
1.3: Histology of the Oral Mucosa
- Page ID
- 41539

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)- Overview
- Skin histology
- Oral mucosa histology:
- Lining mucosa
- Masticatory mucosa
- Dento-gingival mucosa
- Specialized mucosa
- Clinical applications of:
- Lining & masticatory histology
- Dento-gingival histology
- Specialized histology
Chapter overview
We start this chapter reviewing the histology of the skin. The different regions of oral mucosa are similar to the skin because they share the same lineage: ectoderm and mesoderm. There are a few small differences. One unfortunate difference is the names we use for the skin are not the same names we use for oral mucosa. Otherwise, it is faster to focus primarily on the small differences, there is no need to cover the histology of the epidermis or dermis each time. In subsequent chapters on the teeth, pay attention to how the lineage of tooth tissues is different from that of oral mucosa, as well as to how their basic pattern is similar.
For more practice with histology of the oral mucosa (and more), websites worth visiting are:
- The oral histology lab
- by Brian R. MacPherson, Ph.D. and James G. Tieman, Ed.D. at the University of Kentucky College of Medicine.
- The virtual oral histology lab
- By Roger Shore at the School of Dentistry, University of Leeds

Histology of the skin – for comparison
The skin and the oral mucosa share a lot in common because of their shared lineage from ectoderm and mesoderm. Both are composed of a stratified squamous epithelium, just deep to that areolar CT, followed by dense irregular CT. Unfortunately, parts of the skin and oral mucosa receive different names and are classified differently based on their location. That means you have more names to memorize… Boo!
The dermis is the connective tissue layer of the skin. It is composed in part of a layer of dense irregular CT, the old-fashioned name for which is the reticular layer of the dermis. The other part of the dermis is a layer of areolar CT, which has an old-fashioned name, too the papillary layer of the dermis. It received that name for having finger-like dermal papillae on the apical surface, compared to the smoother transition between the papillary and the reticular layer. In Fig 58, the upward-pointing dermal papillae meet downward-pointing rete pegs of the epidermis. The epidermis is composed of stratified squamous epithelial tissue. The dermal papillae of the dermis meet the rete pegs of the epidermis like inter-meshed fingers from two hands, which makes for a strong connection between epidermis and dermis. Some regions of the oral cavity won’t require such a strong connection, and the rete pegs and dermal papillae are smaller or absent. Note that the border between epidermis and dermis is distinct, whereas the border between the reticular and papillary layers of the dermis is blended. That is because the epidermis is derived from the ectoderm, while the two layers of the dermis are derived from the mesoderm.
The epidermis of the skin is highly keratinized. The epithelial cells make a large protein called keratin (or more accurately, keratins, as there are over 50 genes for slightly different keratin molecules), which is similar to collagen, except keratin is not secreted. These long fibrous proteins accumulate within keratinocytes, the principle cell of a stratified squamous epithelium. Epithelial stem cells in the basal layer of the epidermis give rise to new keratinocytes, and as keratinocytes mature, they are pushed towards the apical surface. As the keratinocytes move superficially, they fill up with keratin, and receive fewer nutrients (an epithelium is avascular), until ultimately the keratinocytes at the surface are dead and completely full of keratin. The keratin fibers are cross-linked to each other and to desmosomes, which anchor the dead cells together, making for a very tough and water-resistant barrier. Keratinized regions of oral epithelium are located where there is a lot of abrasion. In the rest of the oral cavity, we want moisture, so there is less or no keratinization.
Skin color
| Pigment | Color | Source | Location |
|---|---|---|---|
| Melanin | red or brown/black | melanocytes | epidermis/oral mucosa |
| Carotene | orange-yellow | diet (plants) | dermis/sub-mucosa |
| Hemoglobin | Red-maroon | blood | Dermis/sub-mucosa |
Table 3.1: The three major skin pigments.
There are 3 major pigments (a molecule that absorbs certain frequencies of visible light) that contribute to skin color, listed in Table 3.1. Keratin has no color, but it can obscure the visibility of the deeper pigment hemoglobin. Melanin levels vary naturally in the skin. Everyone is born with roughly the same number of melanocytes, the cells that synthesize the melanin pigment. Melanocytes are derived from neural crest cells that migrate from the CNS to the deepest layer of the epidermis. They are not anchored to keratinocytes, and their shape more closely resembles neurons or glia than they do epithelial cells. Melanocytes can produce a lighter form of melanin (pheomelanin) or a darker form (eumelanin). After synthesizing melanin, melanocytes transfer it to keratinocytes inside of vesicles (melanosomes). The amount and type of melanin produced has a baseline rate set at birth—this is not regulated by genes we inherit from our parents, but by more complex epigenetic factors.
![[video-to-gif output image]](https://med.libretexts.org/@api/deki/files/22824/video-to-gif-output-image.gif?revision=1)
Environmental changes trigger melanocytes to changes the levels of melanin they produce, and these changes illustrate several functions of melanin. The most obvious function of melanin is to absorb UV light. When UV light causes DNA damage to keratinocytes, this induces them to secrete a hormone (Melanocyte Stimulating Factor) which activates nearby melanocytes to produce more melanin. Extra melanin, when deposited into new keratinocytes, reduces damage to DNA and helps prevent skin cancer. Melanin (in the epidermis) also protects folic acid levels in the blood (the dermis), which can be destroyed by UV light. Folic acid is required for cell division, low levels during pregnancy can lead to congenital malformations of the neural tube (spina bifida).
Melanin may also be present within the oral cavity, despite much lower levels of exposure to UV light. This can be explained because of two more functions of the molecule melanin. Melanin protects tissues against damage from abrasion. Pregnancy leads to an increase in the amount of melanin in the areolas and labia minora, areas more likely to suffer abrasion during or after childbirth than they are to suffer UV damage. A third function of melanin is its ability to bind free radicals. After being transferred to keratinocytes, melanin binds to toxic free radicals, and as keratinocytes are exfoliated removes free radicals from the body.
Two other major skin pigments are hemoglobin and carotene. These are found below the epidermis, higher levels of the darker eumelanin may obscure them. Hemoglobin allows red blood cells to pick up and dump off oxygen molecules. It undergoes a color change when it picks up oxygen, shifting from maroon to red. Healthy people of any skin color do not exhibit variation in hemoglobin. Carotene is an orange pigment molecule made by plants which accumulates in the epidermis. Carotene is converted into Vitamin A, and without Vitamin A human cells cannot make the important morphogen Retinoic Acid. The amount of carotene that accumulates in the skin, along with melanin, contributes to diversity in skin tone, although carotene levels usually do not change in response to environmental factors.

