1.12: Laryngectomy - Total
- Page ID
- 17620

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
TOTAL LARYNGECTOMY
Johan Fagan
Total laryngectomy is generally done for advanced cancers of the larynx and hypopharynx, recurrence following (chemo)radiation, and occasionally for intractable aspiration and advanced thyroid cancer invading the larynx.
Although it is an excellent oncologic procedure and secures good swallowing without aspiration, it has disadvantages such as having a permanent tracheostomy; that verbal communication is dependent on esophageal speech, and/or trachepesophageal fistula speech or an electrolarynx; hyposmia; and the psychological and financial/ employment implications. Even in the best centers, about 20% of patients do not acquire useful verbal communication.
Prelaryngectomy decision making
The surgeon needs to consider the following issues before embarking on a laryngectomy.
- What will be the tumor resection lines? As the initial incisions into the pharynx are done from externally without having the tumor in view, the surgeon must carefully assess the valleculae, base of tongue and the pyriform fossae for tumor involvement, to avoid cutting into tumor when entering the pharynx. Involvement of the base of tongue may also prompt the surgeon to opt for a retrograde laryngectomy (commencing the laryngectomy at the tracheostomal end of the specimen). In the absence of CT or MRI imaging, one can palpate and assess tumor involvement of the pre-epiglottic space and base of tongue under general anesthesia by placing one index finger in the valleculae, and the other on the skin of the neck just above the hyoid bone. The fingers should normally virtually meet, unless there is tumor in the preepiglottic space or vallecula or base of tongue.
- Is thyroidectomy required? Both hypothyroidism and hypoparathyroidism are common sequelae of total laryngectomy, particularly following postoperative radiation therapy, and may be difficult to manage in a developing world setting. Twenty-five percent of laryngectomy patients become hypothyroid following hemithyroidectomy; and 75% if postoperative radiation is added. However, both thyroid lobes may be preserved unless Level 6 nodes need to be resected with subglottic and pyriform fossa carcinoma, or when there is intraoperative or radiological evidence of direct tumor extension to involve the thyroid gland.
- Will a pectoralis major flap be required? A capacious pharynx is essential for good swallowing and fistula speech. Should tumor involve the hypopharynx, especially when it extends distally towards the cricopharyngeus, then the expertise must be available to possibly augment the pharyngeal repair with a pectoralis major flap. Pectoralis major muscle flaps are also frequently used to overlay the pharyngeal repair with salvage laryngectomy to encourage spontaneous closure of pharyngo-cutaneous fistulae when they occur.
- Is elective neck dissection required? With advanced laryngeal squamous cell carcinoma requiring laryngectomy, elective lateral neck dissection (Levels 2-4), either ipsilateral (glottic carcinoma) or bilateral (supraglottic, medial wall of pyriform fossa, bilateral glottic carcinoma) is recommended, with conversion to modified neck dissection should cervical metastases be found intraoperatively. Level 6 is included in subglottic and pyriform fossa carcinoma to clear the paratracheal nodes.
- Is the patient suitable for tracheo-esophageal speech? This decision is based on assessment of cognitive function, motivation, financial ability to pay for replacement speech prostheses, and proximity to speech services.
- Are there synchronous primaries or distant metastases? Total laryngectomy has significant morbidity and should only be done if panendoscopy and CXR/CT chest exclude metastases or 2nd primaries.
Anesthesia
Intubation: The operation is done under general anesthesia. The ENT surgeon must be present to assist with a possibly difficult intubation. If a difficult intubation is anticipated, then either do an awake tracheostomy, or infiltrate skin and trachea with local anesthesia/vasoconstrictor, in preparation for a possible emergency tracheostomy.
Preoperative tracheotomy: Tracheotomy may have been required for airway obstruction. It is not an independent indication for postoperative radiation therapy unless tumor was entered at the time of tracheotomy. If a tracheostomy has already been done, then ask the anesthetist to reintubate through the larynx with an orotracheal tube once the patient has been anesthetized as this facilitates dissection in the lower neck and speeds up the surgery.
Perioperative antibiotics: Commence perioperative antibiotics before putting knife to skin, and continue for 24 hrs.
Surgical anatomy
Figures 1 & 2 illustrate all the muscles that will be divided during laryngectomy.
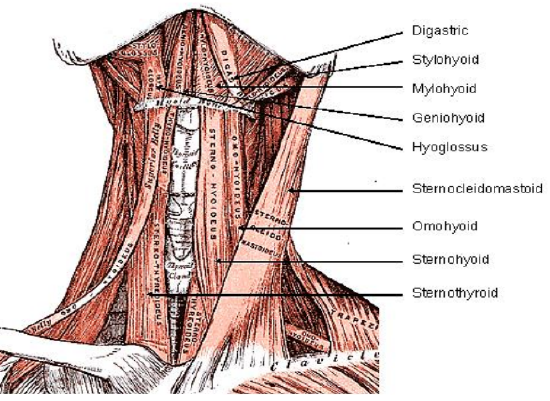
Figure 1: Supra- and infrahyoid muscles
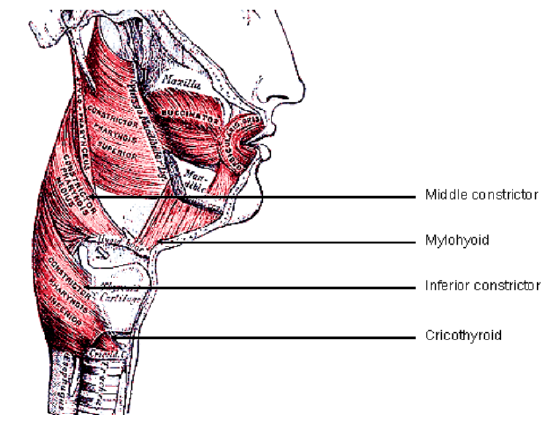
Figure 2: Middle and inferior pharyngeal constrictors
Surgical steps
Positioning: Extend the neck
Incisions for apron flap (Figures 3a, b)
The horizontal limb of the flap is placed approximately 2 cm above the sternal notch. An ellipse of skin around a preexisting tracheostomy is included with the resection. With a simple laryngectomy the vertical incisions are placed along the anterior borders of sternocleidomastoid muscles. For a laryngectomy with neck dissection(s), either a wider flap overlying the sternocleidomastoid muscles is made (Figure 3a), or a narrow flap with inferolateral extensions is made (Figure 3b). The latter has the disadvantage of a trifurcation which is more prone to wound breakdown and exposure of the major cervical vessels.
