
11.2: Vitamin B₁₂
- Page ID
- 40990

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Vitamin \(B_{12}\) is unique among vitamins in that it contains an element (cobalt) and is found almost exclusively in animal products. Neither plants nor animals can synthesize vitamin \(B_{12}\). Instead, vitamin \(B_{12}\) in animal products is produced by microorganisms within the animal that the products came from. Animals consume the microorganisms in soil or microorganisms in the GI tract of ruminant animals produce vitamin \(B_{12}\) that can then be absorbed1. Some plant products, such as fermented soy products (tempeh, miso) and the sea algae supplement, spirulina, are advertised as being good sources of \(B_{12}\). However, fermented soy products are not a reliable vitamin \(B_{12}\) source2 and spirulina contains a pseudovitamin \(B_{12}\) compound that is not bioavailable3. For vegans, supplements, nutritional yeast, and fortified products like fortified soy milk can help them meet their vitamin \(B_{12}\) needs4.
Query \(\PageIndex{1}\)
Vitamin \(B_{12}\)'s scientific name is cobalamin, which makes sense when you consider it contains cobalt and many amine groups, as shown in the figure below.
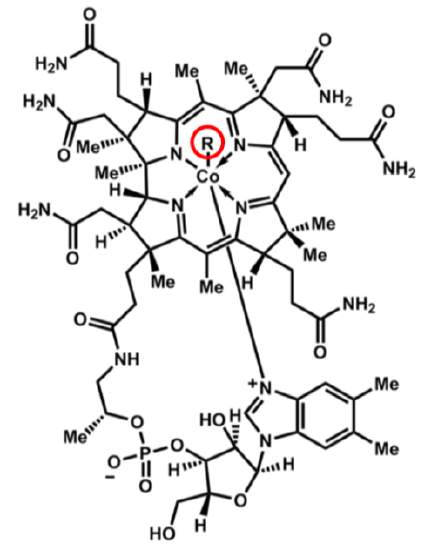
The other feature that is important in cobalamin is the circled R group. This is what differs between the different cobalamins, whose names and R groups are shown in the following table.
| R Group | Name |
|---|---|
| \(\ce{CN}\) | Cyanocobalamin |
| \(\ce{OH}\) | Hydroxocobalamin |
| \(\ce{H2O}\) | Aquocobalamin |
| \(\ce{NO2}\) | Nitritocobalamin |
| 5'-deoxyadenosyl | Adenosylcobalamin* |
| \(\ce{CH3}\) | Methylcobalamin* |
*Cofactor Forms
Query \(\PageIndex{2}\)
The 2 cofactor forms are adenosylcobalamin and methylcobalamin. We can convert most cobalamins into these 2 cofactor forms. Most foods contain adenosylcobalamin, hydroxocobalamin, or methylcobalamin6. The most common form found in supplements is cyanocobalamin, with some also using methylcobalamin7. Cyanocobalamin is a synthetic form of vitamin \(B_{12}\).
The uptake, absorption, and transport of vitamin \(B_{12}\) is a complex process. The overall bioavailability of vitamin \(B_{12}\) is believed to be approximately 50%3, with the different cobalamin forms having similar bioavailabilities7. Sublingual supplements of vitamin \(B_{12}\) have been found to be equally efficacious as oral supplements7. Excretion occurs mostly through bile, with little loss in urine6. The following descriptions and figures explain and illustrate, respectively, these processes.
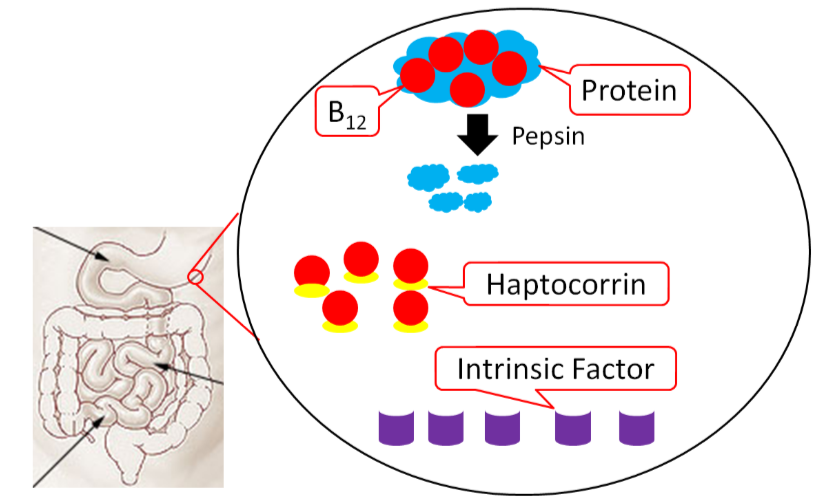
Vitamin \(B_{12}\) is normally bound to protein in food. Salivary glands in the mouth produce haptocorrin (formerly known as R protein), which travels with the food into the stomach. In the stomach, acid converts pepsinogen into pepsin, and the protein intrinsic factor is released from the parietal cells1,8.