Vermilion border
The vermilion border (or margin, or zone) is usually defined as part of the skin. It contains less keratin, no hair follicles and few or no sebaceous glands. Furthermore, the keratinocytes in the vermilion border synthesize a clear protein (Eleidin), which allows the reddish color of hemoglobin in the capillaries of the dermis and muscle tissue to be more visible in the vermilion zone than in the more highly keratinized neighboring regions of skin.

Hair follicles
Hair follicles share developmental processes with teeth. That gives these appendages of the skin and oral mucosa a similar pattern, only one makes keratin and the other calcium hydroxyapatite. A hair follicle is an invagination (an inward-folding) of the epidermis. The stem cells in the basal layer of the hair bulb divide, differentiate into keratinocytes, and die to form the hair itself. A hair, therefore, is an epithelial structure. Surrounding– or deep to– the hair follicle are the connective tissue layers of the dermis.
Where and when hair follicles invaginate from the surface epidermis is regulated by Planar Cell Polarity signals, which ensure more-or-less even spacing between follicles. Similar signals govern the spacing of the teeth. Also similar to teeth, new hair follicles grow beneath old ones, pushing the old ones out in a process called exfoliation. Of course, hair follicles grow and exfoliate more times than a tooth. Nevertheless, it might be a good idea to keep scientific developments in the hair-loss treatment industry somewhere on your radar, advances there may have applications in some future tooth-growth industry.

Sebaceous glands
Sebaceous glands are oil-producing glands within the skin. They may discharge directly to the surface of the skin, but are mostly associated with hair follicles. The material they secrete, called sebum, is mostly lipids (triglyceride and others). Unlike proteins, these molecules are not synthesized on the rER, modified in the Golgi apparatus nor secreted from vesicles. Instead, sebum accumulates in the cytoplasm and is secreted by destruction of the cell. New glandular cells are produced from stem cells in the basal portion of the gland. The vermilion zone and oral mucosa contain few or no sebaceous glands, but when sebaceous glands are present in these regions, they form benign whitish spots known as Fordyce Spots.