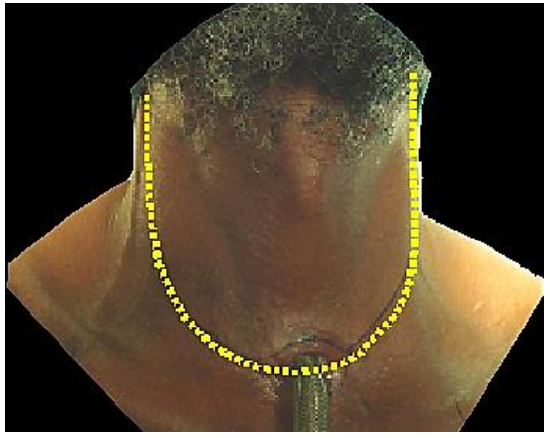
Figure 3a: Wide apron flap to accommodate neck dissections
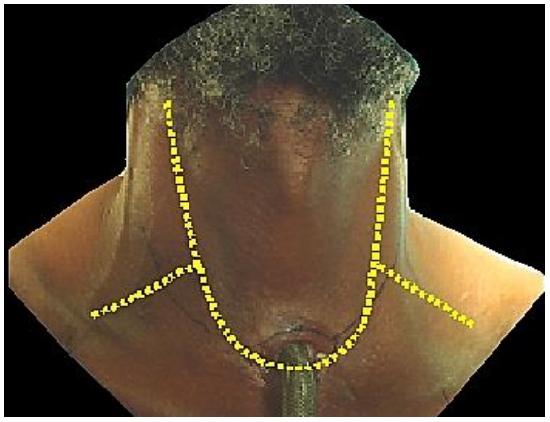
Figure 3b: Narrow apron flap for laryngectomy, with lateral extensions for neck dissections
Flap elevation (Figure 4)
- Cut through the superficial layer of investing fascia and platysma muscles. The platysma is often absent in midline. Take care not to injure the external and anterior jugular veins
- Elevate the apron flap in a subplatysmal plane, remaining superficial to the external and anterior jugular veins
- Dissect the flap superiorly up to approximately 2 cm above the body of the hyoid bone
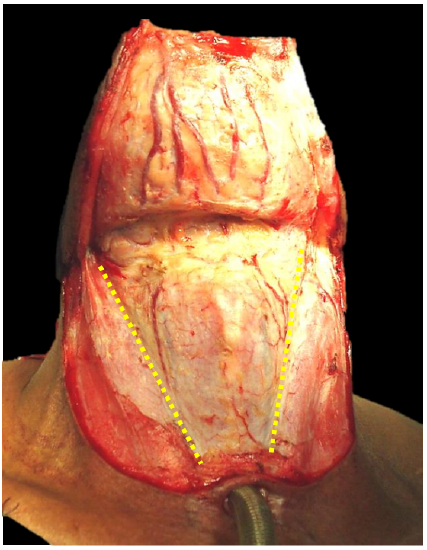
Figure 4: Elevated apron flap and incisions through investing layer of cervical along anterior borders of sternocleidomastoid muscles
Freeing up the larynx
- Free up one side of the larynx at a time
- Stand on the side of neck that is being dissected
- Ligate and transect the anterior jugular veins suprasternally and above the hyoid
- Incise the investing layer of cervical fascia along the anterior border of the sternocleidomastoid muscle (Figure 4)
- Retract the sternocleidomastoid muscle laterally
- Identify the sternohyoid and omohyoid muscles
- Transect the omohyoid muscle medial to where it crosses the internal jugular vein (Figure 5)
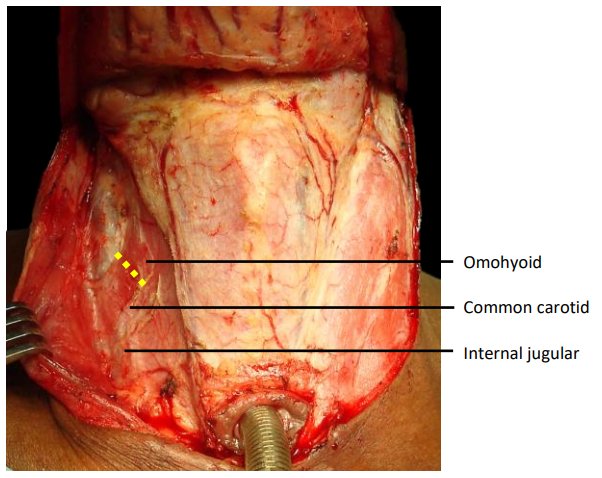
Figure 5: Transect omohyoid along yellow line
- Identify the dissection plane between carotid sheath, and larynx and thyroid gland and open this plane with sharp and blunt finger dissection to expose the prevertebral fascia (Figure 6)
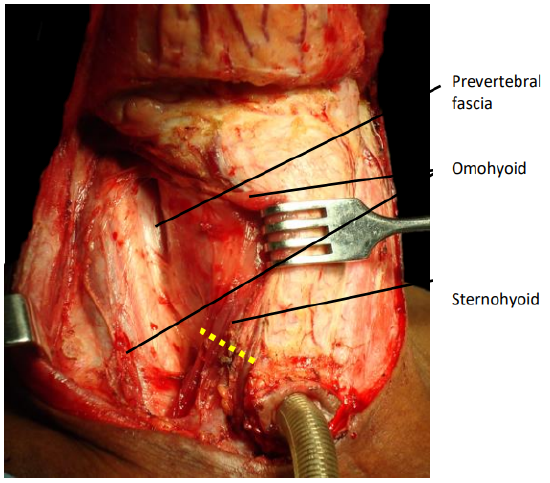
Figure 6: Transect sternohyoid muscle to expose sternothyroid muscle
- Transect the sternohyoid muscle with electrocautery wherever convenient (Figure 6)
- Identify the sternothyroid muscle and carefully divide it below larynx (Figure 6). It is a broad, thin muscle, so take special care not to injure the thyroid gland and its rich vasculature which is immediately deep to muscle
- Carefully elevate and reflect the superior cut end of the sternothyroid muscle from the thyroid gland using electrocautery dissection (Figure 7)
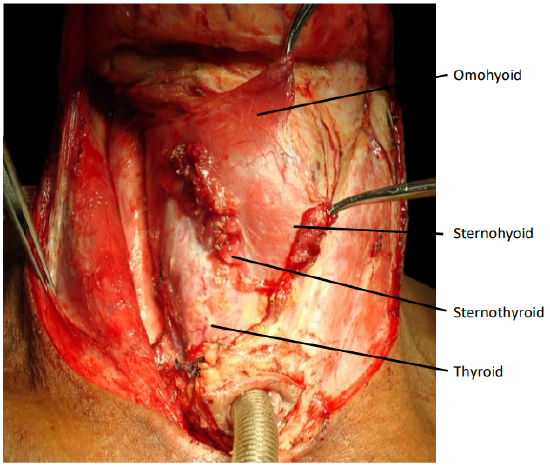
Figure 7: Transect & elevate sternothyroid to expose thyroid gland
