
15.3: Vitamin D
- Page ID
- 58115

Like vitamin A, vitamin D has a long history. Rickets, the most striking sign of D deficiency, was recognized at least 2,500 years ago. And centuries ago the deficiency disease was understood to be curable or preventable by eating certain foods—which eventually were found to be potent sources of vitamin D.
Rickets and Osteomalacia
Rickets is a deceptive and pathetic disorder. Infant victims may not look as if they suffer from malnutrition. But, in fact, they can suffer from a hidden failure of development which may not be apparent until they start to walk.
The condition is technically a form of osteomalacia, literally a softening of the bone. It’s the result of failure to absorb enough calcium—either because there isn’t enough calcium in the diet, or because the body’s absorption and use of calcium is limited by a shortage of vitamin D.
Such infants may be uncomfortably restless. The abdomen may be somewhat distended. The muscles are usually lacking in tone, and flabby. As the infants get older and begin walking, the weight of the body on the legs can cause the bones to become deformed, and the child is described as knock-kneed or bow-legged. The bones of the chest, spine, and pelvis may also become permanently deformed. The “sunken chest” of rickets can lead to lung problems, and a deformed pelvis can cause problems for women during childbirth.
In a sense, what happens in cases of rickets is akin to building the framework of a skyscraper with soft iron instead of steel. The framework may seem sound at first, but as more weight is placed upon it, the iron twists and bends—so also do the bones of children with rickets.
Although this pathetic disorder of development was long known, it became much more common with the coming of civilization, particularly in northern lands. The osteomalacia of adults also became more common, especially among poorer women in northern industrial cities, who regularly went through many pregnancies and long periods of breastfeeding.
By the 17th century in England, there was much speculation about the disorder and its causes. And by the latter part of the 19th century, up to 75% of the children living in the poor areas of industrial cities had rickets.
By the early 1800s, some practical answers to the problem had been found, but with no real understanding of why they were effective. In 1807, an English physician name Bardsley tested the old Scandinavian idea of giving cod-liver oil (a vitamin D source) to babies and young children, and found that the oil cured osteomalacia.
We are reminded again of the interrelationships between nutrients. Osteomalacia can result from a lack of either calcium or vitamin D, or a combined deficiency.
But Bardsley’s report went largely unrecognized. It wasn’t until 1889 and 1890, that two sets of experiments caught medical and public attention. In one, lion cubs at the London zoo were cured of rickets when fed a mixture of crushed bone (a calcium source) and cod-liver oil. Another experiment showed that, in some cases, sunlight alone could cure rickets. During the next 30 years, more bits and pieces of the puzzle gradually emerged.
By 1920, it was speculated that there was a “calcium-depositing, fat-soluble vitamin.” Vitamin D was finally isolated and synthesized in the 1930s, but it was learned even later that vitamin D must go through elaborate chemical pathways before it can take part in human chemistry. Some key parts of this work were accomplished in the 1970s, but the story is not yet complete.
Today, rickets is a relatively uncommon problem in world nutrition, although milder vitamin D deficiency is still common.1 In industrialized countries, it’s been understood since early in this century that certain food sources provided protection There has been steady progress in finding inexpensive ways to assure ample sources of the vitamin in commonly consumed foods.
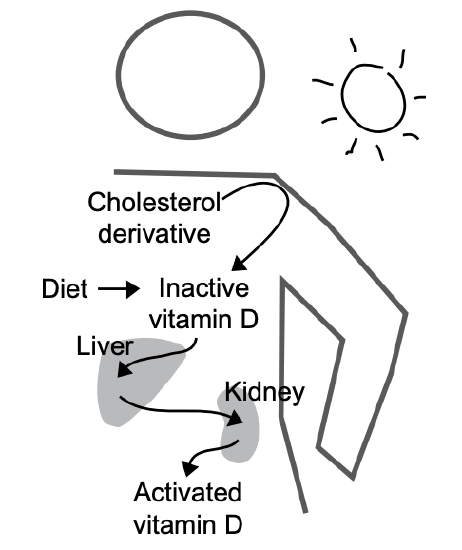
Figure 15-3: The active form of vitamin D
The Sunshine Vitamin
The active form of vitamin D is made in our body either from vitamin D in our diet, or from a derivative of cholesterol in our skin. When the cholesterol-derived precursor is struck by sunlight, there is a chemical change. It becomes vitamin D and is taken into the circulating blood. Thus, when there’s adequate exposure to the sun, vitamin D isn’t required in the diet.
We can begin to understand why the widespread rickets of the 19th century has been called a disease of civilization, and even of the industrial revolution. In Europe, for example, the factory towns of the north received little sunlight, and the workers (many of whom were children) had little chance to be outdoors. Also, in cold climates, more clothing is needed and less skin is exposed to sunlight.
Women workers had few daylight hours outside the factories. They spent as few days as possible away from their machines during and after pregnancy. They drank little milk and could afford little butterfat in foods during either pregnancy or lactation. Birth control methods were limited. Thus, in short, they had little of either sunlight or food sources of vitamin D, and poor reserves of either vitamin D or calcium. With repeated pregnancies and breastfeeding during young adulthood, their own bodies were rapidly depleted, and they became common victims of osteomalacia.
