
9.6: Pneumonia
- Page ID
- 14838

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)ACR – Chest – Acute Respiratory Illness in Immunocompetent Patient
Case 1
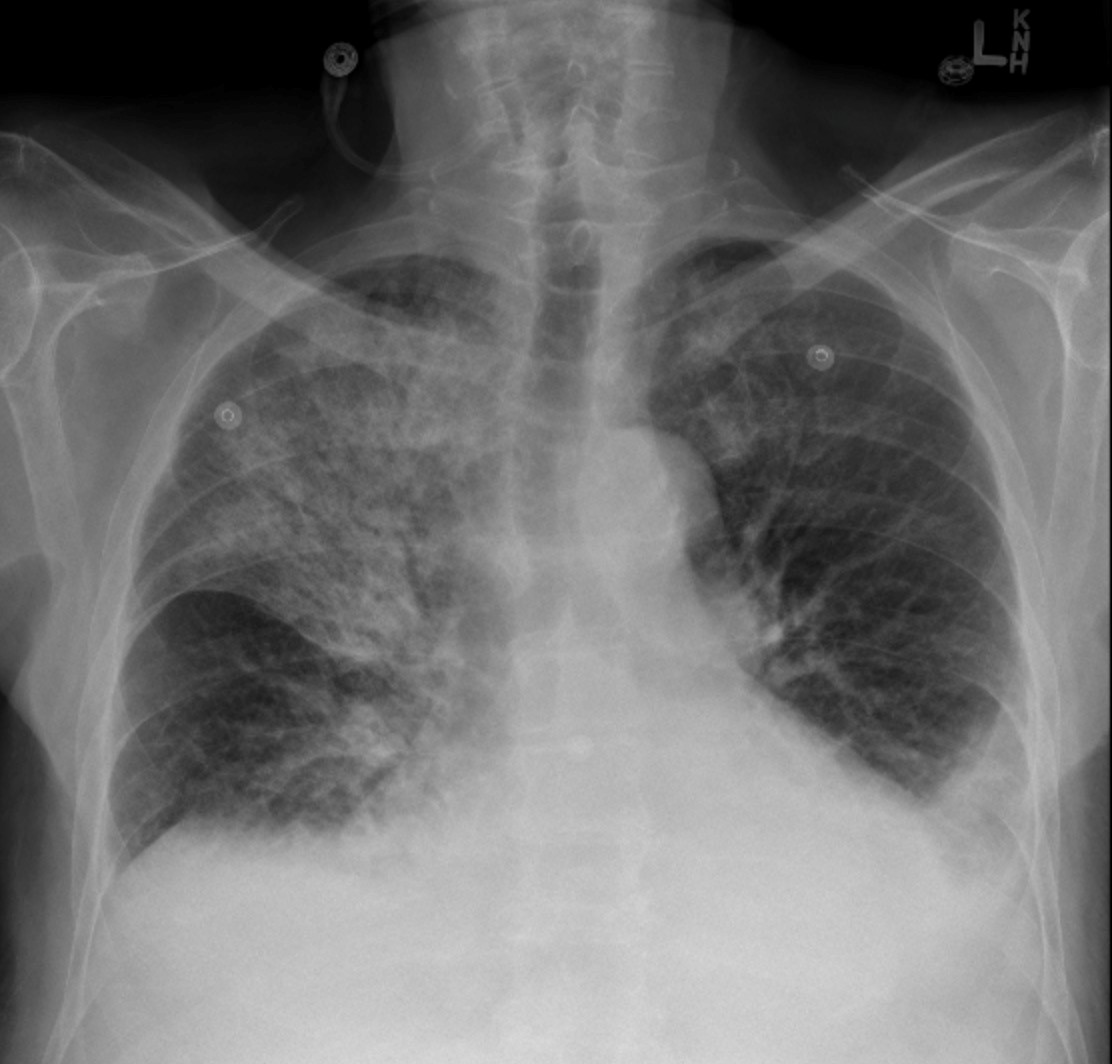
Right Upper Lobe and Left Lower Lobe Consolidation with Air Bronchograms
Clinical:
History – This 50 year old male had just returned from a trip to Cuba. He presented with a fever, fatigue, and a cough productive of green sputum.
Symptoms – Progressively worsening cough associated with a fever of 39C. He was producing green sputum. He also complained of a mildly sore throat.
Physical – Coarse rales were heard in the right upper chest and the left lower chest. Transmitted breath sounds were also heard in these regions. His tonsils and pharynx were reddened with white exudate seen on the tonsilar fossae.
Laboratory – His white blood cell count was elevated.