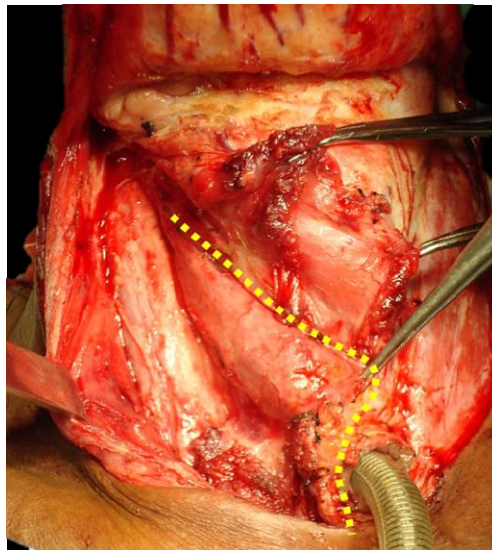
Figure 8: Divided sternothyroid retracted to expose thyroid. Line indicates course of dissection of thyroid gland and along midline of trachea
- Divide the thyroid isthmus with electrocautery
- Divide and strip the tissues overlying the cervical trachea vertically in the midline to avoid injuring the inferior thyroid veins
- Carefully reflect the thyroid lobe off the trachea, cricoid and inferior constrictor with electrocautery (Figure 9) while inspecting for and excluding direct laryngeal tumor extension to the thyroid gland
- Identify and transect the recurrent laryngeal nerve (Figure 10)
- Identify the esophagus and tracheoesophageal groove (Figure 10)
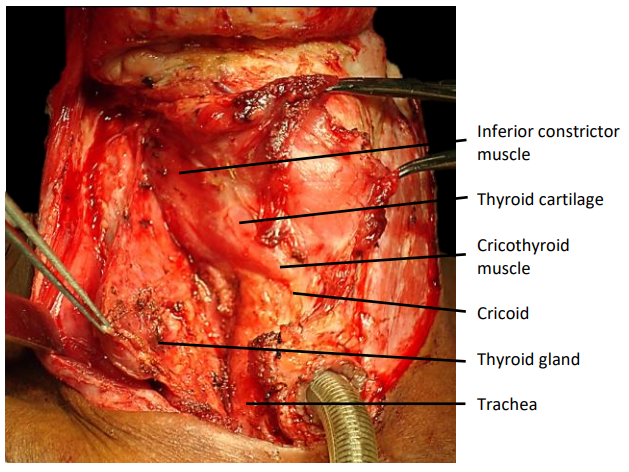
Figure 9: Thyroid gland has been mobilized from larynx and trachea
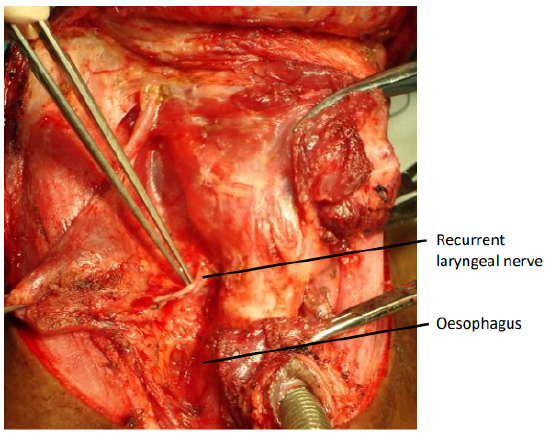
Figure 10: Identify esophagus, and divide recurrent laryngeal nerve
- Identify and divide the superior larynxgeal branch of superior thyroid artery, and reflect and preserve the superior thyroid pedicle from the larynx (Figure 11)
- Identify and divide the superior laryngeal nerve
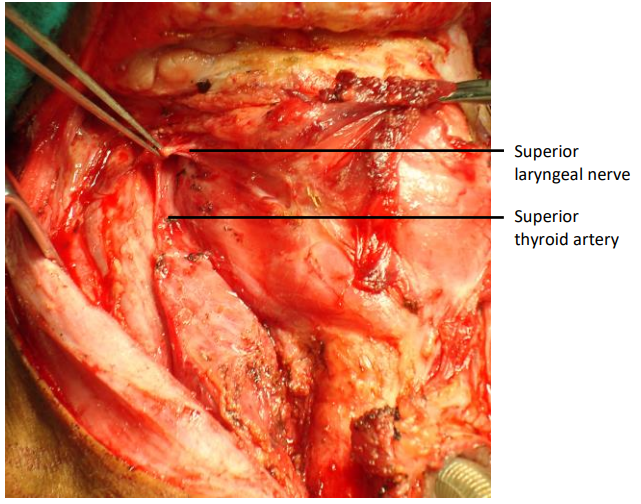
Figure 11: Identify and divide superior laryngeal branch of superior thyroid artery
- Rotate the larynx to the contralateral side, and identify the posterior border of the thyroid ala (Figure 12)
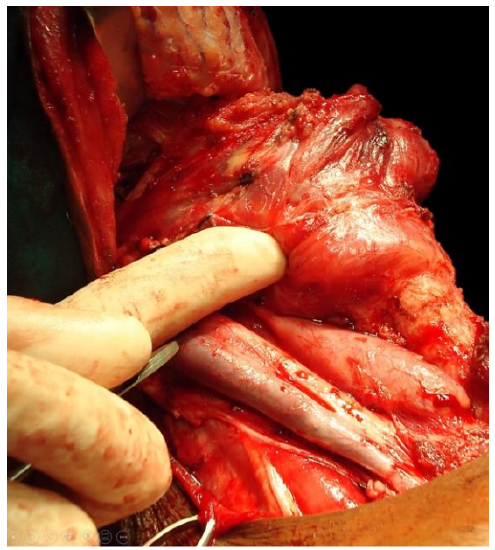
Figure 12: Rotate the larynx with a finger placed behind the thyroid ala
- Divide the inferior pharyngeal constrictor muscle and thyroid perichondrium with electrocautery at, or just anterior to the posterior border of the thyroid ala (Figure 13)
- Strip the lateral wall of the pyriform fossa off the medial aspect of the thyroid ala in a subperichondrial plane with a swab/sponge held over a fingertip, or with a Freer’s elevator, only on the side of the larynx opposite to the cancer (Figure 14). On the side of the cancer, this step is omitted to ensure adequate resection margins.
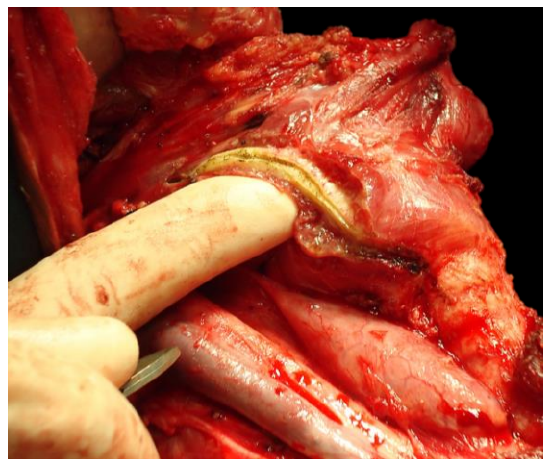
Figure 13: Divided inferior pharyngeal constrictor and thyroid perichondrium
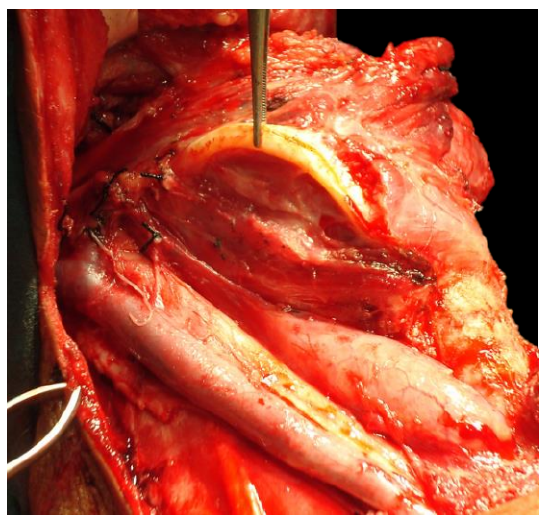
Figure 14: Pyriform fossa mucosa stripped from thyroid lamina
The surgeon then crosses to the opposite side of the patient and repeats the above operative steps.
