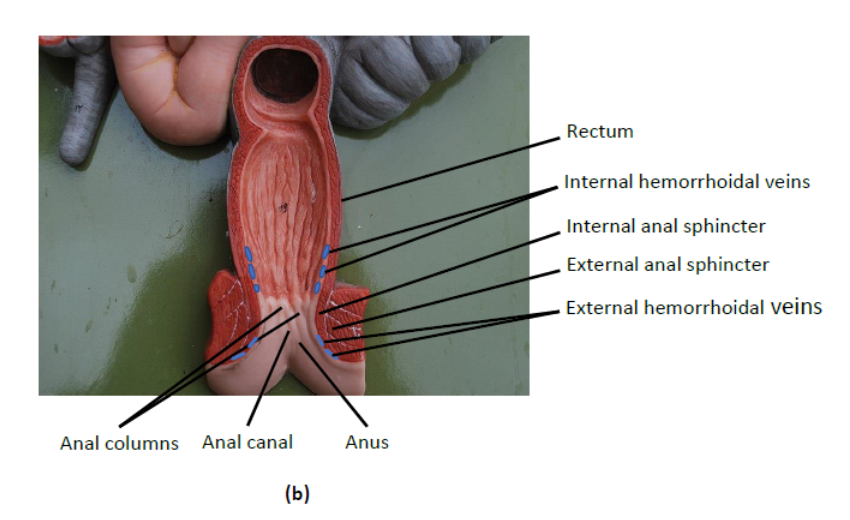
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)The large intestine, which is about 1.5 meters (5 feet) long, extends from the end of the small intestine to the end of the GI tract (Figure 10.1 and Figure 10.4). Most of the large intestine is referred to as the colon. The last section of the colon has an S shape and is called the sigmoid colon. The sigmoid colon leads into the final segment of the large intestine, the rectum (Figure 10.4b). The rectum, which is several centimeters long, leads into a very short passage called the anal canal. This canal ends at the anus, which is the opening from the large intestine to the outside of the body. The appendix is a fingerlike projection jutting out from the colon just below the junction of the small intestine and the colon.
Secretion and Absorption
A smooth layer of cells lines the inner surface of the large intestine. Many of these cells secrete a lubricating mucus that aids the passage of materials. The materials in the large intestine are called feces. Many other lining cells absorb water, minerals, and vitamin K from the feces. Much of the vitamin K is produced by bacteria that normally reside in the feces. The absorption of most of the water and minerals from the feces is essential for maintaining adequate supplies of these substances for body cells. Vitamin K is needed to form blood-clotting materials. Absorbed substances pass into the blood.
Movements
Within the wall of the colon, some smooth muscle lies in three narrow ribbonlike bands (teniae coli). These bands run parallel along the length of the colon and are nearly evenly spaced around its circumference. The remainder of the smooth muscle lies in rings spaced little more than 2.5 cm (1 inch) from each other. This leaves regularly arranged patches of the colon wall with little muscular support. Since these patches (haustra) are weaker areas, they bulge outward.
As in the stomach and small intestine, smooth muscle in the colon churns materials and moves them along by peristalsis. The activity of this smooth muscle is encouraged by exercise and other physical activity. The muscle has diminished activity when a person is sedentary.
The churning action assists in the absorption of useful substances by mixing the feces and bringing them into contact with the lining of the large intestine. The absorption of water causes the feces to change in consistency from a liquid to a soft semisolid. As more indigestible material continues to enter the large intestine from the small intestine, the total amount of feces gradually increases.
The accumulation of feces causes the pressure inside the large intestine to increase, and the intestine is stretched outward. These changes cause neurons in the intestinal wall to activate large-scale peristalsis (mass peristalsis) throughout the length of the large intestine. Eating a meal or having stimulatory chemicals in the large intestine can also reflexively activate mass peristalsis, which pushes feces into the rectum.