DDx:
Pharyngitis
Pneumonia
Bronchitis
Imaging Recommendation
ACR – Chest – Acute Respiratory Illness in Immunocompetent Patient, Variant 4
Chest X-ray
ODIN Link for Pneumonia images, Figure 9.17A and B: mistr.usask.ca/odin/?caseID=20170221151826268
Imaging Assessment
Findings:
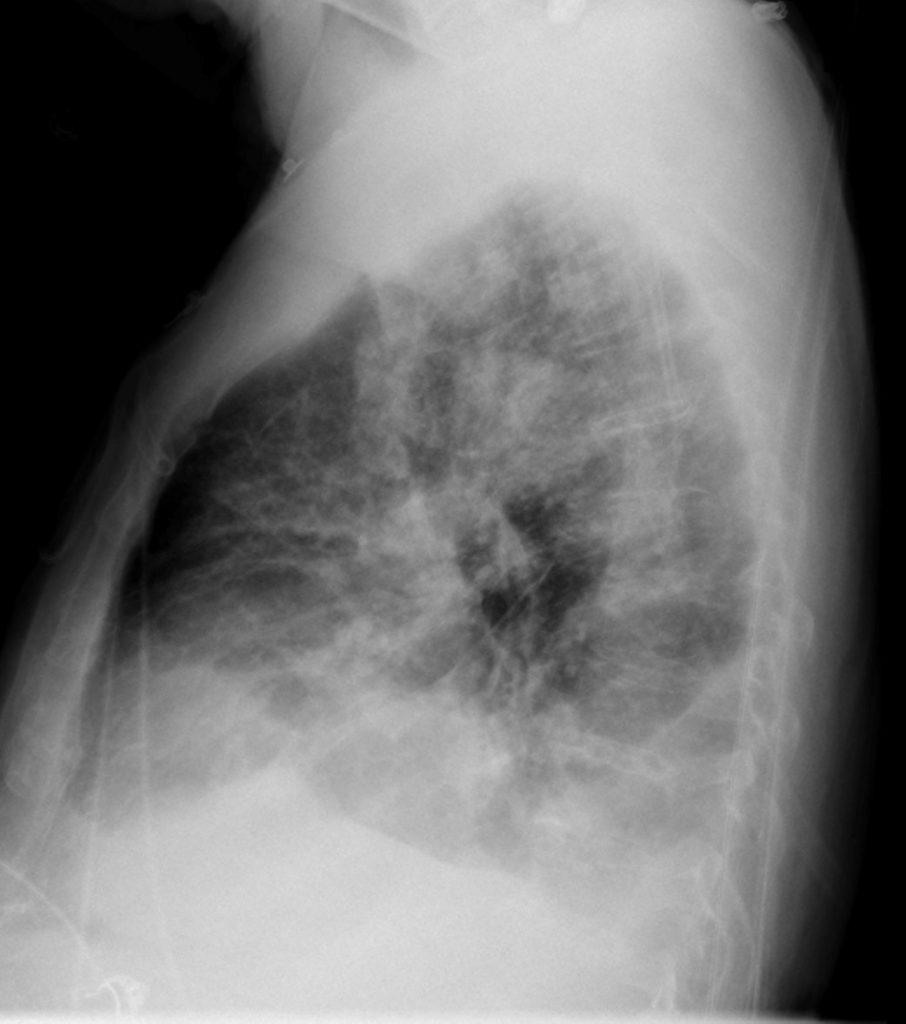
There were small, bilateral pleural effusions. The right upper lobe and the left lower lobe were densely consolidated with air bronchograms seen in these regions. There was patchy airspace consolidation throughout the lungs. No masses or adenopathy.
Interpretation:
Bilateral lung consolidation associated with small bilateral effusions. If the clinical presentation includes fever, this is most likely pneumonia.
Diagnosis:
Right Upper Lobe and Left Lower Lobe Consolidation with Air Bronchograms – Community Acquired Pneumonia
Discussion:
Generalized opacity of the lung, with preserved volume of the lung, is called consolidation. Consolidation can be caused by fluid (transudate, exudate), blood, protein, and cells. In the clinical setting of associated fever and abnormalities of the white blood cell count, the pattern would fit best with infective consolidation (pneumonia, exudate).
Pneumonia can be defined as consolidation of the lung produced by inflammatory exudate, usually as a result of an infectious agent. Most pneumonias produce airspace disease, either lobar or segmental. Other pneumonias demonstrate interstitial disease and others produce findings in both the airspaces and the interstitium. Most microorganisms that produce pneumonia are spread to the lungs via the tracheobronchial tree, either through inhalation or aspiration of the organisms.
An air-bronchogram is the presence of a tubular, air filled, bronchus that does not contain exudate. The margins of the consolidated lung are irregular as alveoli are recruited by passage of exudate from one to the other via the pores of Kohn, resulting in an ill defined edge to the consolidation. Fissures block the spread of consolidation and there is a straight edge demarcating consolidation abutting a fissure.