Suprahyoid dissection
The following description applies to laryngeal cancer not involving the pre-epiglottic space, vallecula or base of tongue. When tumor does involve vallecula, pre-epiglottic space and/or base of tongue, then the pharynx is entered via the opposite pyriform fossa or a retrograde laryngectomy is done, commencing the dissection inferiorly at the tracheostomy (see later)
- Identify the body of the hyoid bone
- Remember that the hypoglossal nerves and lingual arteries lie just deep to the greater cornua/horns of the hyoid bone
- Divide the suprahyoid muscles with electrocautery along the superior border of the body of the hyoid bone (Figure 15)
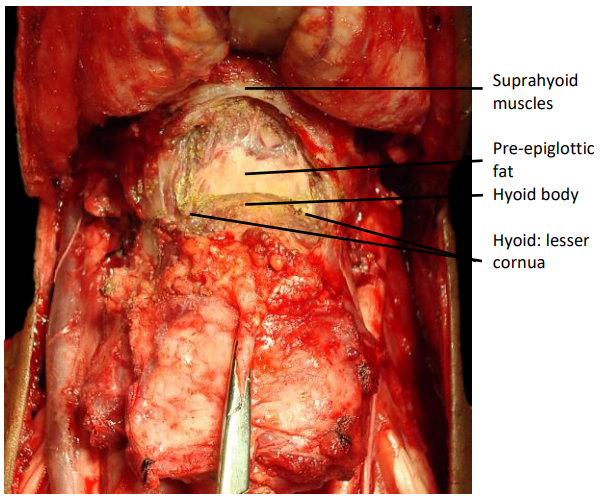
Figure 15: Transection of suprahyoid muscles from hyoid body
- Initially do not dissect lateral to the lesser cornua, as the hypoglossal nerves and the lingual arteries are located deep to the greater cornua of the hyoid bone
- Release the digastric tendon and stylohyoid ligament and muscle from the lesser cornu of the hyoid. The hyoidthen become more mobile and can be retracted inferiorly, away from the hypoglossal nerves
- Rotate the hyoid bone to the contralateral side, and identify the position of the greater cornu/horn of the hyoid bone (Figure 16)
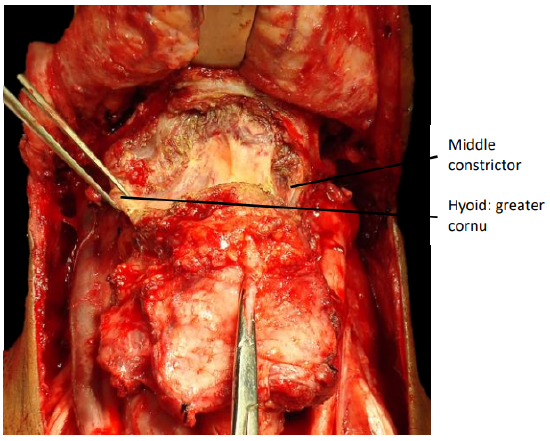
Figure 16: Identify greater cornu
- The hyoglossus and middle constrictor muscles are next released from the greater cornu with diathermy (Figure 16)
- Divide the soft tissue on the medial aspect of the tips of the greater cornua of the hyoid with scissors to free the greater cornua of the hyoid bilaterally (Figure 17). Hug the inner aspect of the greater cornua to avoid the hypoglossal nerves. If a neck dissection has been done, the hypoglossal nerves will already be visible
- Dissect transversely with diathermy along the superior margin of the body of the hyoid bone, and along the superior margin of the pre-epiglottic space
- Identify the hyoepiglottic ligament in the midline
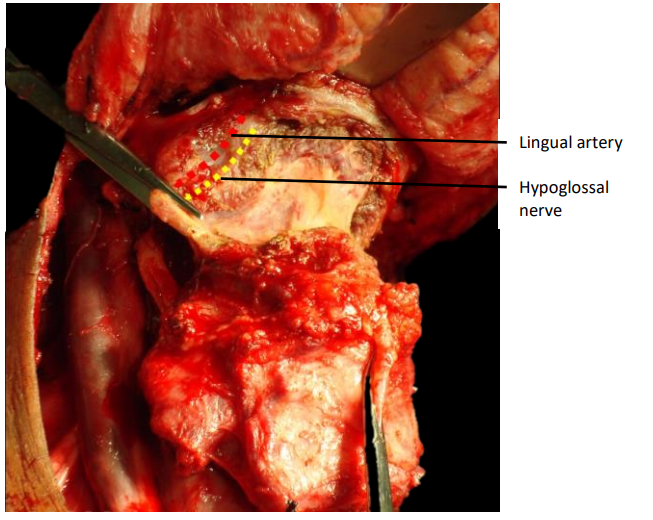
Figure 17: Releasing greater cornu
- Dissect along the hyoepiglottic ligament and strip the vallecular mucosa from the anterior surface of the epiglottis (Figure 18)
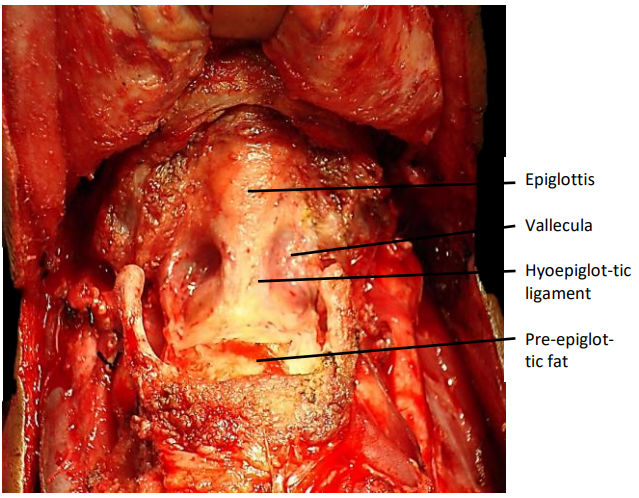
Figure 18: Suprahyoid approach to valleculae
- Enter the pharynx by incising the mucosa along the superior margin of the epiglottis (Figure 19)
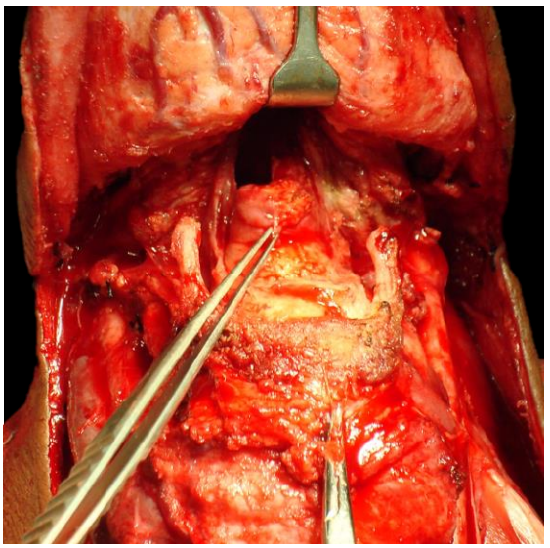
Figure 19: Entering vallecula
Tracheostomy
- A tracheostomy is done at this stage to mobilize the larynx and to facilitate the laryngeal resection
- Ask the anesthetist to preoxygenate the patient
- Incise the trachea transversely between the 3rd/4th/5th tracheal rings or below a preoperative tracheostomy
- With a small trachea, incise the lateral tracheal walls in a superolateral direction to bevel and enlarge the tracheostoma
- Place a few 3-0 vicryl half-mattress sutures between the anterior wall of the transected trachea and the skin to approximate mucosa to skin
- Puncture and deflate the cuff of the endotracheal tube, and cut the tube in the pharynx, and remove the distal end of the tube through the pharyngotomy
