
9.3: Atelectasis
- Page ID
- 14835

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)Case 1
Post-operative Atelectasis
Clinical:
History – This 50 year old female was two days post-operative from a colostomy. She presented with a fever, cough, and fatigue.
Symptoms – Mild cough.
Physical – The lungs were clear on auscultation. Poor inspiration was noted due to abdominal discomfort.
Laboratory – Her white blood cell count was mildy elevated.
DDx:
Atelectasis
Pneumonia
Imaging Recommendation
Chest X-ray
ODIN Link Linear Atelectasis, Figure 9.9: mistr.usask.ca/odin/?c seID=20160412203825261
Imaging Assessment
Findings:
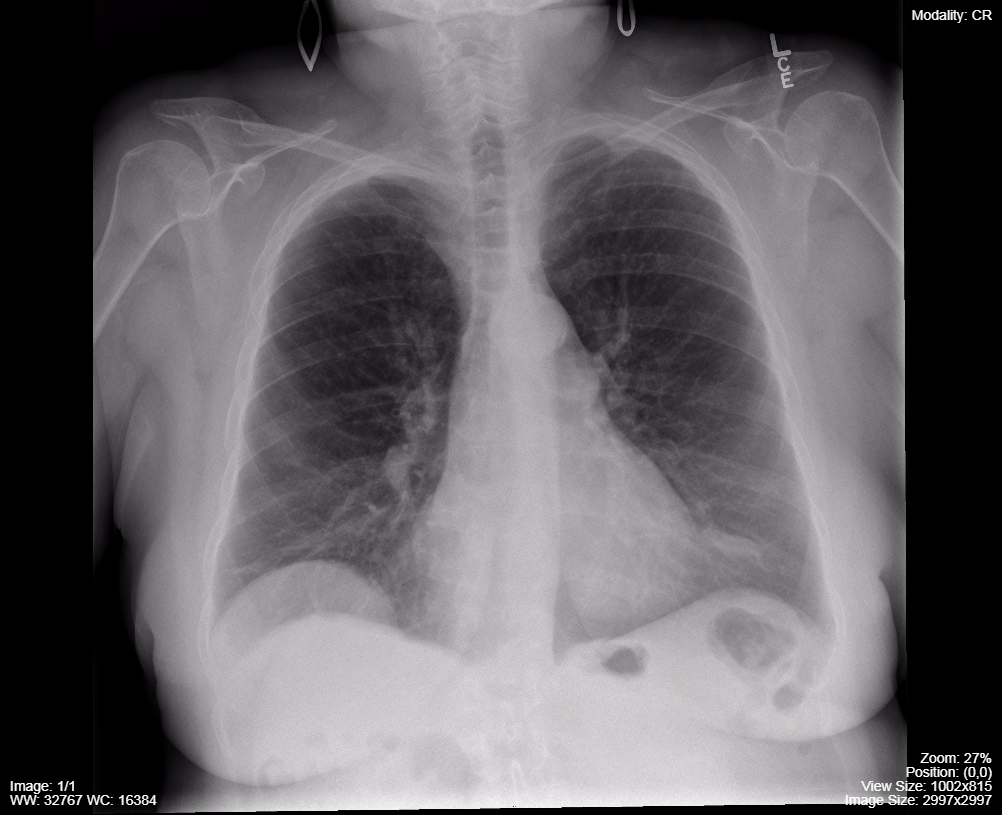
There were bands of linear opacity in both lower lungs. No evidence of any air bronchograms. Mild eventration of the right diaphragm was seen. No masses or adenopathy.
Interpretation:
Bilateral lung, linear atelectasis.
Diagnosis:
Plate or band-like atelectasis.
Discussion:
Definition of Atelectasis:
Atelectasis is diminished inflation of all, or part of, the lung. The synonym “collapse” is often used interchangeably with atelectasis, particularly when it is severe or accompanied by an obvious increase in lung opacity.
On x-rays and CT scans, reduced volume is seen, accompanied by increased opacity (chest radiograph) or attenuation (CT scan) in the affected part of the lung. Atelectasis is often associated with abnormal displacement of fissures, bronchi, vessels, diaphragm, heart, or mediastinum. The distribution can be subsegmental, segmental, or lobar. Subsegmental atelectasis is often qualified by descriptors such as linear, discoid, or platelike.
The different types of atelectasis are:
Passive – Another entity occupies the space usually occupied by lung, most often pleural fluid, but masses i.e. lung, or pleural, can enlarge and cause compression of the adjacent lung. Pneumothorax can also lead to passive atelectasis as the air in the pleural space causes the underlying lung to partially collapse.