General histology of the oral mucosa
The oral mucosa is the mucous membrane that lines the oral cavity. It shares the same lineage as the skin, and we therefore see the same tissue types in the same order. However, its layers get different names and are classified differently. Based on the 3 major embryonic tissues, the layers of the skin are divided appropriately, but the oral mucosa is divided incorrectly.
First, stratified squamous epithelium and underlying areolar connective tissue are lumped together and called the oral mucosa. The stratified squamous epithelium may be referred to individually as the oral epithelium, and like the epidermis, is derived from the ectoderm. The layer of areolar connective tissue, which is homologous to the papillary layer of the dermis in the skin, is called the lamina propria. It is produced by cells derived from mesoderm. Deep to the oral mucosa, the layer of dense irregular connective tissue is called the sub-mucosa, which is the homologue of the reticular layer of the dermis in the skin. The sub-mucosa is also produced by cells derived from mesoderm.
| Embryonic tissue | Skin | Oral mucosa | ||
|---|---|---|---|---|
| Ectoderm | Epidermis | Stratified squamous epithelium | Stratified squamous epithelium | Oral mucosa |
| Mesoderm | Dermis | Areolar CT | Areolar CT | |
| Dense irregular CT | Dense irregular CT | Sub-mucosa |
Table 3.2: Summary of the layers of the skin compared to the layers of the oral mucosa

The amount of keratinization of the oral mucosa reflects the amount of stress or abrasion that region experiences. This is similar to the formation of a callus on the hands or feet. Higher-than-normal levels of keratinization are clinically relevant when they indicate bruxism, tobacco use, or other health-related issues. Keratin doesn’t have a color, but higher levels of keratin in the epithelium obscures the maroon-ish color of blood found within the sub-mucosa, hence non-keratinized mucosa look more reddish, while keratinized mucosa more whitish. Levels of keratinization are categorized into three or four groups listed in Table 3.3.
| Type of stratified squamous epithelium | Level of keratinization | Location |
|---|---|---|
| Keratinized | Full | Skin |
| Ortho-keratinized | Partial | Masticatory mucosa |
| Para-keratinized | ||
| Non-keratinized | None | Lining mucosa |
Table 3.3: Different types of oral mucosa and their level of keratinization
Histology of oral mucosa

3 classes oral mucosa
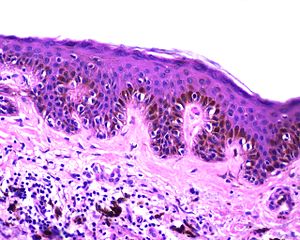
Lining mucosa is found in most regions of the oral cavity, and is not involved significantly with mastication. These are regions more important for speech and swallowing. They are therefore mostly non-keratinized. They may have higher levels of elastic fibers within the lamina propria. Because lining mucosa does not get as much friction and abrasion, it has small or no visible dermal papillae and rete pegs between the epithelium and connective tissue layers. The upper-half of Fig. 3.9 illustrates a lining mucosa.
Masticatory mucosa is found in regions of high abrasion caused by mastication, such as the attached gingiva. The epithelium is either be ortho-keratinized or para-keratinized, which are both partially keratinized. An ortho-keratinized epithelium contains keratinocytes with keratin and nucleuses, whereas the para-keratinized epithelium lacks nucleuses. Differentiating between ortho- and para-keratinized tissue is based on appearance, and has no clinical significance. For the rest of this book, we refer to them together as “ortho- or para-keratinized epithelium”. Because this mucosa is generally under higher levels of stress, it has more pronounced dermal papillae and rete pegs than lining mucosa. The lower-half of Fig. 3.9 illustrates a masticatory mucosa, whose apical surface contains a degree of keratinization.
Specialized mucosa is found on the dorsal surface of the tongue. It does not display a uniform level of keratinization.
Lining mucosa, by region

Labial and buccal mucosa
Labial mucosa and buccal mucosa both have a non-keratinized stratified squamous epithelial layer. This gives them a more reddish or pinkish baseline appearance (see alveolar mucosa pigmentation below). As with all oral mucosa, there are no hair follicles, but in places sebaceous glands may be present, forming Fordyce spots. As a lining mucosa, the epithelial layer is generally non-keratinized, but there can be regions of keratinization where stress occurs. Most notably is likely the Linea Alba (or “white line”), running along the line in the buccal mucosa where the teeth meet.

Ventral surface of the tongue and the floor of the mouth
The ventral surface of the tongue and the floor of the mouth both contain very thin, non-keratinized stratified squamous epithelium. The thin-ness gives these surfaces a more reddish-appearance than other lining mucosa. The thinness of the epithelium, coupled with the rich blood supply in the deeper lamina propria are also why some medications are given sub-lingually.