- Insert a flexible endotracheal tube e.g. armoured tube into the tracheostoma. Avoid inserting the tube too deeply as the carina is quite close to the tracheostoma. Fix the tube to the chest wall or drapes with a temporary suture so that it does not become displaced, attach the sterile anesthesia tubing and resume ventilation
Laryngeal resection
- Inspect the subglottis through the tracheostoma to ensure that the tracheal tumor resection margin is adequate
- Move to the head of the operating table
- Retract the epiglottis and larynx anteriorly through the pharyngotomy, and inspect the larynx and the tumor
- Commence laryngeal resection contralateral to the tumor using curved scissors with points located anteriorly/ upwards to avoid inadvertently resecting too much pharyngeal mucosa
- Cut along the lateral border of the epiglottis on the less involved side, to expose the hypopharynx
- Repeat this on the side of tumor with at least a 1 cm mucosal margin around the tumor
- On the less involved side, cut through the lateral wall of the pyriform fossa and hug the arytenoids and cricoid to preserve pyriform sinus mucosa (Figure 20). The superior laryngeal neurovascular pedicle is transected if not previously addressed
- Repeat on the tumor side
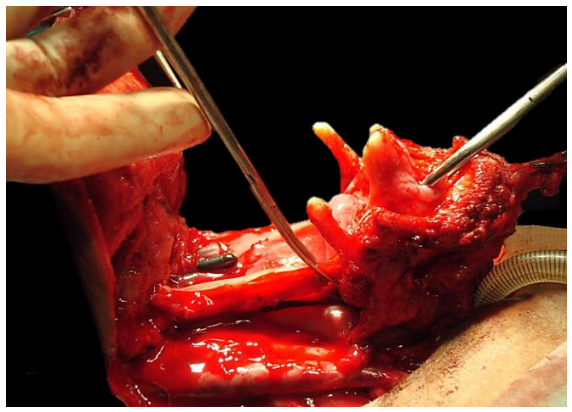
Figure 20: Resect the larynx preserving maximum amount of pharyngeal mucosa
- Join the left and right pyriform incisions by tunneling below and cutting the postcricoid mucosa transversely (Figure 21)
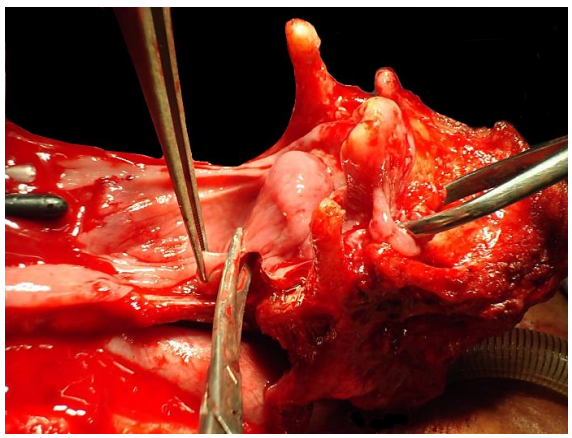
Figure 21: Transverse postcricoid cut
- Separate the posterior wall of the larynx (cricoid, tracheal membrane) from the anterior wall of the esophagus by dissecting with a scalpel along the avascular plane between that exists between esophagus and trachea/cricoid (Figure 22). Take care to stop just short of the tracheostoma.
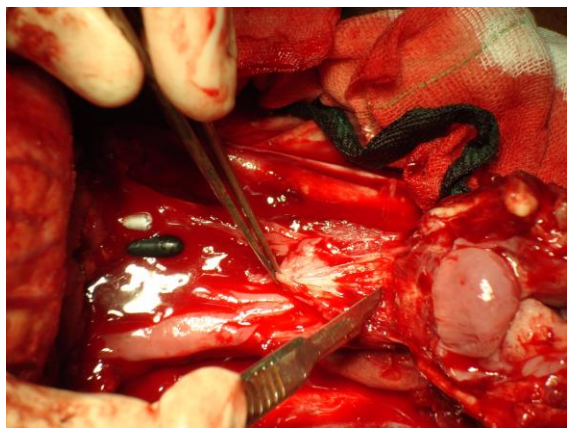
Figure 22: Dissecting in the avascular plane between esophagus and trachea
- Transect the posterior wall of the trachea, and remove the larynx (Figure 23)
- Inspect the laryngectomy specimen for adequacy of resection margins, and resect additional tissue if indicated
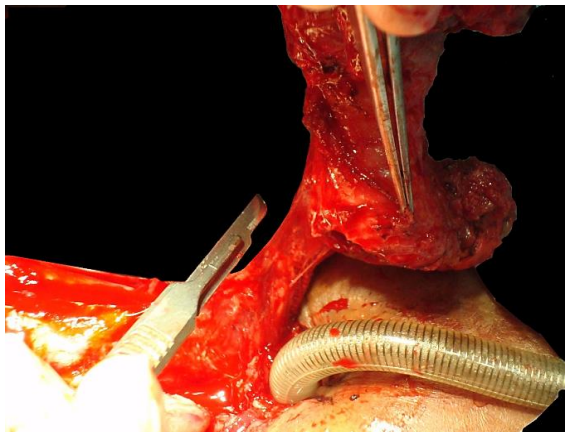
Figure 23: Transect trachea and remove larynx
Retrograde laryngectomy
- This involves commencing the laryngeal resection inferiorly at the tracheostomy site; it is recommended when tumor involves the pre-epiglottic space and/or base of tongue, to ensure an adequate suprahyoid resection margin. Some surgeons routinely do retrograde laryngectomy
- Free the hyoid bone and the lateral borders of the thyroid cartilage as described above
- Incise the trachea at about the level of the 3rd/4th tracheal rings, insert an armored endotracheal tube and remove the orotracheal tube (Figure 24)
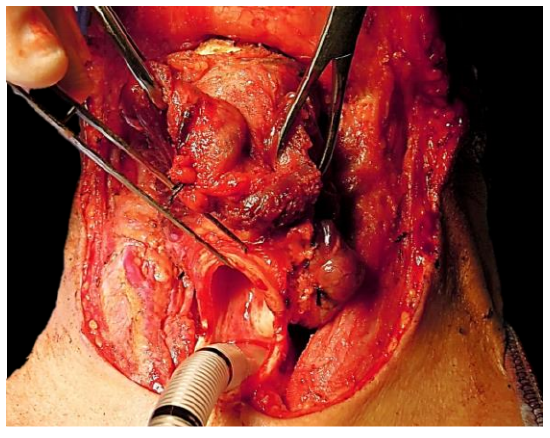
Figure 24: Trachea incised
- Transect the thin membranous posterior tracheal wall (Figure 25)
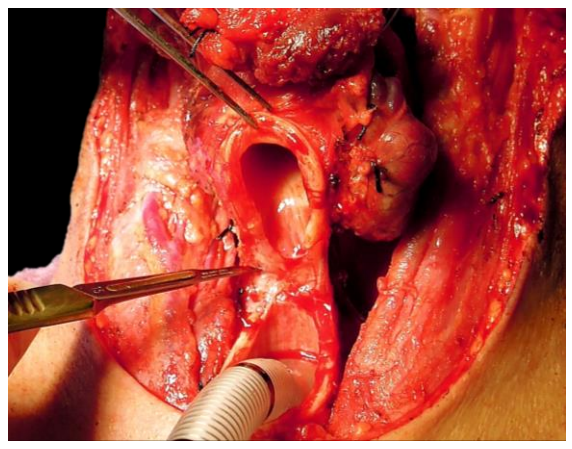
Figure 25: Transecting posterior tracheal wall to expose anterior wall of esophagus
- Find the dissection plane between trachea and esophagus and dissect cephalad in this well-defined plane with a scalpel until the posterior aspect of the cricoid and the posterior cricoarytenoid muscles come into view (Figure 26)
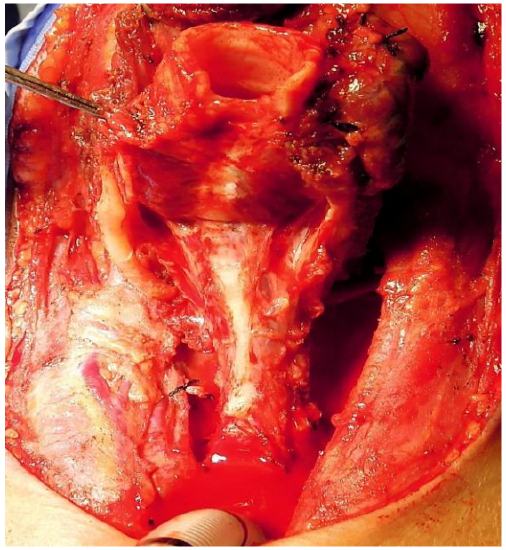
Figure 26: Esophagus, thyroid laminae, cricoid and posterior cricoarytenoid muscles exposed