Defecation
Initially, the feces are prevented from passing out of the rectum through the anus by two rings of muscle in the anal canal. The inner ring (internal sphincter) is made of smooth muscle and is controlled by reflexes (Figure 10.4b). The outer ring (external sphincter) is made of skeletal muscle and is under voluntary control. These muscular rings cause retention of feces because they are usually in a state of contraction, which closes the passage through the anal canal and the anus. The internal sphincter provides about 85 percent of the force needed to retain feces, and the external sphincter provides the remaining 15 percent.
As the quantity of feces in the rectum increases, the rectum is stretched outward. When it stretches nearly as far as it can, further influx of feces causes pressure in the rectum to increase dramatically. Sensory neurons in the rectum are stimulated, and the person begins to perceive the need to pass the feces. The stretching and rise in pressure also cause rectal neurons to produce reflexive relaxation of the internal sphincter muscle, and there is an increase in the perception that elimination of feces is needed. Then only the external sphincter prevents the exit of feces through the anus. It is easier for the external sphincter to retain feces with a more solid consistency than to retain less solid or more watery feces.
At this point the individual can prevent the release of feces by voluntarily continuing contraction of the external sphincter. Alternatively, the person can cause the external sphincter to relax. Then the pressure in the rectum will begin to push feces out of the body through the anal canal and the anus. This action is often accompanied by reflexive peristalsis in the large intestine and voluntary contraction of the abdominal muscles. Since these additional contractions increase pressure in the large intestine, they assist in pushing feces through the anus.
As the rectum empties, the stretching and pressure in the rectum subside. Then reflexive contraction of muscles in and around the anal canal eliminates the feces still in the canal. Finally, the internal sphincter contracts again, and elimination of feces stops. Elimination of feces is often called a bowel movement or defecation.
Voluntary contraction of the external sphincter can delay defecation for an extended period. If a sizable mass of feces is retained in the rectum, the rectal muscles relax, allowing the rectum to stretch outward and the pressure to drop. As a result, the urge to defecate subsides until more feces enter the rectum and the pressure rises again. However, control of the external sphincter is retained only as long as the pressure in the rectum remains low or moderate. Very great pressure in the rectum causes uncontrollable reflexive relaxation of the external sphincter, and defecation occurs.
Appendix
The appendix is a small and unimportant part of the large intestine (Figs. 10.1 and 10.4a). Though its size and shape vary considerably from person to person, typically the appendix looks like a slender finger approximately 5 to 7 cm (2 to 3 inches) in length. The narrow passage within the appendix has one opening, which leads into the colon, and the wall of the appendix contains many lymph nodes.
In humans the appendix has no role in digestion. Normally, no materials from the intestine enter the appendix. Like all other lymph nodes, its lymph nodes help prevent the spread of infection and serve as part of the immune system.
Age Changes
With aging, the lining of the large intestine becomes somewhat thinner and less mucus is secreted. These changes may be due partially to arteriosclerosis in small arteries that serve the large intestine. There is also a slight shrinkage of smooth muscle in the large intestine. Usually the extent of these changes is not great enough to alter the functioning of the large intestine significantly.
Movements
An age change in the colon that may produce important consequences in some older individuals is a decrease in the responsiveness of the smooth muscle to neuron messages. This tends to delay the onset of peristalsis, and more time is needed for feces to pass through the large intestine.
When feces spend more time in the large intestine, more water is absorbed, and the feces become firmer and more difficult to move. Bowel movements occur less frequently, and defecation becomes more difficult. If periods between bowel movements become abnormally long or defecation requires excessive straining, the abnormal condition called constipation has developed.
Defecation
Aging and other age-related factors cause three significant changes in the rectum. The other factors include surgery in the rectal area, forced bowel movements, and childbearing and reduced estrogen levels. One resulting change in the rectum is an increase in the amount of fibrous tissue in the walls, which reduces the amount of rectal stretching as feces enter. A second change is a decline in the strength of contraction of the internal sphincter. The third change is a decrease in the motor neurons controlling the external sphincter.
Each of these changes reduces the ability of the sphincter muscles to delay defecation until it is appropriate. Though inappropriate fecal elimination can happen to anyone, having such occurrences on a regular or frequent basis is abnormal. When inappropriate elimination of feces happens at least once a month, the condition is called fecal incontinence.