Soft palate
The soft palate is lined by a non-keratinized stratified squamous epithelium, with a very thin layer of sub-mucosa deep to it. This gives the epithelium a firm attachment to deeper muscle tissue, which is important for speech and swallowing.

Alveolar mucosa
Alveolar mucosa is lined by a non-keratinized stratified squamous epithelium. It has a rich blood supply and numerous elastic fibers within the lamina propria, but few dermal papillae and rete pegs. Because of the large blood supply and low levels of keratin, you may often hear healthy attached gingiva should appear pinkish, but this assumes the absence of melanin.

Clinical disorders may alter the coloration of the gingiva, but to assume all healthy gingiva are pinkish ignores healthy variation in skin color. The gingiva of darker-skinned patients may be darker and be completely healthy. Melanin can be deposited in gingival mucosa, either uniformly (evenly) or focally (localized, such as a freckle or macule– a freckle on the labia). Unlike tanning, which represents a change in melanocyte activity in response to UV damage to keratinocytes, melanin in the gingiva rarely represents a homeostatic change (hence, not a pathological change). Instead, melanin levels in the oral mucosa are linked to inborn melanin level in the skin (the patient’s skin color), a concept that should hopefully be more obvious once we consider the shared lineage of these two tissues.
Masticatory mucosa

Attached gingiva
Attached gingiva is a type of masticatory mucosa, lined with a para-keratinized stratified squamous epithelium. The increased amount of keratin, compared to alveolar mucosa, obscures the underlying blood supply, creating a lighter appearance (which can be described as whitish in the absence of melanin).

Large dermal papillae and rete pegs create the stippled (rough surface) appearance of the attached gingiva.

Interdental gingiva
Interdental gingiva is similar to the attached gingiva.

Marginal gingiva
Marginal gingiva is similar to the attached gingiva.

Hard palate
The hard palate is lined by an ortho-keratinized stratified squamous epithelium and mostly lacks a sub-mucosa, making for a rigid connection to underlying bone tissue.
Mucosa of the Dento-Gingival junction

Sulcular epithelium
Sulcular epithelium (or crevicular epithelium) is lined by either a non-keratinized or para-keratinized stratified squamous epithelium. It creates a space between the gingiva and tooth, named the gingival sulcus. Sulcular epithelium is not attached to the surface of the tooth. Under the microscope, the absence of dermal papillae and rete pegs indicates this tissue gets very little abrasion.

Junctional epithelium
Junctional epithelium (JE) is a non-keratinized stratified squamous epithelium. It is special in that its apical surface attaches to the tooth by way of hemi-desmosomes. Other epithelia attach to connective tissue only on their basolateral surface, their apical surface faces the external environment. This unique attachment to the tooth surface is referred to as the epithelial attachment (EA). This uniqueness is challenging to re-create with dental implants. In a subsequent chapter, we cover the special lineage of the junctional epithelium that gives the adult tissue its uniqueness.
Junctional epithelium is thinner than other gingival mucosa, only five cells thick at the end. It is are also more permeable, having fewer desmosomes between cells. This allows white blood cells from the underlying vascular sub-mucosa to migrate through junctional epithelium and enter the gingival sulcus. But this also increases the potential for oral cavity bacteria to do the same in reverse, especially if the epithelial attachment is lost.
Specialized mucosa