- Transversely incise the pharyngeal mucosa about 1 cm below the upper border of the cricoid lamina to enter the postcricoid hypopharynx (Figure 27)
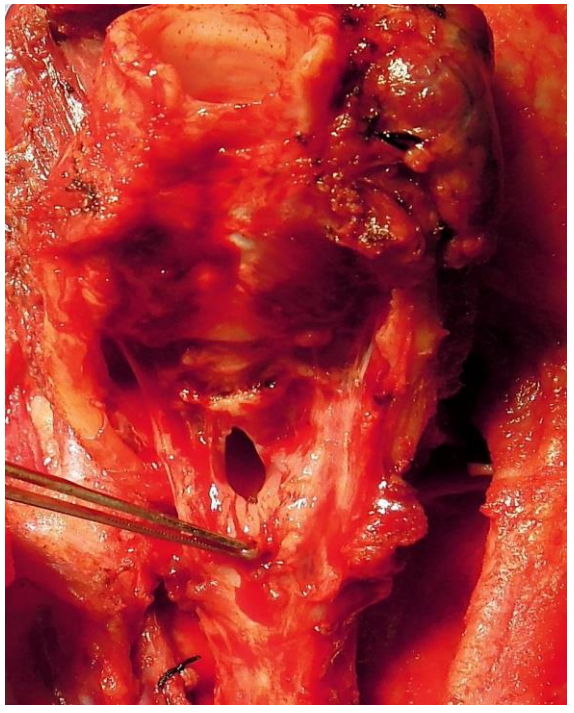
Figure 27: Entering the postcricoid area of the pharynx
- Extend the incision to the pyriform fossa contralateral to the cancer
- Once the cancer can be seen through the pharyngotomy, incise the pyriform fossa mucosa on the involved side
- By placing an index finger across the vallecula to palpate the upper extent of the cancer one can proceed to transect the base of tongue with an adequate margin
Pharyngo-esophageal myotomy
- Optimizing speech and swallowing requires a capacious and floppy pharynx
- Always perform a pharyngoesophageal myotomy to prevent hypertonicity of the pharyngoesophageal segment
- Insert an index finger into the esophagus (Figure 28)
- With a sharp scalpel, divide all the muscle fibers down to the submucosa, and distally to the level of the tracheastoma (Figure 28). The myotomy may be done in the midline or to the side

Figure 28: Cricopharyngeal myotomy
Tracheo-esophageal fistula
- Tracheo-esophageal speech is the best form of alaryngeal communication
- A tracheo-esophageal fistula is created before closing the pharynx
- Pass a curved artery forceps through the pharyngeal defect along the esophagus and tent up the anterior wall of esophagus/posterior tracheal wall 5-10 mm below the superior margin of the tracheostoma. Placing the fistula too low makes changing the prosthesis difficult
- Cut down onto the tip of the artery forceps with a scalpel, and pass the tip of the forceps through the fistula into the tracheal lumen
- Hold the tip of a 14-gauge Foley urinary catheter with the artery forceps and pull the catheter through the fistula into the esophagus and pass it through the pharyngeal defect (Figure 29). Then advance the catheter down the esophagus. Avoid accidental displacement of the catheter by injecting 5 mL water into the bulb and by fixing the catheter to the skin with a suture
- The catheter acts as a stent to allow the fistula to mature in preparation for fitting a tracheo-esophageal prosthesis, and is initially used for stomagastric feeding
- An alternative method is to insert a speech prosthesis ab initio, and to feed the patient via a nasogastric tube, or a catheter passed through the speech prosthesis (Postlaryngectomy vocal and pulmonary rehabilitation)
- Divide the sternal heads of the sternomastoid muscles to create a flattened peristomal contour and to facilitate digital stomal occlusion (Figure 30).
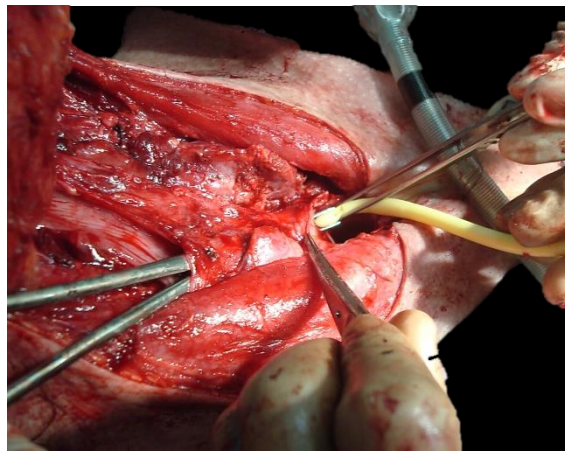
Figure 29: Creation of tracheo-esophageal fistula
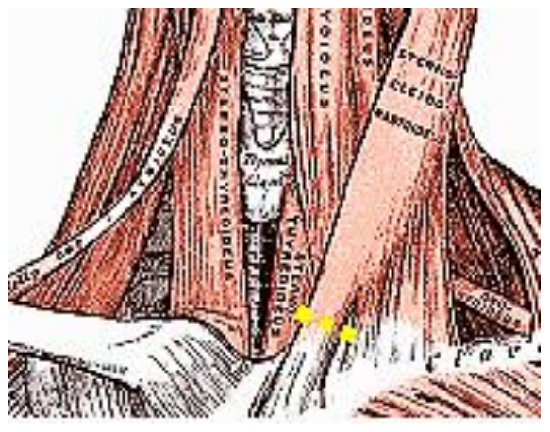
Figure 30: Division of sternal heads of sternomastoid to flatten peristomal area
Pharyngeal closure
- At least 2.5 cm transverse diameter of residual pharyngeal mucosa is required for primary pharyngeal closure. The teaching that the minimum pharynx required is that which may be closed over a nasogastric tube is incorrect, as the neopharynx is then too narrow for adequate swallowing and voicing
- A horizontal/transverse closure is preferred as it maximizes the capacity of the pharynx (Figures 31). Only if there is undue tension on the suture line, then do T-shaped closure, keeping the vertical limb as short as possible