Abnormal Changes
Constipation
Though age has little effect on the structure and functioning of the large intestine, many aging people develop one or more abnormalities. One of the most common conditions is constipation. Generally, constipation occurs when bowel movements occur less than three times a week. However, since there is great variation in the frequency of bowel movements among individuals, better indicators are having an unusual decrease in the frequency of bowel movements and needing to strain excessively during defecation.
Although the incidence of constipation rises with age, it is difficult to estimate its actual frequency because of preconceived notions about how frequently bowel movements should occur and the use of laxatives. (A laxative is a substance that is ingested to promote bowel movements.) However, regardless of the confusion over the precise incidence, constipation is a problem for many elderly people. A variety of factors can contribute to the onset of constipation, including inadequate fluid intake, inactivity, delayed defecation, inadequate or excess fiber intake, and laxatives.
One of the most abundant types of dietary fiber is cellulose, which is contained in fruits and vegetables. Bran also contains much cellulose. Cellulose is especially important because it binds much water and thus makes feces large in volume but soft in consistency. Large soft feces stimulate peristalsis and are easy to move and eliminate by defecation.
Laxatives come in a variety of forms and work in different ways. Among the different types are fiber supplements, oils, magnesium salts, and intestinal stimulants.
Constipation can lead to significant discomfort and many complications. The discomfort may include indigestion, a bloated feeling, pain and embarrassment from intestinal gas, and difficulty defecating. One complication is an increased risk of future constipation. This occurs because the sensitivity of rectal sensory neurons declines when the rectum is stretched for long periods. With reduced rectal sensitivity, the urge to defecate and the reflexes involved in defecation are suppressed and defecation is delayed. Additional complications include diarrhea, fecal incontinence, diverticulosis, hemorrhoids, and cancer, which are discussed below. Still other complications include obstruction of the large intestine, formation and absorption of toxins, infections, difficulty urinating, irregular heart functioning, and heart attack.
Since constipation is not an age change and since its causes are largely known and controllable, much can be done to prevent its occurrence. Preventive measures are based on minimizing factors that contribute to constipation. Special consideration is required to ensure that toilet facilities and assistance are readily available to those who are disabled.
Treatments for people with constipation are derived from these preventive measures. They include gradually increasing fluid intake, physical activity, and dietary fiber. Regular bowel movements can be promoted by scheduling regular visits to the toilet. Laxatives should be used only when other treatments fail since regular laxative use promotes constipation and can cause other serious side effects, such as dehydration, vitamin deficiencies, and mineral imbalances.
Some cases of constipation can be relieved by using suppositories containing substances that stimulate mass peristalsis. These suppositories are inserted into the rectum through the anus. Other cases of constipation can be relieved by enemas. If feces are especially hard and difficult to pass, it may be necessary for a physician to remove them through the anus.
Diarrhea
A second abnormality of the large intestine that is important in elderly populations is diarrhea. Diarrhea is characterized by the presence of more than three relatively liquid and voluminous bowel movements a day. Causes of diarrhea are listed in Table 10.1.
Table 10.1 Causes of Diarrhea
- Antacids containing magnesium
- Toxins produced by bacteria in spoiled food or contaminated water
- Laxatives
- Certain antibiotics and other medications
- Constipation
- Toxins produced by bacteria in the small intestine
- Viral infections in the GI tract
- Diseases of the large intestine (e.g., ulcerative colitis)
- Emotional disturbances
- Cancer of the large intestine
- Cancer of other body organs (e.g., pancreas)
One of the most serious consequences of diarrhea is an abnormally high loss of water and minerals. When body fluid levels drop, maintaining adequate blood pressure and blood flow to vital organs such as the heart, brain, and kidneys becomes difficult. These organs begin to malfunction and fail. Disturbances in mineral homeostasis can also adversely affect the heart and brain and disrupt muscle functioning.
Three factors make these outcomes from diarrhea especially likely among the elderly. First, many elderly people already have reduced blood flow to the heart, brain, and kidneys because of atherosclerosis. Second, aging reduces the ability of the kidneys to maintain adequate fluid levels. Third, the decrease in thirst sensation caused by aging reduces the urge to replace fluids by drinking. Individuals who take medications that increase fluid output by the kidneys (i.e., diuretics) or that lower blood pressure have an even greater risk of developing circulatory failure.