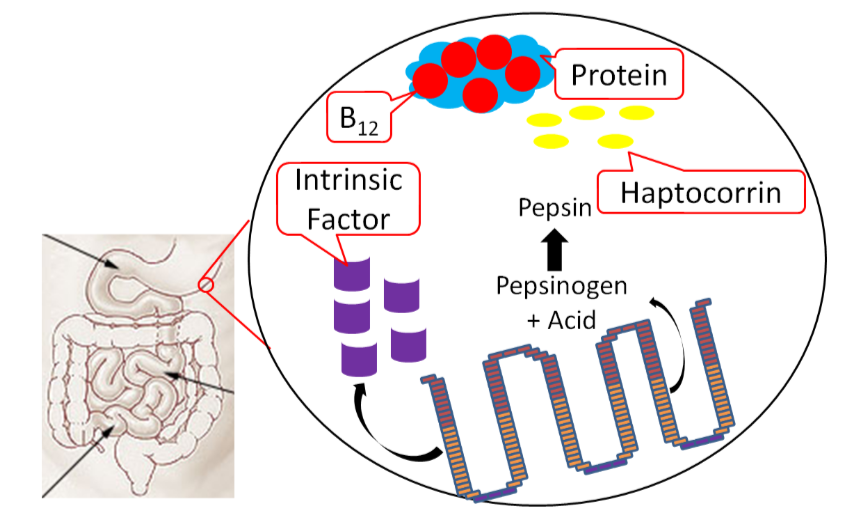
As pepsin frees \(B_{12}\) from protein, haptocorrin binds to the newly freed vitamin \(B_{12}\) (haptocorrin + \(B_{12}\)). Intrinsic factor escapes digestion and, along with haptocorrin + \(B_{12}\), exits the stomach and enters the duodenum1,8.
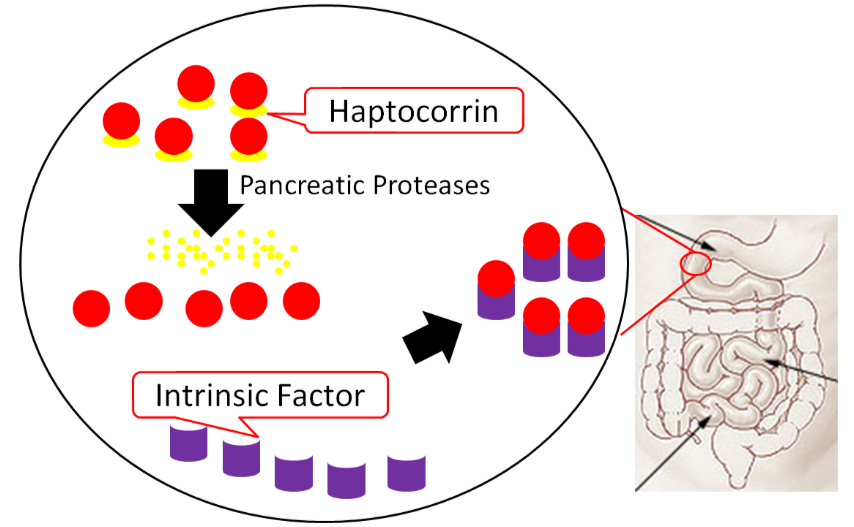
In the duodenum, pancreatic proteases break down haptocorrin, and again vitamin \(B_{12}\) is freed. Intrinsic factor then binds vitamin \(B_{12}\) (intrinsic factor + \(B_{12}\)); intrinsic factor + \(B_{12}\) continues into the ileum to prepare for absorption1,8.