Another factor contributed as well. Much of milk was either watered or skimmed of some fat, thereby removing vitamin D. (Most of the low-fat and fat-free milk sold today in the United States is fortified with vitamin D.) Butterfat (the source of vitamin D in milk), was the most valued part of dairy products. Creams, cheeses, and other butterfat-rich products were not for the poor.
Vitamin D and Body Chemistry
Even after vitamin D has been consumed in food or made in the skin, further chemical changes are needed before the body can use it. First, the liver makes a chemical change. Then, the kidneys make a second change, and the vitamin D is now called activated vitamin D (see Fig. 15-3).
When either the liver or kidney is compromised by injury or disease, vitamin D activation is impaired. Chronic kidney disease can produce some of the signs of vitamin D deficiency, since the necessary modification of the vitamin doesn’t occur at a normal rate.
Activated vitamin D is needed for the absorption of calcium and phosphorus. It also controls both calcium and phosphorus in the mineralization of bone. These two minerals are used together in about equal amounts to form bone and teeth.
Moreover, we know that calcium and phosphorus are chemically necessary to the nerve‑muscle systems of the body, and are involved in muscular contraction and relaxation. And apparently, wherever these two minerals are used, vitamin D is used. The vitamin appears to signal various cells to produce special proteins needed to transport these minerals.
These more recent insights suggest why the symptoms of rickets (and other forms of osteomalacia) extend beyond weak and malformed bones. The involvement of vitamin D with the muscular and neurological systems explains why deficiencies can cause rickets-associated muscle spasms and weakness, and such psychological effects as irritability and restlessness.
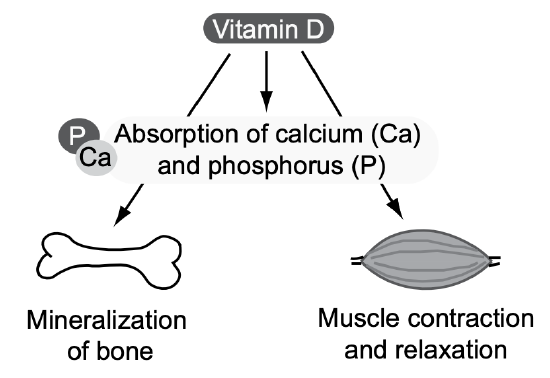
Figure 15-4: Vitamin D, calcium, and phosphorous function together.
Vitamin D Requirements
It could be said that civilization made vitamin D a vitamin (in the sense that it was needed in the diet). Since vitamin D can be made as long as sunlight is allowed to fall on the skin, deficiencies apparently began when civilization took people out of the sun.
Sunlight production of vitamin D varies according to the intensity of the light, time of exposure, amount of skin exposed, color of one’s skin, and the use of sunscreen. The lighter the skin, the more efficient the absorption of solar radiation. Conversely, the pigmentation of dark-skinned people can keep as much as 95% of solar radiation from reaching the deeper layers, where most of the vitamin production occurs.
Moderation and Balance: Not enough sun exposure means less vitamin D production, but too much increases the risk of skin cancer.
There have been studies that link living at higher latitudes (where people have less sun exposure) and/or are vitamin D deficient, to higher rates of some cancers.4 However, randomized clinical trails of vitamin D supplementation do not support a lowering of cancer risk.
People of all races can get all the vitamin D they need with enough sun exposure, but many simply cannot or do not get enough sun exposure. For these people, vitamin D must be ingested. The Food and Nutrition Board has set an adequate intake to be 10 µg per day from birth to age 50, 15 µg/day for ages 51-70, and 20 µg/day for those over age 70 (see Appendix A). Older adults usually get less sun exposure, and vitamin D production from sun exposure is less efficient.
Because of so much variance in skin-production of vitamin D and dietary intakes, blood levels of vitamin D are used to assess adequacy.
Infant formula has enough vitamin D, but human milk doesn’t. So a vitamin D supplement is advised for breast-fed infants, (An alternative might be more exposure to direct sunlight, but is not advised due to increased risk of skin cancer.)
Vitamin D in Foods
Unless foods are fortified with vitamin D, few are very potent sources. Fish livers, certain fatty fish, and liver and fat from seals and polar bears are good sources of vitamin D, but most of us do not eat much of these. The most common source of vitamin D in our diet is vitamin D fortified foods such as milk and many breakfast cereals. Cow’s milk is a convenient vehicle for vitamin D fortification, especially because milk is an important source of calcium.
The Toxicity of Excess
Excesses are stored in the liver, and toxic amounts are typically from supplements. (Sun exposure doesn’t result in toxic amounts.) Excess vitamin D can lead to weight loss, vomiting, irritability, and destructive deposits of excess calcium in soft tissues, like those of blood vessels, lung and kidney. The UL (Upper Limit) for vitamin D is 100 µg/day for ages 9 and older.