Tongue histology
The dorsal surface of the tongue contains more than one type of mucosa. The epithelial surface is mostly an ortho-keratinized stratified squamous epithelium, and can therefore be thought of as a masticatory mucosa. Scattered across the dorsal and lateral surfaces are four different shapes of bumps called lingual papillae. The most numerous are filiform papillae, which contain only keratinocytes, and may be ortho- or para keratinized. The other three lingual papillae also contain taste buds, which are not keratinocytes, and therefore not a masticatory or lining mucosa, but a specialized mucosa. These structures are appendages of the oral mucosa.
Anteriorly, deep to the oral mucosa and sub-mucosa, the tongue contains numerous bundles of skeletal muscle tissue, and some adipose tissue. Posteriorly, the tongue contains more adipose and salivary gland tissue.
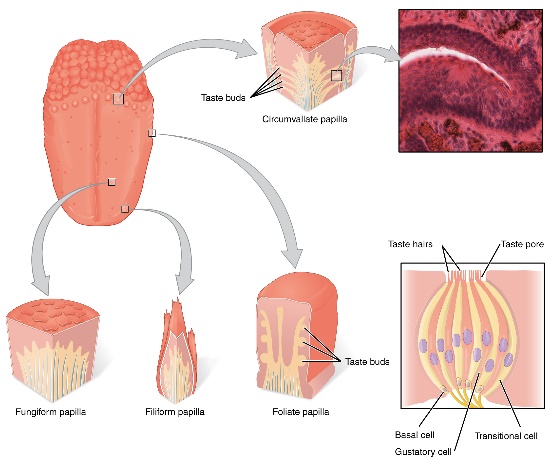
Filiform papillae contain an ortho-keratinized or para-keratinized epithelial layer. These papillae function for providing friction only, their mucosa contain no taste buds.
Fungiform papillae contain an ortho-keratinized or para-keratinized epithelial layer over a highly vascular sub-mucosa, giving these structures a more reddish-appearance than neighboring filiform papillae. The epithelial layer contains taste buds, which detect the sense of gustation, which is in turn a part of the perception of taste.
Foliate papillae are found on the lateral edges of the tongue. They contain an ortho-keratinized or para-keratinized epithelial layer with taste buds.
Circumvallatepapillae are found at the border between the anterior and posterior portion of the tongue, the sulcus terminalis. They contain an ortho-keratinized or para-keratinized epithelial layer with taste buds and minor salivary glands.
Turnover time of epithelia
| Epithelium | Turnover time (days) |
|---|---|
| Skin | 27-38 |
| Hard palate | 24 |
| Floor of mouth | 20 |
| Buccal and labial mucosa | 14 |
| Attached gingiva and taste buds | 10 |
| Junctional epithelium | 5 |
Table 3.4: Turnover time of the various regions of oral mucosa and skin
The time it takes to replace all of the cells within the epithelial layers of the skin and oral mucosa is shown in Table 3.4. As you should see, the oral epithelium grows quickly, which means it can regenerate quickly following injury. This is largely due to the presence of growth factors in saliva. This also means the lifespan of these cells is short, which means oral cancers are relatively rare in the absence of large doses of carcinogens (tobacco and alcohol). The epithelial cells of oral mucosa do not live long enough to easily acquire the multiple mutations to oncogenes and tumor-suppressor genes required to cause cancer.
Clinical applications of lining and masticatory mucosa histology
Hyper-keratosis
Hyper-keratosis is a homeostatic response of the oral mucosa to stress, either chemical or physical. In response to stress, epithelial cells express more keratin, causing an increase in the degree of keratinization. Vitamin A deficiency can lead to generalized hyper-keratosis.

Leukoplakia
If the increase in keratinization is localized, it is referred to as leukoplakia. Parafunctional habits can cause regions of the buccal mucosa to undergo hyper-keratosis. Bruxism may cause the linea alba to appear more white-ish. Chemical stress caused by use of smokeless tobacco products (snuff) cause leukoplakia at the site of use.

Nicotinic stomatitis
Hyper-keratosis can be caused by the chemical stress of cigarette smoke. It is not caused by nicotine, which is an addictive substance but mostly non-toxic, despite what many otherwise reliable resources suggest. We cover adverse effects of nicotine when we discuss PDL loss in chapter 11. For the oral mucosa, the chemical stress from smoking is caused by benzene, formaldehyde, poly-aromatic hydrocarbons, and other toxic chemicals produced by combustion (burning). At the time we are writing this, there is no evidence that nicotine gum causes hyper-keratosis of the oral mucosa, and the link between vaping and hyper-keratosis is not strong, despite both containing nicotine. If your patients smoke, these two nicotine-delivery methods are considerably safer for both the lungs and oral cavity, and can be helpful tools in smoking-cessation (nicotine is the addictive component of tobacco products). This is not to be mistaken for an endorsement of taking up an e-cigarette habit, nor maintaining one, we are discussing relative risk here.
Nicotinic stomatitis is a visible change to the hard palate. In response to chronic stress, the ortho-keratinized epithelium produces more keratin, leading to a more white-ish appearance. However, epithelial cells of the minor salivary glands do not respond to stress in this fashion, and remain pinkish (the genes for keratin production are possibly methylated and packed around histones in these cells). This same pattern can also be caused by ingesting hot liquids.
Clinical changes to the gingiva

Inflammation of any tissue is referred to as tissue-name-itis, hence gingivitis is inflammation of the gingiva, while periodontitis is inflammation to the gingiva and periodontium. The redness, swelling, heat and pain symptoms indicate the body has likely suffered trauma, and is undergoing a response to that trauma. Mucosa exude more liquid into an area as a part of the inflammatory process, known as edema, making that region of the oral mucosa larger and paler when inflamed. Edema may give gingiva a puffy or rolled appearance.
Ideally, an inflammatory response limits the spread of the initial damage and set the stage for regeneration. When a tissue regenerates, stem cells migrate into the affected area, divide, and differentiate into the cells needed to repair the damage, such as keratinocytes or fibroblasts.