Another important consequence of diarrhea is temporary loss of the ability to retain feces when defecation is inappropriate. An individual of any age who has diarrhea may have difficulty retaining feces because of their liquid consistency and large volume and because of the strong urge to release them. Older individuals have even greater difficulty because of age changes that weaken and reduce control of the anal sphincters. Any other condition that reduces conscious control of muscles or delays access to toilet facilities further increases the risk of unwanted defecation when a person has diarrhea. Examples of such conditions that are more prevalent among older individuals include CNS disorders (e.g., Alzheimer's disease) and physical disabilities (e.g., fractures, arthritis). Repeated incidents of diarrhea can cause fecal incontinence (see below).
Many cases of diarrhea can be prevented by avoiding factors that cause diarrhea. A main aspect of treatment is replacing lost fluids and minerals. However, care must be taken to avoid introducing excess fluids, which can overwork the heart and cause fluid accumulation in the lungs. When diarrhea is caused by certain types of bacteria, treatment may include antibiotic therapy. Good nutrition and anti-inflammatory medications can speed recovery from diarrhea. Medications that slow motility of the large intestine should be avoided since they increase the risk of retaining feces and absorbing toxins.
Fecal Incontinence
A third abnormal condition of the large intestine is fecal incontinence, which can be defined as having inappropriate elimination of feces at least once a month.
Recall that fecal incontinence can be a complication of constipation. This occurs because mass peristalsis finally becomes strong enough to force feces into the rectum. Age changes in the rectum and anus that reduce the ability to retain feces voluntarily contribute to fecal incontinence from constipation and to the age-related increase in fecal incontinence from other causes. Among the factors that cause fecal incontinence are constipation; diarrhea; physical injury to the colon, rectum, or anus; nervous system abnormalities; diabetes mellitus; disability; and psychological disturbances.
Since many of the causes of fecal incontinence develop slowly and progressively and since each aging person may encounter more of these causes as time passes, fecal incontinence usually develops gradually and becomes worse over time.
The consequences of fecal incontinence are diverse and devastating. If feces are present on clothes or bed linens, they may also be in contact with the skin for prolonged periods, irritating the skin and causing infections. Even if these problems are avoided, people with fecal incontinence often suffer severe social disruption, social isolation, and psychological upheaval. The magnitude of the disturbances is sufficient to make fecal incontinence (together with urinary incontinence) the second leading cause of institutionalization among the elderly. Only disorders of the nervous system such as strokes and dementia rank higher as a cause of institutionalization.
Since fecal incontinence is an abnormal condition and since its causes are well known, much can be done to prevent, reduce, or stop its occurrence. The main strategy in each case is to identify the specific causes and reduce or eliminate them. Suggestions for preventing or stopping constipation and diarrhea were presented above. Individuals with structural irregularities of the colon, rectum, or anus may be helped by corrective surgery. Many individuals whose fecal incontinence results from disorders affecting the nervous system can be helped by biofeedback training combined with exercising the external sphincter muscle to increase its strength. Biofeedback training and muscle strengthening can also be helpful for individuals who are incontinent for reasons other than nervous system disorders. Such training increases the individual's awareness of the need to defecate and the individual’s control of the external sphincter. Strengthening the external sphincter enables the individual to retain feces until defecation is desired. A combination of training and muscle strengthening is required for significant and long-lasting progress in reducing or stopping fecal incontinence.
Another key factor in preventing or reducing fecal incontinence is making toilet facilities easily accessible or available at appropriate times by scheduling visits to the toilet at specific times or intervals. Attempting to defecate shortly after eating is often effective because filling the stomach leads to reflexive mass peristalsis and a high probability of having a successful defecation shortly afterward. Using dietary modifications to regulate intestinal functioning can also increase control of defecation. Examples include regulating water intake and reducing the intake of foods such as beans, cabbage, and cauliflower, which cause intestinal gas production. Control of defecation can be further increased by using medications to regulate intestinal functioning or by modifying the use of medications for other disorders.
