
2.7: Focused Assessments
- Page ID
- 9993

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Health care professionals do focused assessments in response to a specific patient health problem recognized by the assessor as needing further assessment of a body system or systems.
Focused Respiratory System Assessment

Figure 2.2 Respiratory system
A focused respiratory system assessment includes collecting subjective data about the patient’s history of smoking, collecting the patient’s and patient’s family’s history of pulmonary disease, and asking the patient about any signs and symptoms of pulmonary disease, such as cough and shortness of breath. Objective data is also assessed.
The focused respiratory system assessment in Checklist 19 outlines the process for gathering objective data.
Checklist 19: Focused Respiratory System AssessmentDisclaimer: Always review and follow your hospital policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Conduct a focused interview related to history of respiratory disease, smoking, and environmental exposures. | Ask relevant questions related to dyspnea, cough/sputum, fever, chills, chest pain with breathing, previous history, treatment, medications, etc. | ||
2. Inspect:
|
Patients in respiratory distress may have an anxious expression, pursed lips, and/or nasal flaring.
Asymmetrical chest expansion may indicate conditions such as pneumothorax, rib fracture, severe pneumonia, or atelectasis. 
Assess respiration rate With hypoxemia, cyanosis of the extremities or around the mouth may be noted. |
||
| 3. Auscultate (anterior and posterior) lungs for breath sounds and adventitious sounds. | Fine crackles (rales) may indicate asthma and chronic obstructive pulmonary disease (COPD).
Coarse crackles may indicate pulmonary edema. Wheezing may indicate asthma, bronchitis, or emphysema. Low-pitched wheezing (rhonchi) may indicate pneumonia. Pleural friction rub (creaking) may indicate pleurisy. 
Auscultate anterior chest; blue dots indicate stethoscope placement for auscultation 
Auscultate posterior chest; blue dots indicate stethoscope placement for auscultation |
||
| 4. Report and document assessment findings and related health problems according to agency policy. | Accurate and timely documentation and reporting promote patient safety. | ||
| Data source: Assessment Skill Checklists, 2014; Jarvis et al., 2014; Perry et al., 2014; Stephen et al., 2012; Wilson & Giddens, 2013 | |||
Focused Cardiovascular and Peripheral Vascular System Assessment
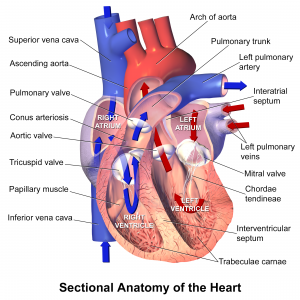
Figure 2.3 Anatomy of the heart
The cardiovascular and peripheral vascular system affects the entire body. A cardiovascular and peripheral vascular system assessment includes collecting subjective data about the patient’s diet, nutrition, exercise, and stress levels; collecting the patient’s and the patient’s family’s history of cardiovascular disease; and asking the patient about any signs and symptoms of cardiovascular and peripheral vascular disease, such as peripheral edema, shortness of breath (dyspnea), and irregular pulse rate. Objective data is also assessed.
The focused cardiovascular and peripheral vascular system assessment in Checklist 20 outlines the process for gathering objective data.
Checklist 20: Focused Cardiovascular/Peripheral Vascular System AssessmentDisclaimer: Always review and follow your hospital policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
| 1. Conduct a focused interview related to cardiovascular and peripheral vascular disease. | Ask relevant questions related to chest pain/shortness of breath (dyspnea), edema, cough, fatigue, cardiac risk factors, leg pain, skin changes, swelling in limbs, history of past illnesses, history of diabetes, injury. | ||
2. Inspect:
|
Cyanosis is an indication of decreased perfusion and oxygenation.

Assess capillary refill 
Assess bilateral lower legs Alterations and bilateral inconsistencies in colour, warmth, movement, and sensation (CWMS) may indicate underlying conditions or injury. Sudden onset of intense, sharp muscle pain that increases with dorsiflexion of foot is an indication of deep venous thrombosis (DVT), as is increased warmth, redness, tenderness, and swelling in the calf. Note: DVT requires emergency referral because of the risk of developing a pulmonary embolism. |
||
| 3. Auscultate apical pulse for one minute. Note the rate and rhythm. | Note the heart rate and rhythm. Identify S1 and S2 and follow up on any unusual findings.

Auscultate apical pulse at the fifth intercostal space and midclavicular line |
||
| 4. Palpate the radial, brachial, dorsalis pedis, and posterior tibialis pulses. | Absence of pulse may indicate vessel constriction, possibly due to surgical procedures, injury, or obstruction.