Resorptive – An obstruction (intraluminal or extraluminal) prevents the normal ingress and egress of air. The gas in the aerated lung (bronchi, respiratory bronchioles, alveoli) downstream of the obstruction is resorbed/absorbed. This can be seen with endobronchial malignancies, mucous plugs in the bronchi, or extrinsic masses compressing airways leading to bronchial obstruction.
Also, inability to fully inflate the lungs i.e. splinting of the chest due to pain, and prolonged bed rest. may lead to linear bands of resorptive atelectasis.
Cicatrizing (/ˈsikəˌtrīz/) – Abnormal lung elasticity prevents the lung from expanding completely. This is often encountered after radiation therapy to the lung or as the result of a fibrosing infection such as tuberculosis.
X-ray findings may include:
- Atelectasis is often opaque lung associated with the diminished volume of air containing lung.
- Atelectasis can occur in a subsegmental (linear), segmental, or lobar distribution.
- The appearance of the diminished lung volume depends upon the type of atelectasis.
Case 2
Post Intubation Atelectasis
Clinical:
History – This 3 year old male presented with severe asthma and required endotracheal intubation.
Symptoms – None – intubated, sedated, and paralyzed.
Physical – No breath sounds in the left hemi-thorax or upper right lung.
Laboratory – Non-contributory.
DDx:
Atelectasis
Collapse
Pneumonia
Imaging Recommendation
Chest X-ray
ODIN Link Misplaced Endotracheal Tube and Atelectasis, Figure 9.10: mistr.usask.ca/odin/?caseID=20170114165716169
Imaging Assessment
Findings:
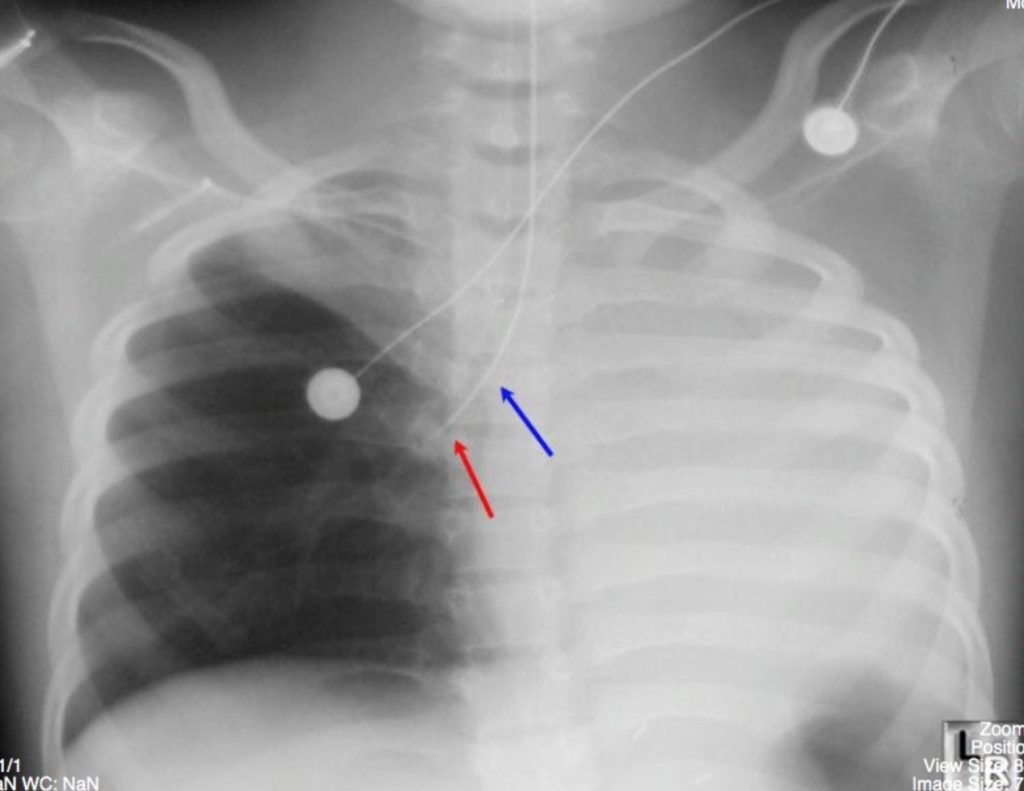
The left lung is totally opacified as is the right upper lobe. The endotracheal tube is in the right main bronchus quite distal in location. Note how the cardiac shadow was not seen in the right hemithorax as the central mediastinal structures have all shifted to the left due to the total atelectasis of the left lung.