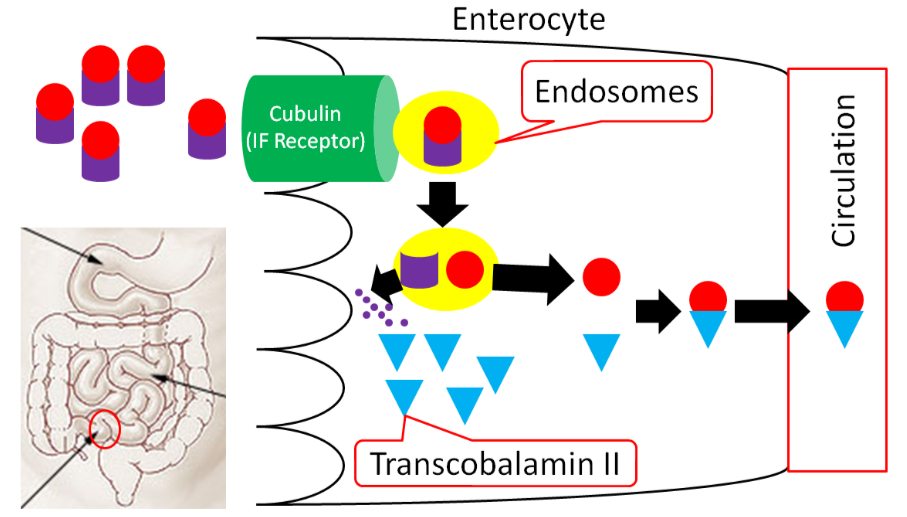
In the ileum, intrinsic factor + \(B_{12}\) is believed to be endocytosed by intrinsic factor binding to cubulin (aka intrinsic factor receptor), forming an endosome inside the enterocyte. Intrinsic factor is broken down in the enterocyte, freeing vitamin \(B_{12}\). The free vitamin \(B_{12}\) is then bound to transcobalamin II (TC II + \(B_{12}\)); TC II + \(B_{12}\) moves into circulation8.
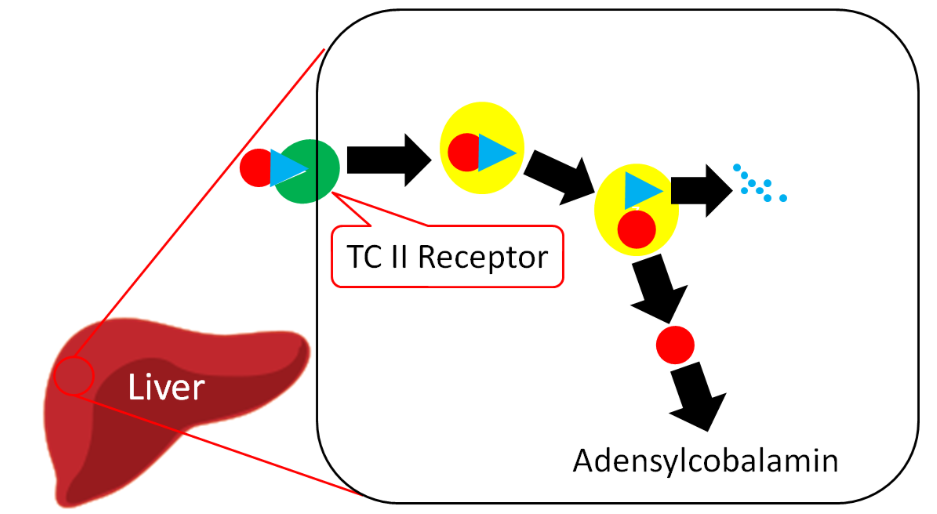
The liver is the primary storage site for vitamin \(B_{12}\). Unlike most other water-soluble vitamins, the liver is able to maintain significant stores of vitamin \(B_{12}\). Uptake into the liver occurs through the binding of TC II + \(B_{12}\) to the TC II Receptor and the endocytosis of both the compound and the receptor8. Vitamin \(B_{12}\) is once again freed after degradation of TC II. Vitamin \(B_{12}\) is primarily stored in the liver as adenosylcobalamin6,8.