Assess tibial pulses 
Assess pedal pulses |
||
| 5. Report and document assessment findings and related health problems according to agency policy. | Accurate and timely documentation and reporting promote patient safety. | ||
| Data source: Assessment Skill Checklists, 2014; Jarvis et al., 2014; Perry et al., 2014; Stephen et al., 2012; Wilson & Giddens, 2013 | |||
Focused Gastrointestinal and Genitourinary Assessment

Figure 2.4 Gastrointestinal system

Figure 2.5 Components of the urinary system
The gastrointestinal and genitourinary system is responsible for the ingestion of food, the absorption of nutrients, and the elimination of waste products. A focused gastrointestinal and genitourinary assessment includes collecting subjective data about the patient’s diet and exercise levels, collecting the patient’s and the patient’s family’s history of gastrointestinal and genitourinary disease, and asking the patient about any signs and symptoms of gastrointestinal and genitourinary disease, such as abdominal pain, nausea, vomiting, bloating, constipation, diarrhea, and characteristics of urine and faeces. Objective data is also assessed.
The focused gastrointestinal and genitourinary assessment in Checklist 21 outlines the process for gathering objective data.
Checklist 21: Focused Gastrointestinal and Genitourinary AssessmentDisclaimer: Always review and follow your hospital policy regarding this specific skill. |
|||
Safety considerations:
|
|||
| Position patient supine if tolerated | |||
Steps |
Additional Information |
||
| 1. Conduct a focused interview related to gastrointestinal and genitourinary systems. | Ask relevant questions related to the abdomen, urine output, last bowel movement, flatus, any changes, diet, nausea, vomiting, diarrhea. | ||
2. Inspect:
|
Abdominal distension may indicate ascites associated with conditions such as heart failure, cirrhosis, and pancreatitis. Markedly visible peristalsis with abdominal distension may indicate intestinal obstruction. | ||
| 3. Auscultate abdomen for bowel sounds in all four quadrants before palpation. | Hyperactive bowel sounds may indicate bowel obstruction, gastroenteritis, or subsiding paralytic ileus.
Hypoactive or absent bowel sounds may be present after abdominal surgery, or with peritonitis or paralytic ileus. 
Auscultate abdomen for bowel sounds in all four quadrants |
||
| 4. Palpate abdomen lightly in all four quadrants. | Palpate to detect presence of masses and distension of bowel and bladder.

Palpate abdomen lightly in all four quadrants Pain and tenderness may indicate underlying inflammatory conditions such as peritonitis. |
||
| Note: If patient is wearing a brief, ensure it is clean and dry. Inspect skin underneath for signs of redness/rash/breakdown. | |||
| Note: If patient has a Foley catheter, inspect bag for urine amount, colour, and clarity. Inspect skin at insertion site for redness/breakdown. | |||
| 5. Report and document assessment findings and related health problems according to agency policy. | Accurate and timely documentation and reporting promote patient safety. | ||
| Data source: Assessment Skill Checklists, 2014; Jarvis et al., 2014; Perry et al., 2014; Stephen et al., 2012; Wilson & Giddens, 2013 | |||
Focused Musculoskeletal System Assessment

Figure 2.6 Anterior and posterior views of muscles
A focused musculoskeletal assessment includes collecting subjective data about the patient’s mobility and exercise level, collecting the patient’s and the patient’s family’s history of musculoskeletal conditions, and asking the patient about any signs and symptoms of musculoskeletal injury or conditions. Objective data is also assessed.
The focused musculoskeletal assessment in Checklist 22 outlines the process for gathering objective data.
Checklist 22: Focused Musculoskeletal System AssessmentDisclaimer: Always review and follow your hospital policy regarding this specific skill. |
|||
Safety considerations:
|
|||
Steps |
Additional Information |
||
1. Check patient information prior to assessment:
|
Determine patient’s activity as tolerated (AAT)/bed rest requirements.

Patient position prior to standing Determine if patient has non-weight-bearing, partial, or full weight-bearing status. Determine if patient ambulates independently, with one-person assist (PA), two-person assist (2PA), standby, or lift transfer. Check alertness, medications, pain. Ask if patient uses walker/cane/wheelchair/crutches. Consider non-slip socks/hip protectors/bed-chair alarm. |
||
| 2. Conduct a focused interview related to mobility and musculoskeletal system. | Ask relevant questions related to the musculoskeletal system, including pain, function, mobility, and activity level (e.g., arthritis, joint problems, medications, etc.). | ||
3. Inspect, palpate, and test muscle strength and range of motion:
Evaluate client’s ability to sit up before standing, and to stand before walking, and then assess walking ability. |
Note strength of handgrip and foot strength for equality bilaterally.