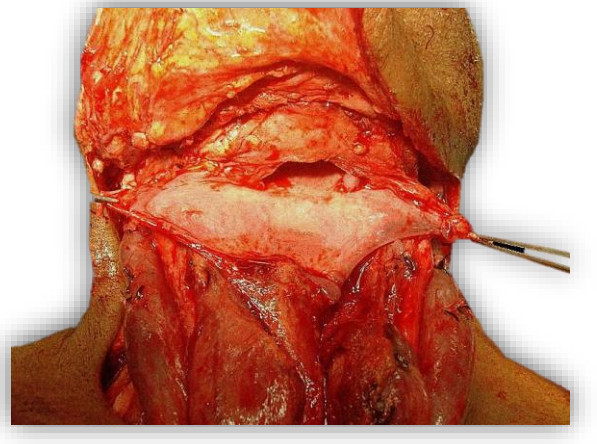
Figure 31: Pharynx well-suited to a transverse closure
- Take care not to injure the lingual arteries when suturing the pharynx, as injury to the arteries may lead to necrosis of the tongue
- A 3-layered pharyngeal closure is suggested (Video)
- 1st layer: 3-0 vicryl running modified Connell or true Connell technique (Invert mucosa) (Figure 32)
- 2nd layer: 3-0 vicryl running suture of submucosa and muscle
- 3rd layer: Approximate inferior constrictors and suture constrictors to suprahyoid muscles with interrupted 3-0 vicryl
Final steps
- Ask the anesthetist to do a Valsalva manoeuvre to detect bleeding and a chyle leak
- If there is excessive, lax suprastomal skin that may occlude the tracheostomy when the patient flexes the neck, then trim a crescent of suprastomal skin from the edge of the apron flap
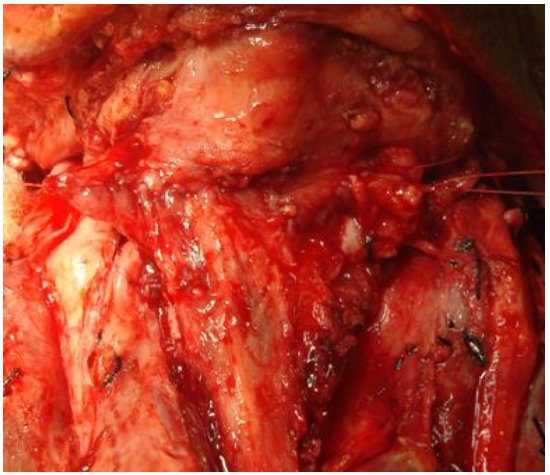
Figure 32: Completed 1st layer of transverse closure of pharynx
- Suture the skin to the edge of the tracheostomy with half-mattress interrupted 3-0 vicryl sutures
- Seal the trifurcation at the lateral edge of the stoma with a suture as indicated below (Figure 33)
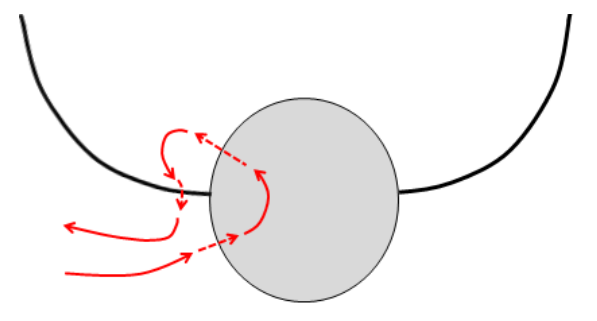
Figure 33: Suture technique to seal trifurcation between skin and side of tracheostoma
- Insert a ¼” suction drain
- Irrigate neck with sterile water
- Reapproximate the platysma with 3-0 vicryl running sutures
- Close the skin with a running nylon suture or with skin staples
- Suction blood from trachea
- Insert a cuffed tracheostomy tube, and suture it to skin
Postoperative care
- Antibiotics x 24 hours
- Omeprazole (20mg/day) via Foley or mouth x 14 days to reduce risk of developing pharyngocutaneous fistulae (See references)
- Chest physiotherapy
- Remove suction drains when <50 mL drainage per 24 hours (See references)
- Day 1: Mobilize to chair, remove urinary catheter
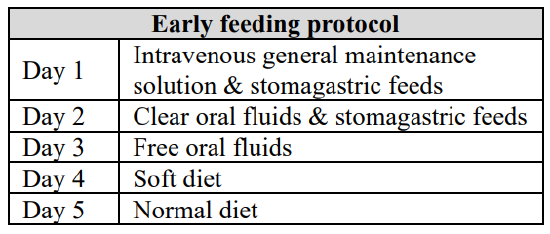
- Day 2: Commence oral feeding. Early oral feeding is safe, and does not cause pharyngocutaneous fistulae (See references)
- Day 7: Remove sutures
- Day 10: Insert speaking valve; no anesthetic required (Figures 34, 35)
- Cover the stoma with a bib (Figure 36)
Pharyngeal reconstruction
Following resection of large pyriform fossa tumours (Figure 37) or tumors that extend close the cricopharyngeus, or involve the postcricoid area, only a narrow strip of mucosa may remain to reconstruct the neopharynx. If the residual pharyngeal mucosa is <2.5 cm in width, then additional tissue is required to avoid pharyngeal stenosis, dysphagia and poor speech (Figure 38). Reconstructive options include pectoralis major, latissimus dorsi and supraclavicular flaps, or microvascular free tissue transfer flaps (radial forearm, anterolateral thigh).
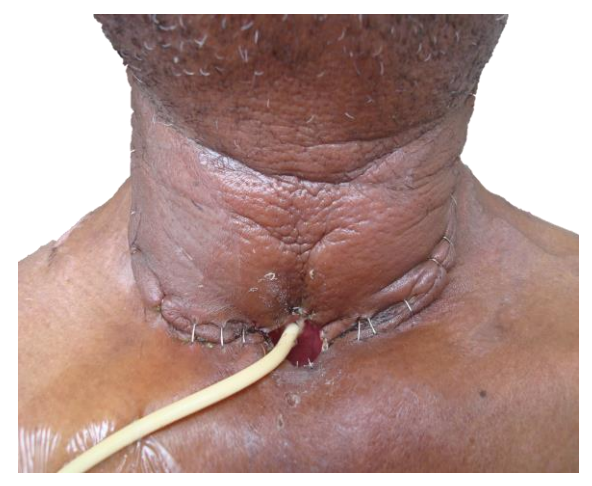
Figure 34: Stoma and Foley catheter feeding tube one week following surgery

Figure 35: Speaking valve

Figure 36: Bib
All these flaps can be used to augment the pharyngeal repair, or when the pharynx has been completely resected, may be tubed to entirely replace the pharynx (Figures 39 – 42).
Following pharyngeal reconstruction with a flap, a contrast swallow X-ray is done on about day 7 to exclude an anastomotic leak before commencing oral feeding.