Query \(\PageIndex{3}\)
Query \(\PageIndex{4}\)
Vitamin \(B_{12}\) Functions
Vitamin \(B_{12}\) is a cofactor for 2 enzymes and is also important for neuron function as described further below.
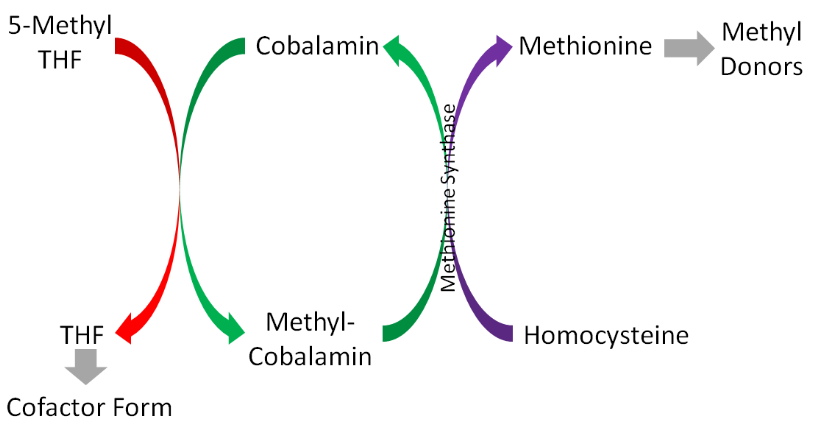
Methionine Synthase
Methionine synthase is an important enzyme in 1-carbon metabolism that uses methylcobalamin as its cofactor and converts homocysteine to methionine by adding a methyl group. Methionine is then converted to other compounds that serve as methyl donors, as shown below1.
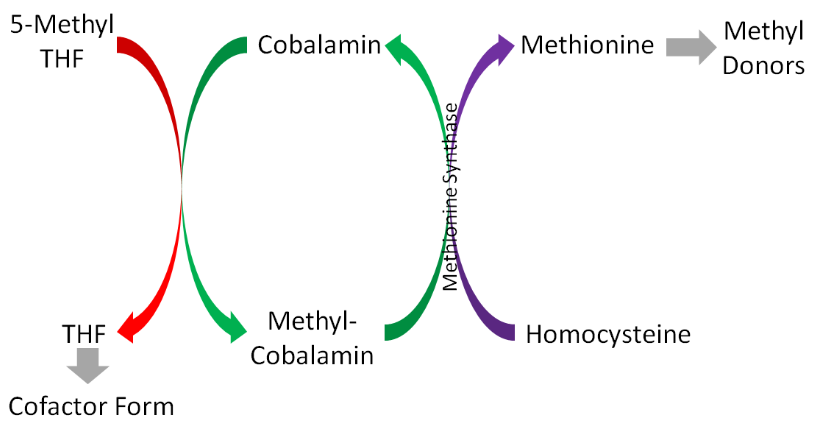
These methyl donors can donate methyl groups for methylating DNA, an epigenetic modification1.
Methymalonyl mutase
This enzyme uses adenosylcobalamin as its cofactor, and is important in the breakdown of odd chain fatty acids (5 carbons etc.). As you know, odd chain fatty acids are less common than even chain fatty acids, but this enzyme is required to properly handle these less common fatty acids1.
Demyelination
In addition to its role as a cofactor for enzymes, vitamin \(B_{12}\) is also important for preventing degradation of the myelin sheath that surrounds neurons, as shown below.
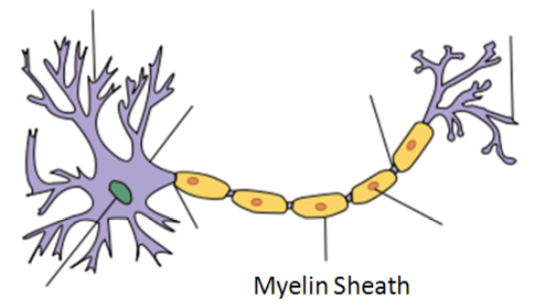
The mechanism by which vitamin \(B_{12}\) prevents demyelination is not known11.