Interpretation:
Total, resorptive, atelectasis with obstruction of the bronchi supplying both lobes of the left lung and the right upper lobe by the endotracheal tube.
Diagnosis:
Misplaced endotracheal tube leading to resorptive (obstructive) atelectasis.
Case 3
Pleural effusions, Passive atelectasis
Clinical:
History – This 42 year old male had severe gallstone pancreatits. He presented with severe shortness of breath and abdominal pain.
Symptoms – Severe shortness of breath with increased work of breathing and anxiety due to breathlessness.
Physical – Diminished breath sounds in both hemi-thoraces. Decreased volume in both lungs.
Laboratory – Non-contributory.
DDx:
Atelectasis
Collapse
Pneumonia
Pleural effusions
Imaging Recommendation
Chest X-ray
ODIN Link for Massive Pleural Effusions and Atelectasis (Chest x-ray and Ultrasound), Figure 9.11A and B: mistr.usask.ca/odin/?caseID=20170407235902470

Imaging
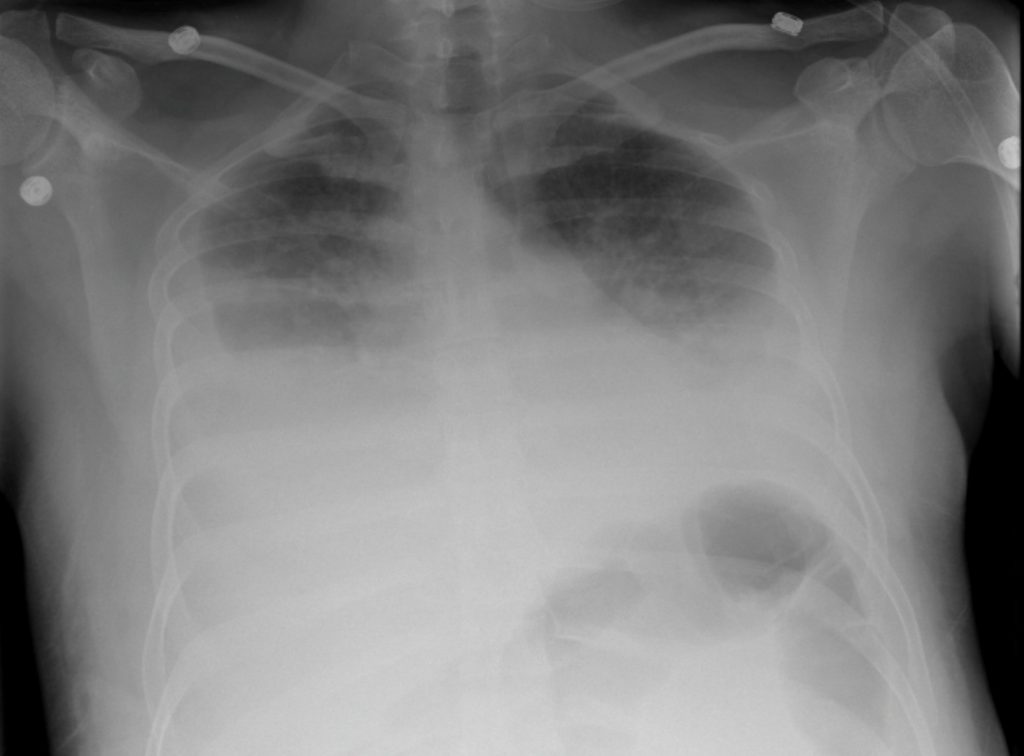
Findings CXR:
The volume of the aerated lungs is very diminished. There were large, bilateral pleural effusions.
Interpretation:
Basilar atelectasis due to large bilateral pleural effusions.
Findings US:
The basilar lung is an echogenic collapsed, triangular structure. The collapsed lung is basically suspended in the pleural fluid. There is a large, anechoic region surrounding the collapsed lung.
Diagnosis:
Passive atelectasis due to large, bilateral, pleural effusions.
Attributions
Figure 9.9 Post-Operative Atelectasis: Linear or Plate Like Atelectasis; Left Lower Lobe by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC–BY-NC-SA 4.0 license.
Figure 9.10 Resorptive Atelectasis. Endotracheal tube in right main bronchus. Totally atelectatic left lung and atelectasis of right upper lobe by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC–BY-NC-SA 4.0 license.
Figure 9.11A Passive Atelectasis. Massive Pleural Effusions by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC–BY-NC-SA 4.0 license.
Figure 9.11B Passive Atelectasis – Ultrasound, large pleural with atelectasis by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC–BY-NC-SA 4.0 license.