Assess strength on dorsiflexion
Assess strength on plantar flexion 
Assess grip strength Note patient’s gait, balance, and presence of pain. |
||
| 4. Report and document assessment findings and related health problems according to agency policy. | Accurate and timely documentation and reporting promote patient safety. | ||
| Data source: Assessment Skill Checklists, 2014; Jarvis et al., 2014; Perry et al., 2014; Stephen et al., 2012; Wilson & Giddens, 2013 | |||
Focused Neurological System Assessment
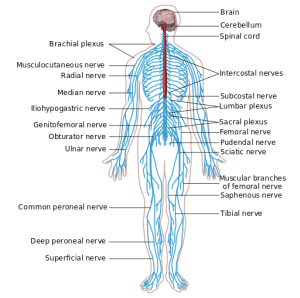
Figure 2.7 Nervous system
The neurological system is responsible for all human function. It exerts unconscious control over basic body functions, and it also enables complex interactions with others and the environment (Stephen et al., 2012). A focused neurological assessment includes collecting subjective data about the patient’s history of head injury or dysfunction, collecting the patient’s and the patient’s family’s history of neurological disease, and asking the patient about signs and symptoms of neurological conditions, such as seizures, memory loss (amnesia), and visual disturbances. Objective data is also assessed.
The focused neurological assessment in Checklist 23 outlines the process for gathering objective data.
Checklist 23: Focused Neurological System AssessmentDisclaimer: Always review and follow your hospital policy regarding this specific skill. |
|||||||||||||||||||||||||||||||||||||||
Safety considerations:
|
|||||||||||||||||||||||||||||||||||||||
Steps |
Additional Information |
||||||||||||||||||||||||||||||||||||||
| 1. Conduct a focused interview related to the neurological system. | Ask relevant questions related to past or recent history of head injury, neurological illness, or symptoms, confusion, headache, vertigo, seizures, recent injury or fall, weakness, numbness, tingling, difficulty swallowing (dysphagia) or speaking (dysphasia), and lack of coordination of body movements.

Focused interview |
||||||||||||||||||||||||||||||||||||||
| 2. Assess mental health status. | Assess mental status by observing the patient’s appearance, attitude, activity (behaviour), mood and affect, and asking questions similar to those outlined in this example of a mini-mental state examination (MMSE). | ||||||||||||||||||||||||||||||||||||||
3. Assess neurological function using the Glasgow Coma Scale (GCS):
|
|
||||||||||||||||||||||||||||||||||||||
| 4. Note patient’s LOC (level of consciousness, oriented x 3), general appearance, and behaviour. | Note hygiene, grooming, speech patterns, facial expressions. | ||||||||||||||||||||||||||||||||||||||
| 5. Assess pupils for size, equality, reaction to light (PERL), and consensual reaction to light. | Unequal pupils may indicate underlying neurological disease or injury.

Assess pupillary reaction to light |
||||||||||||||||||||||||||||||||||||||
6. Assess motor strength and sensation.
|
Unequal motor strength and unusual sensation may indicate underlying neurological disease or injury, such as stroke or head injury.

Assess motor strength and sensation of extremities
Assess motor strength and sensation of extremities
Assess motor strength and sensation of extremities |
||||||||||||||||||||||||||||||||||||||
| 7. Report and document assessment findings and related health problems according to agency policy. | Accurate and timely documentation and reporting promote patient safety. | ||||||||||||||||||||||||||||||||||||||
| Data source: Assessment Skill Checklists, 2014; Jarvis et al., 2014; Perry et al., 2014; Stephen et al., 2012; Wilson & Giddens, 2013 | |||||||||||||||||||||||||||||||||||||||
Critical Thinking Exercises
- Your patient complains of stomach pain during your head-to-toe assessment. What would be your next steps?
- You notice that your patient seems lethargic during your head-to-toe assessment. What would be your next steps?
Attributions
Figure 2.2
The respiratory system by LadyofHats is in the public domain.
Figure 2.3
Sectional anatomy of the heart by Blausen Medical Communications, Inc. is used under a CC BY 3.0 licence.
Figure 2.4
Digestive system diagram by Mariana Ruiz Villarreal is in the public domain.
Figure 2.5
Urinary system is in the public domain.
Figure 2.6
Anterior and posterior views of muscles by OpenStax College is used under a CC BY 3.0 licence.
Figure 2.7
Nervous system diagram by William Crochot is used under a CC BY SA 4.0 licence.