Query \(\PageIndex{5}\)
Vitamin \(B_{12}\) Deficiency & Toxicity
There are 2 primary symptoms of vitamin \(B_{12}\) deficiency:
- Megaloblastic (Macrocytic) Anemia
- Neurological Abnormalities
Megaloblastic (Macrocytic) Anemia
This is the same type of anemia that occurs in folate deficiency that is characterized by fewer, enlarged, immature red blood cells. In vitamin \(B_{12}\) deficiency, this can occur because there is not enough cobalamin to convert 5-methyl THF to THF as it normally would as illustrated below.
Thus, THF is not available for normal DNA synthesis and the red blood cells do not divide correctly.
Query \(\PageIndex{6}\)
Neurological Abnormalities
Vitamin \(B_{12}\) deficiency also results in nerve degeneration and abnormalities that can often precede the development of anemia. These include a decline in mental function and burning, tingling, and numbness of legs. These symptoms can continue to worsen and deficiency can be fatal1.
The most common cause of vitamin \(B_{12}\) deficiency is pernicious anemia, a condition of inadequate intrinsic factor production that causes poor vitamin \(B_{12}\) absorption. This condition is common in people over the age of 50 because they have the condition atrophic gastritis12. Atrophic gastritis is a chronic inflammatory condition that leads to the loss of glands in the stomach, as shown in the figure in the following link.
Web Link
The loss of glands leads to decreased intrinsic factor production. It is estimated that ~6% of those age 60 and over are vitamin \(B_{12}\) deficient, with 20% having marginal status12. In addition to the elderly, vegans are also at risk for vitamin \(B_{12}\) deficiency because they do not consume animal products. However, the deficiency may take years to develop in adults because of stores and recycling of vitamin \(B_{12}\)13. Deficiency has the potential to occur much quicker in infants or young children on vegan diets because they do not have stores that adults do1.
Query \(\PageIndex{7}\)
Folate/Folic Acid masking vitamin \(B_{12}\) deficiency
As mentioned above, folate and vitamin \(B_{12}\) lead to the same megaloblastic (macrocytic) anemia. If high levels of folate or folic acid (most of the concern is with folic acid since it is fortified in foods and commonly taken in supplements) is given during vitamin \(B_{12}\) deficiency, it can correct this anemia. This is referred to as masking because it does not rectify the deficiency, but it "cures" this symptom. Folate/folic acid can do this by providing so much folate that there is enough THF for red blood cell division to occur even without having the cobalamin normally needed to accept a methyl group from 5-methyl THF. This is problematic because it does not correct the more serious neurological problems that can result from vitamin \(B_{12}\) deficiency. There are some people who are concerned about the fortification of cereals and grains with folic acid because people who are \(B_{12}\) deficient might not develop macrocytic anemia, which makes a vitamin \(B_{12}\) deficiency harder to diagnose12.
No toxicity of vitamin \(B_{12}\) has been reported.
Query \(\PageIndex{8}\)
References
- Byrd-Bredbenner C, Moe G, Beshgetoor D, Berning J. (2009) Wardlaw's perspectives in nutrition. New York, NY: McGraw-Hill.
- Craig W, Mangels A. (2009) Position of the american dietetic association: Vegetarian diets. J Am Diet Assoc 109(7): 1266-1282.
- Watanabe F. (2007) Vitamin B12 sources and bioavailability. Exp Biol Med 232(10): 1266-1274.
- http://www.vrg.org/nutrition/b12.php
- en.Wikipedia.org/wiki/File:Cobalamin.png
- Gropper SS, Smith JL, Groff JL. (2008) Advanced nutrition and human metabolism. Belmont, CA: Wadsworth Publishing.
- https://ods.od.nih.gov/factsheets/Vi...hProfessional/
- Shils ME, Shike M, Ross AC, Caballero B, Cousins RJ, editors. (2006) Modern nutrition in health and disease. Baltimore, MD: Lippincott Williams & Wilkins.
- commons.wikimedia.org/wiki/Fi...atal%C3%A0.png
- en.Wikipedia.org/wiki/Myelin...Hand-tuned.svg
- lpi.oregonstate.edu/infocente...min\(B_{12}\)/
- Whitney E, Rolfes SR. (2008) Understanding nutrition. Belmont, CA: Thomson Wadsworth.
- Allen L. (2009) How common is vitamin B-12 deficiency? Am J Clin Nutr 89(2): 693S-696S.