Chronic inflammation, on the other hand, leads to cell death and the loss or recession of a tissue. This is because stem cells generally halt progression through the cell cycle until the inflammatory process removes the source of the stress. Without stem cells generating new cells, chronic stress allows everyday wear on a tissue to accumulate.

During an inflammatory response, the gingival sulcus fills with gingivo-crevicular fluid (GCF). GCF contains breakdown products of human cells undergoing necrosis or apoptosis, the breakdown products of bacteria being killed by white blood cells, bacterial toxins, and inflammatory molecules released by human cells. The dead-end of the gingival pocket minimizes mixing with the secretions of salivary glands, therefore taking a sample of gingival fluid is a diagnostic tool for measuring gingival health

Gingivitis
Gingivitis is any inflammation of the gums. It includes edema in the ECM of connective tissues in the lamina propria and sub-mucosa, as well as inside the epithelial cells of the oral mucosa. This causes the marginal, attached and inter-dental gingiva to become visibly swollen. When marginal gingiva is swollen, it may produce a crescent-shaped edema known as a McCall’s festoon. This inflammatory response generally causes no damage, but untreated gingivitis can progress to periodontitis, which in turn can lead to bone and tooth loss. Gingivitis also increases the risk of developing Alzheimer’s Disease and heart disease, making it all the more important to intervene as early as possible. Currently, half of American adults over the age of 30 suffer from periodontal disease, and seventy percent of people over the age of 65, there is plenty of room for more work to be done.

Gingival hyperplasia
Hyperplasia means the increased growth of a tissue, which could mean an increased number of cells, an increased amount of ECM produced by cells, or both. Gingival hyperplasia is an abnormal growth of gingival tissue. It may look similar to edema, but the underlying cause (and therefore treatment) is different. A tissue that has undergone hyperplasia is not as squishy as a tissue with edema. Hyperplasia is a side-effect of certain medications, such as phenytoin and cyclosporine. Other triggers exist, including pregnancy, hormonal disturbances, or it may even be a hereditary condition (Hereditary Gingival Fibromatosis). Like edema, gingival hyperplasia may be caused by poor oral hygiene. The first response of the immune system to oral microorganisms is inflammation (and therefore edema). Over time, the immune system may respond to continued stress by releasing growth factors that trigger increased cell division of nearby stem cells, and other signals (morphogens) that trigger cell differentiation and cellular activity (such as the production of ECM proteins). This is a perfectly healthy response to stress in the palms of the hands or soles of the feet, generating a callus. However, the body sometimes has trouble distinguishing between physical stress and other types of stress, such as chemical stress caused by toxins produced by microorganisms.

The increase in the size of the gingiva, even if not caused by poor oral hygiene, may make maintaining oral hygiene difficult, and should therefore be addressed. In some cases, it may not be possible to remove the underlying cause (such as a hereditary condition, or a life-saving anti-seizure medication), in which case surgical removal of gingival tissue (gingivectomy) or gingival reshaping (gingivoplasty) may be warranted. Excess gingival tissue can be removed using a scalpel or a laser tool. The use of lasers can reduce bleeding and pain by cauterizing damaged blood vessels and ablating nerve endings.

Pigmentation of the gingiva
Similar to increased levels of keratin in the attached gingiva, increased levels of melanin may obscure underlying healthy level of hemoglobin. The presence of melanin alone should not be mistaken for unhealthy gingiva. Unlike keratin, melanin is a pigment, meaning it absorbs only certain wavelengths of light (has a color). Surgeries and treatments to remove gingival pigment exist, often advertising what is found in textbooks: healthy gingiva should be pinkish or whitish in color (try a google search for gingival hyperpigmentation if you are skeptical). It is worth noting skin whitening products exist because systemic racism in the United States and other countries has led many people of color to feel displeasure with darker skin pigmentation, illustrated by experiments such as the Doll test by Drs Kenneth and Mamie Clark. Furthermore, the concept that pink is healthy and brown is unhealthy is not shared across cultures. For instance, dental offices in Ethiopia and surrounding areas may offer ethnobotanical tattooing of the maxillary gingiva to add a blue-ish or grey-ish coloration to the gingiva, masking pinkish regions.