X-ray findings may include:
- Opaque segment or lobe (consolidation).
- The margins of the opacity may have a fluffy boundary due to spread through the alveolar sacs via the pores of Kohn.
- The consolidation does not cross any fissures.
- The volume of the opaque lung is preserved.
- Air bronchograms may be present.
Case 2
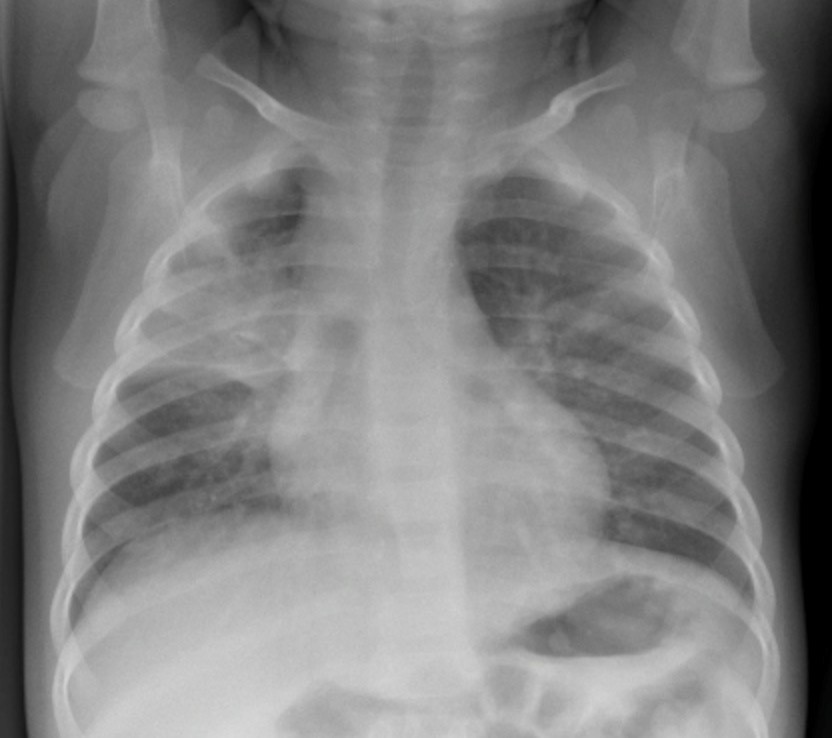
Pediatric Right Upper Lobe Consolidation
Abuts Major Fissure
Clinical:
History – This 5 year old male was lethargic and looked unwell. He presented with a fever, cough productive of green sputum, and fatigue.
Symptoms – Progressively worsening cough associated with a fever of 39C. He was producing green sputum. He also complained of a mildly sore throat.
Physical – Coarse rales were heard in the right upper chest and the left lower chest. Transmitted breath sounds were also heard in these regions. His tonsils and pharynx were reddened with white exudate seen on the tonsilar fossae. His tympanic membranes were normal.
Laboratory – His white blood cell count was elevated.
Imaging Recommendation
ACR – Chest – Acute Respiratory Illness in Immunocompetent Patient, Variant 4
Chest X-ray
ODIN Link Rounded Pneumonia images, Figure 9.18A and B: mistr.usask.ca/odin/?caseID=20150702231205343

Imaging Assessment
Findings:
There was no evidence of pleural effusion. The right upper lobe was consolidated with air bronchograms seen in this region. The edges of the lung opacity do have rounded contours at several locations. There was patchy airspace consolidation throughout the lungs. No masses or adenopathy.
Interpretation:
Right lung consolidation. If the clinical presentation includes fever, this is most likely pneumonia. The smooth contour of area of consolidation is typical for ’rounded pneumonia’ most often seen in children.
Diagnosis:
Right Upper Lobe Consolidation, Rounded Pneumonia, with Air Bronchograms – Community Acquired Pneumonia
Rounded Pneumonia
This is a subtype of pneumonia that occurs in children between 2 and 10 years of age. The pores of Kohn and the communications between bronchioles are less mature in children and this prevents the spread of exudate via these pathways. Hence, the margins of the pneumonia in this subtype are smoother and more distinct resulting in a rounded edge contour of the consolidation.
Attributions
Figure 9.17A AP Chest x-ray, Pneumonia by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC–BY-NC-SA 4.0 license.
Figure 9.17B Lateral Chest x-ray, Pneumonia by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC–BY-NC-SA 4.0 license.
Figure 9.18A Pediatric Chest x-ray. Rounded Pneumonia by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC–BY-NC-SA 4.0 license.
Figure 9.18B Lateral Pediatric Chest x-ray. Rounded Pneumonia by Dr. Brent Burbridge MD, FRCPC, University Medical Imaging Consultants, College of Medicine, University of Saskatchewan is used under a CC–BY-NC-SA 4.0 license.