Many aspects of preventing or reducing the incidence and effects of fecal incontinence depend on the actions of those who care for affected individuals. While ample care is important, the extra attention and social interaction that usually accompany the extra care may perpetuate or increase the problem by unintentionally providing positive reinforcement for incidents of incontinence.
Diverticulosis and Diverticulitis
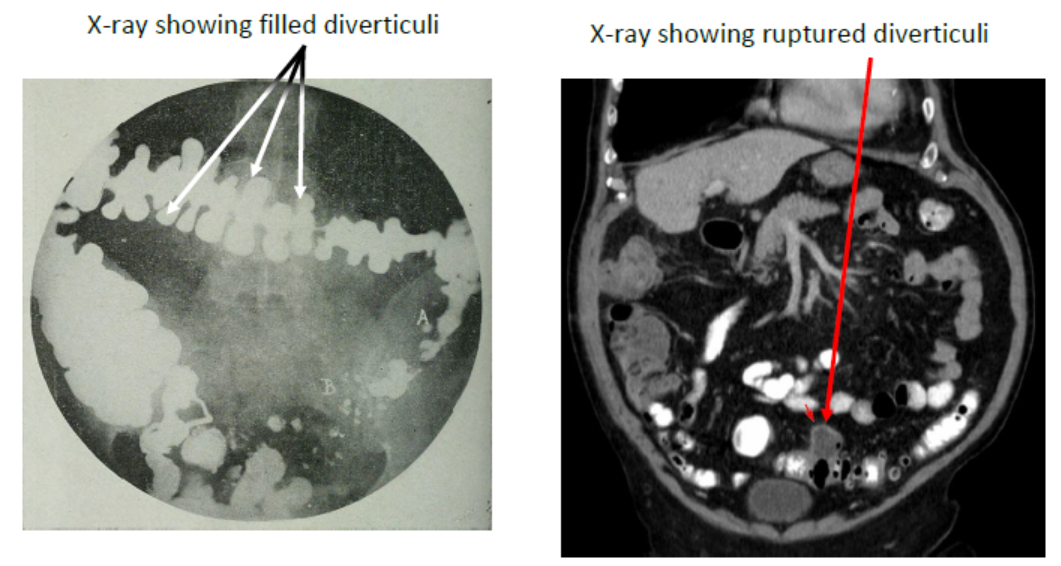
Diverticulosis is characterized by the presence of deep outpocketings (diverticula) in the wall of the large intestine (Figure 10.5). Usually, each diverticulum has a narrow opening leading to an expanded outer region. Most diverticula occur in the sigmoid colon.
Diverticulosis is present in about 30 percent of people over age 60, its incidence increases to about 50 percent of those over age 70, and it may occur in 60 percent of those over age 80. The number of diverticula increases with age.
Though 80 to 85 percent of people with diverticulosis have no ill effects from this disorder, diverticula in the remaining 15 to 20 percent become inflamed. When this occurs, the condition is called diverticulitis. The longer a person has diverticulosis, the greater is the chance of developing diverticulitis.
Diverticulosis develops when excessive pressure from strong mass peristalsis, such as from constipation or intestinal spasms, cause the intestinal wall to bulge outward at weak spots such as haustra and blood vessels. Most cases are believed to result from inadequate amounts of fiber in the diet over a period of years.
Diverticulosis leads to diverticulitis when fecal material becomes trapped within the diverticula and produces noxious material. Irritation of diverticula by entrapped indigestible particles such as seed hulls may also cause diverticulitis.
Most people who develop diverticulitis experience significant abdominal pain, constipation, or diarrhea. Diverticulitis causes intestinal bleeding in approximately 25 percent of cases. Though the bleeding is usually slow and is not life-threatening, it may lead to anemia. Individuals with anemia usually become fatigued quickly and may be lethargic because inadequate amounts of oxygen are delivered to body cells.
Other serious complications of diverticulitis include infection and perforation of the large intestine. If the large intestine perforates, feces can pass into the surrounding body cavity. This condition can cause excruciating pain and lead to death from extremely low blood pressure or widespread infection.