A rapid, focal change in melanin production in the oral cavity may be a response to a medical condition. Most common among dark-skinned women between the ages of 30-50, increased melanin production in response to acute trauma or prolonged irritation (such as smoking) may arise, termed a melanocanthoma (further reading can be found here). Despite the name this type of skin lesion has, it is not a tumor, but a homeostatic change in cell activity. Tobacco smoke creates numerous free radicals that can be absorbed by epithelial cells, thus increased melanin production helps protect the oral mucosa. Tetracycline antibiotics bind to melanin, which triggers melanocytes to up-regulate melanin synthesis. Tetracycline drugs are very common, found in over-the-counter first-aid creams, added to animal feeds, and were even in beers brewed in Sudan 2,000 years ago.
There are other pigments that cause color changes to the gingiva, and they are classified as either endogenous (produced by human cells) or exogenous (environmental). Endogenous pigments commonly found in the gingiva, besides melanin, include hemoglobin and breakdown products of hemoglobin. A reddish lesion caused by hemoglobin or its breakdown products is a sign of damage to capillaries (bruising). An example of an exogenous pigment is jimsonweed (Datura stramonium), which can be used in the ethnobotanical gingival tattoos mentioned previously.

Figure 3.34: Gingival recession. Image credit: Class II gingival recession on the left maxillary canine and lateral incisor by Nitin Khuller, is licensed under CC BY 3.0
Gingival recession
Chronic inflammation of the gingiva can lead to gingival recession, exposing deeper tissues of the tooth, which in turn may make teeth more susceptible to tooth decay. The most common cause of gingival recession is gingivitis and periodontitis. Gingival recession can also be caused by abrasion (improper tooth brushing), abfraction (bruxism), improper tooth position, and aging.

A Stillman cleft is a V-shaped region of gingival recession. It is often caused by occlusal trauma.

Gingival grafting
A sub-epithelial connective tissue graft (SECT graft) may be performed to repair gingival recession. Unlike a skin graft, which grafts epithelial plus some or all of the connective tissue from a donor, a sub-epithelial graft transplants only connective tissue from the lamina propria and/or sub-mucosa. The goal of a sub-epithelial graft is not to replace damaged tissue, but to provide a scaffold that promotes healing of the patient’s own tissues. The connective tissue provides a scaffold which epithelial stem cells are attracted to and migrate over. These stem cells undergo mitosis, producing more epithelial cells which differentiate into keratinocytes and regenerate the oral epithelium. Similarly, the patient’s mesenchymal stem cells migrate through the scaffold and replace the transplanted collagen, regenerating the lamina propria and sub-mucosa.
 with transannular pericardial patch being sutured">
with transannular pericardial patch being sutured">
Sub-epithelial grafts splice connective tissue from nearby regions of healthy gingiva (such as from neighboring gingiva or hard palate). This leaves behind small wounds, which heal quickly. Nevertheless, damaging healthy tissue is not optimal. Another option is to use tissue from a human cadaver. Because the connective tissue used in such a procedure is mostly collagen fibers, options include the use of synthetic collagen-like polymers (Fig X) or a pericardial patch procedure. Unlike human tissue, there is a large supply of cow and pig connective tissue. First, the connective tissue that surrounds a cow or pig heart (the pericardium) is harvested and stripped of any pig or cow cells. The acellular tissue that remains should not trigger tissue rejection (collagen is collagen across vertebrates), but it acts as a scaffold. Ultimately, the patient’s own epithelial stem cells migrate over the scaffold to regenerate the oral mucosa. In addition, the patients mesenchymal stem cells migrate into the scaffold from nearby healthy sub-mucosa, and replace the cow or pig collagen. This procedure is very similar to different types of bone tissue grafts and is not limited in use to the gingiva—a video of a heart valve replacement using bovine pericardium can be viewed here We hope you appreciate the amount of histology and cell biology required to understand how pieces of cow hearts can be used to repair damaged gingiva.
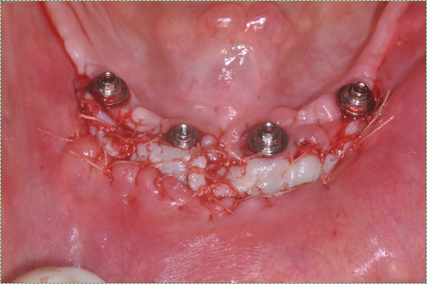
A free gingival graft may be done around dental implants, or used to repair gingival recession. Similar to the sub-epithelial graft, the free gingival graft harvests healthy tissue from the donor, only in this case epithelial cells from the oral mucosa are also transplanted. When placed around dental implants, attached gingival tissue can adhere to the implant, as opposed to junctional epithelium which adheres to a tooth. Coating a dental implant with Hyaluronic Acid helps grafted tissue adhere to the implant. Without adhesion to the implant, oral microorganisms can bypass the oral mucosa and enter the sub-mucosa. Similar to the sub-epithelial graft, connective tissue from a pig or cow can be used as a scaffold, removing the need for a second surgery site. Connective tissue grafts are relatively common in dentistry and maxillofacial surgery, but these technologies are starting to generate changes in tissue grafting below the neck, too.
| For further reading on dental biomaterials |
|---|
| FDA information on GINTUIT |
| Mucograft – acquired by Geistlich biomaterials |
| Gengigel Hyaluronic Acid gel |
Table 3.5: Further reading about currently available dental biomaterials
Clinical applications of dento-gingival junction histology