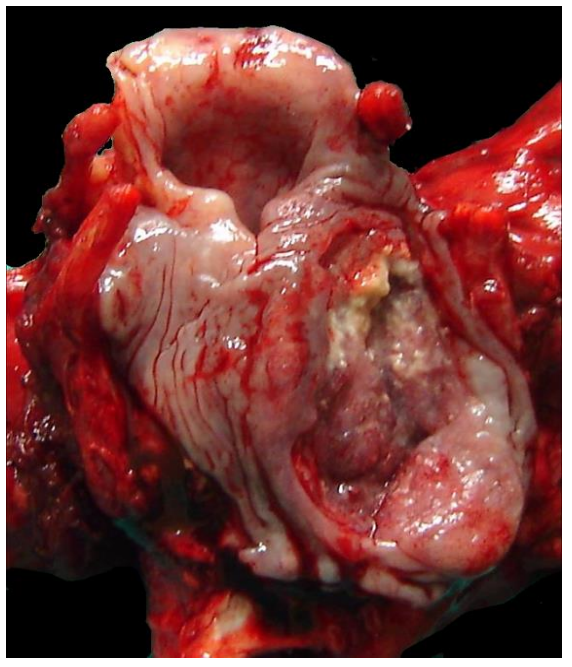
Figure 37: Large carcinoma of hypo-pharynx that requires pharyngeal reconstruction
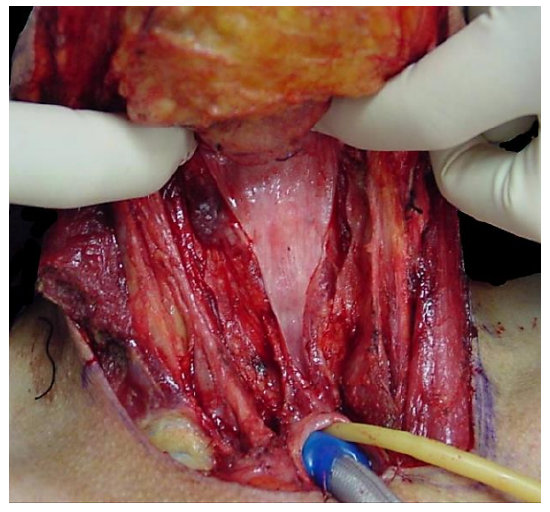
Figure 38: Insufficient pharyngeal mucosa for primary closure of pharynx
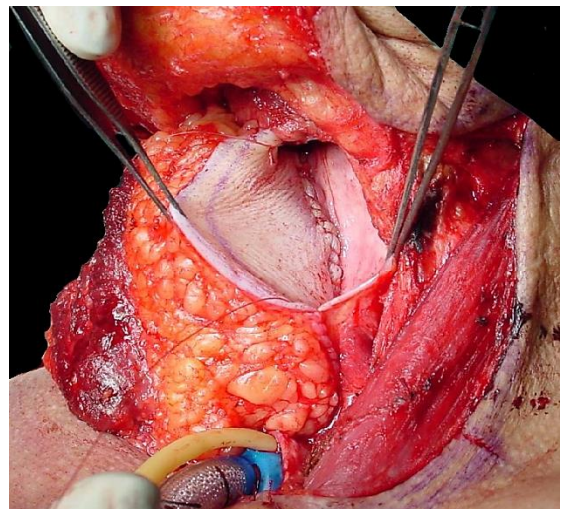
Figure 39: Pectoralis major augmentation of pharynx
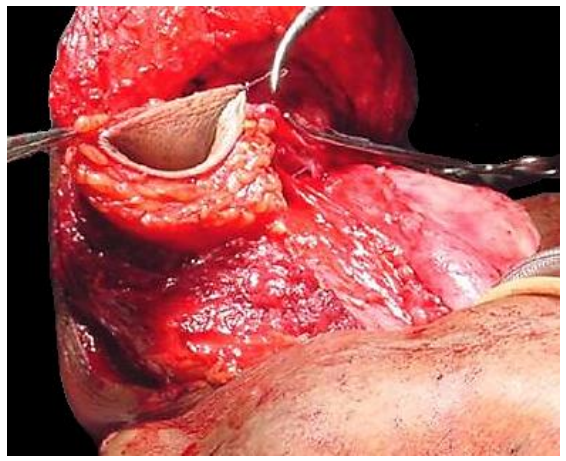
Figure 40: Tubed pectoralis major flap
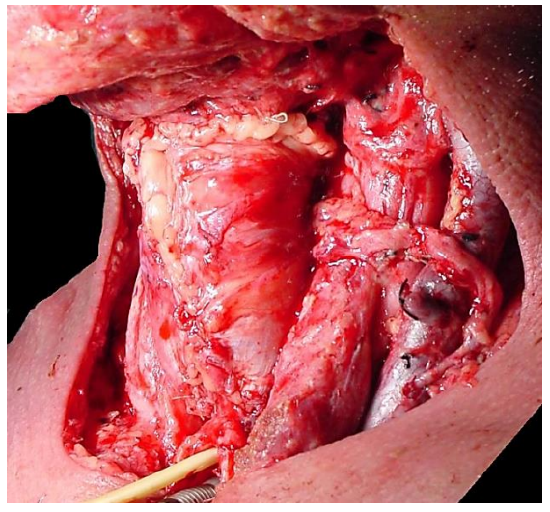
Figure 41: Tubed anterolateral thigh flap
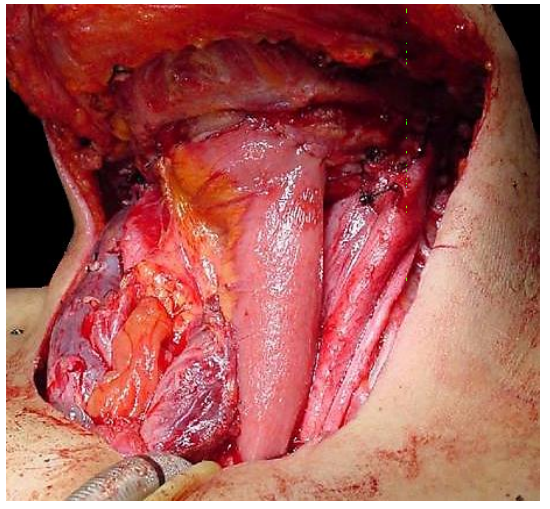
Figure 42: Free jejunal flap
Useful references
- Stephenson K, Fagan JJ. The effect of perioperative proton pump inhibitors on the incidence of pharyngocutaneous fistula following total laryngectomy: a prospective randomized controlled trial. Head Neck 2015 Feb;37(2):255-9
- Aswani J, Thandar MA, Otiti J, Fagan JJ. Early oral feeding following total laryngectomy. J Laryngol Otol. 2009; 123:333-338
- A practical guide to post-laryngectomy vocal and pulmonary rehabilitation - Fourth Edition: Postlaryngectomy vocal and pulmonary rehabilitation
- Fagan JJ, Lentin R, Oyarzabal MF, S Iaacs, Sellars SL. Tracheoesophageal speech in a Developing World Community. Arch Otolaryngol 2002, 128 (1): 50-3
- Fagan JJ, Kaye PV. Management of the thyroid gland with laryngectomy for cT3 glottic carcinomas. Clin Otolaryngol, 1997; 22: 7-12
- Harris T, Doolarkhan Z, Fagan JJ. Timing of removal of neck drains with head and neck surgery. Ear Nose Throat J. 2011 Apr; 90(4):186-9
- Fagan JJ, Lentin R, Quail G. International Practice of Laryngectomy Rehabilitation Interventions - A Perspective from South Africa. Curr Opin Otolaryngol Head Neck Surg. 2013 Jun;21(3):199-204
- Quail G, Fagan JJ, Raynham O, Krynauw MH, John LR, Carrara MH. The effect of cloth stoma covers on tracheal climate of laryngectomy patients. Head Neck. 2016 Apr;38 Suppl 1:E480-7
Clinical Practice Guidelines
- Cancer of Glottis: https://developingworldheadandneckcancerguidelines.com/index-page-glottic-cancers/
- Cancer of Supraglottis: https://developingworldheadandneckcancerguidelines.com/index-page-supraglottic-cancers/
- Cancer of Hypopharynx: https://developingworldheadandneckcancerguidelines.com/index-page-hypopharyngeal-cancers/
Author & Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za

The Open Access Atlas of Otolaryngology, Head & Neck Operative Surgery by Johan Fagan (Editor) johannes.fagan@uct.ac.za is licensed under a Creative Commons Attribution - Non-Commercial 3.0 Unported License