Prevention of diverticulosis and diverticulitis is relatively easy if adequate dietary fiber is consumed daily and constipation is avoided. Those who have developed either abnormality can be helped by increasing their intake of dietary fiber, avoiding constipation, and avoiding foods containing seeds or other materials that increase intestinal inflammation. Antibiotics may be prescribed for those who have developed infections. Individuals with advanced cases of diverticulosis may require surgical removal of portions of the large intestine.
Hemorrhoids
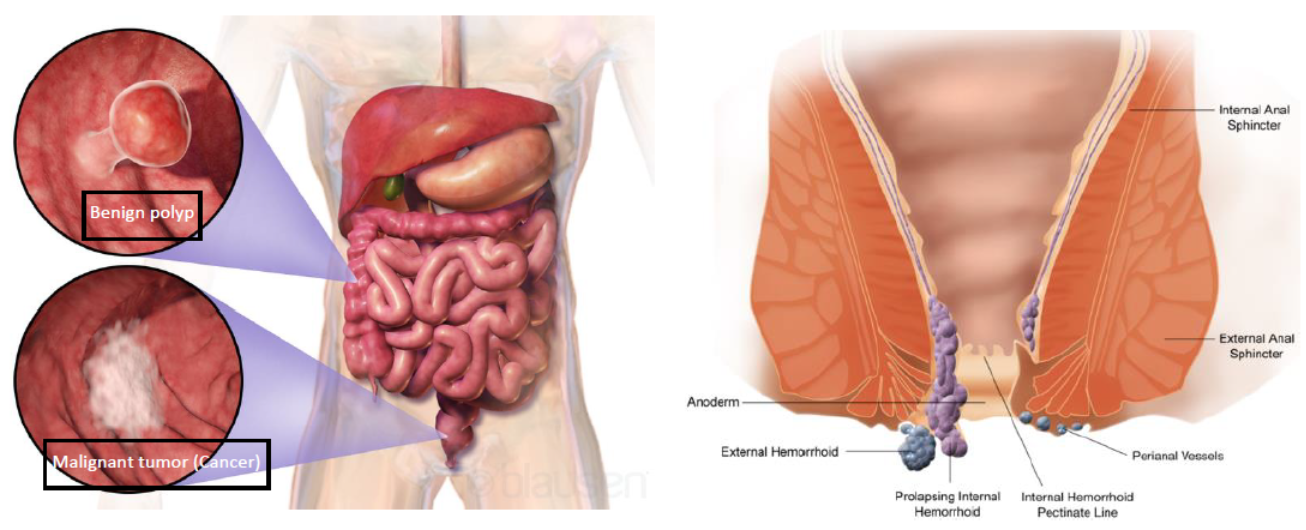
A fifth abnormality of the large intestine is the presence of hemorrhoids (Figure 10.5). These varicose veins in the rectum and anal canal were discussed in Chapter 4. Their occurrence increases and they become more of a problem as age advances because the factors that promote them increase with age.
Hemorrhoids result from conditions that cause repeated high pressure in the rectal and anal areas such as straining during bowel movements that accompany constipation, straining while lifting heavy objects, chronic coughing from bronchitis, and cirrhosis of the liver. Hemorrhoids can cause considerable pain and discomfort and, if they bleed regularly, can lead to anemia. Injured and inflamed hemorrhoids may become infected.
Preventing hemorrhoids involves avoiding circumstances that cause high pressures near the rectum and anus. Individuals with hemorrhoids can relieve discomfort by applying appropriate salves to the affected area. More advanced cases and hemorrhoids that contain clotted blood can be treated surgically.
Cancer is a disease characterized by uncontrolled reproduction and spreading of cells. Cancer of the large intestine is called colorectal cancer (Figure 10.5).
The incidence of colorectal cancer increases dramatically after approximately age 40, nearly doubling with each 5-year increase beyond that age. It occurs equally among men and women. Of all forms of cancer in the United States, only lung cancer occurs with a higher frequency.