Periodontal pockets
The depth of a periodontal pocket can be measured using a calibrated probe. In a healthy state, the distance from the marginal gingiva to the epithelial attachment should be between 1-3mm. Pockets within this range typically have an intact epithelial attachment, which prevents oral bacteria from entering the sub-mucosa and causing gingivitis or periodontitis. Poor oral hygiene, however, can lead to increased levels of oral bacteria within the periodontal pockets. Because the junctional epithelium is more permeable than other regions of the oral mucosa, white blood cells come into contact with this bacterial population and trigger inflammation. With chronic inflammation comes a loss of junctional epithelium, which can reduce the thickness of the junctional epithelium further, potentially causing the loss of the epithelial attachment. At this point, the pocket is said to be lined with pocket epithelium. Since it is no longer attached to the tooth, the probe can likely be inserted over 3mm. The thinness of the pocket epithelium brings the probe closer to blood vessels in the lamina propria, making it more likely to damage these vessels, causing Bleeding on Probing (BoP, or Bleeding after Probing, BaP).
It is possible that a periodontal pocket deeper than 3mm can have junctional epithelium with an intact epithelial attachment. These exhibit minimal Bleeding on Probing, and can be considered uncharacteristically deep pockets rather than a clinical manifestation of periodontitis.

The major risk with Bleeding on Probing involves the oral microbiome, which is a large collection of microorganisms. These microorganisms come into contact with the bloodstream with disruption to the epithelial barrier. Even so-called “good bacteria” trigger inflammation when they move inside the body. Until damage to the barrier is repaired, inflammation continues. Chronic inflammation within the pockets leads to damage to nearby tissue, such as alveolar bone. This leads to further damage to the oral cavity which we discuss later. A second risk with migration of the epithelial attachment is that acid-producing bacteria now come into contact with softer cementum, leading to root caries.
Pseudopockets, which may also be called false pockets or gingival pockets, are caused by gingival hyperplasia or edema. Enlargement of the gingival margin, whether by mitosis or fluid buildup, deepens the measurement of a pocket, but does not share the same harmful loss of the epithelial attachment. The underlying cause of the pseudopocket may need to be addressed.
Clinical applications of specialized mucosa histology

Geographic tongue
Geographic tongue is a condition where filiform papillae on the dorsal surface of the tongue become non-uniformly hyper-keratinized, giving some filiform papillae a more white-ish appearance. Other papillae may be lost due to prolonged inflammation, leaving more reddish spots on the tongue. The pattern of keratinized versus partially-keratinized papillae changes over weeks. The result is almost always a cosmetic concern, although some patients may describe periods of heightened sensitivity to hot, acidic and/or spicy foods. There are currently no treatments for geographic tongue. The underlying causes of geographic tongue are unknown.

Black hairy tongue
Black hairy tongue occurs when filiform papillae shed epithelial cells more slowly, thus the papillae become enlarged. This allows the papillae to pick up more stains from tobacco smoke, foods, or oral bacteria, creating thicker, darker bumps on the tongue. It is thought that this condition might be triggered by overgrowth of certain oral fungi, possibly following the loss of competition with the use of certain antibiotics. The reason the filiform papillae appear hair-like is that both filiform papillae and hairs are composed predominantly of dead keratinized epithelial cells. Patients are encouraged to brush their tongue when brushing their teeth.
Chapter 2 * Chapter 4