Colorectal cancer is a common cause of death. It ranks as the third leading cause of death from cancer, accounting for about 15 percent of all deaths from cancer in adults. Only lung cancer and breast cancer cause more deaths. Since colorectal cancer increases in incidence with age, it ranks as a major cause of death among the elderly. It is the second leading cause of cancer deaths for men over age 75 and the leading cause of cancer deaths for women over age 75.
Though the causes of colorectal cancer are not known, several factors are known to increase the risk of developing it. They include diets low in fiber; diets high in meats, animal fat, or sugar; having relatives with colorectal cancer; having the identifiable gene that promotes familial colorectal cancer; having cancer of the breast or female reproductive organs; having noncancerous intestinal growths such as polyps; and conditions that cause chronic intestinal inflammation, such as ulcerative colitis.
Colorectal cancer can cause obstruction of the large intestine and destroy the intestinal wall. Obstruction can cause toxic materials from intestinal bacteria to accumulate and be absorbed into the body. Obstruction of the large intestine or destruction of the intestinal wall can lead to intestinal perforation and widespread infection. Colorectal cancer can also cause substantial bleeding. Finally, it often spreads to other parts of the body, such as the liver and lungs, and can destroy any organ it enters. The functioning of organs damaged by cancer is reduced, and their ability to help maintain homeostasis diminishes. Illness and death result.
One main way to combat colorectal cancer is to reduce the major dietary risk factors. Such changes seem to minimize the formation and accumulation of carcinogens in the large intestine. Other important preventive measures for colorectal cancer and its consequences include early detection and prompt treatment. Warning signs, such as having blood in the feces and having noticeable changes in bowel functioning, should be followed up by a professional examination. People over age 40 should have routine diagnostic testing for this cancer. People with a family history of colorectal cancer can be screened for the presence of the gene, for familial colorectal cancer and can receive more frequent and thorough diagnostic testing if they have the gene. Finally, removal of polyps may be advisable.
Once colorectal cancer has developed, the only effective treatment is surgical removal of the affected areas. Chemotherapy or radiation therapy is sometimes used before surgical treatment of cancer in the rectum or anus.
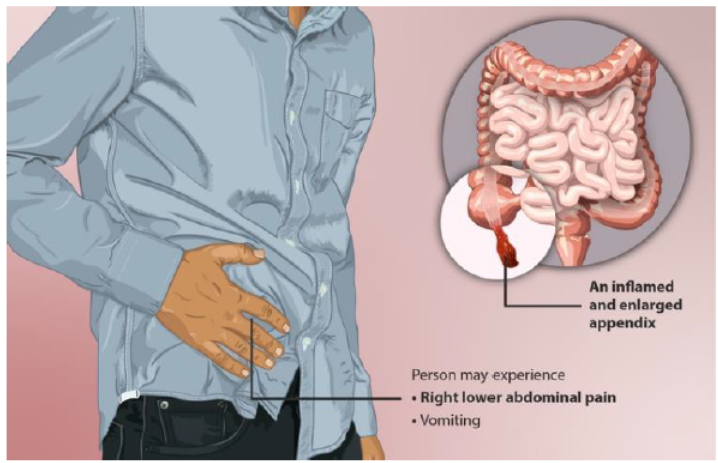
Appendicitis
Inflammation of the appendix (appendicitis) may be caused by entrapment of feces within the blind passageway in the appendix or infection of the lymph nodes in the appendix wall, both of which cause the appendix to become infected (Figure 10.5). The infection can be spread through the body by the circulatory system. A life-threatening crisis develops if the appendix ruptures and feces and infected material, such as pus, spread into the body cavity surrounding it. Older people face the same dangers of infection found in younger people.
The incidence of appendicitis decreases with age. However, cases in older individuals may be more severe, and the incidence of rupturing increases because age-related reductions in sensitivity to symptoms and milder signs of disease cause a delay in seeking diagnosis. In addition, an age-related reduction in blood flow allows deterioration of the appendix to occur faster and rupturing to occur sooner. Appendicitis is treated by surgical removal of the appendix. Antibiotics may be administered to combat infection.