
3.6: Pediatric Nasopharyngeal Airway (NPA)
- Page ID
- 15445

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
PEDIATRIC NASOPHARYNGEAL AIRWAYS (PNA)
Andrés Alvo, Cecilia Sedano, Graeme van der Meer
A nasopharyngeal airway (NPA) is an airway adjunct consisting of a hollow plastic tube designed to stent the nose and nasopharynx. Depending on the level of the obstruction the NPA will terminate in the nasopharynx, oropharynx or hypopharynx. It is better tolerated than an oropharyngeal (Guedel) airway and has the advantage that it can be used in patients with an intact gag reflex, trismus and oral trauma.
| Level of obstruction | Etiology |
| Nose |
Pyriform aperture stenosis Choanal atresia |
| Nasopharynx |
Adenoid hypertrophy Underdeveloped midface (Crouzon’s, Apert’s, Pfeifer’s syndromes) |
| Oropharynx |
Tonsil hypertrophy Tumours Macroglossia |
| Hypopharynx |
Micrognathia (Pierre Robin Syndrome) Lingual tonsil hypertrophy Glossoptosis |
Table 1: NPAs can be used to alleviate obstruction at any level from the anterior nasal cavity to the hypopharynx
Although NPAs have been mainly used in emergency and anesthetic medicine, they are being increasingly used in pediatric otolaryngology. NPAs can be used to alleviate obstruction at any level from the anterior nasal cavity to the oropharynx (Table 1). They are often used to maintain airway patency in patients with a high risk of developing postoperative respiratory complications after adenotonsillectomy.
Relative and absolute contraindications to NPA insertion include severe stenosis or atresia of the nasal cavities, facial fractures, recent surgery of the skull base, active sinonasal infection, active epistaxis, and uncorrected coagulopathies or anticoagulant use.
| Age | NPA size | Suction catheter size |
| Preterm - 1 mo | 3 | 6 |
| 1-6 mo | 3.5 | 8 |
| 6-18 mo | 4 | 8 |
| 18 mo - 3 yrs | 4.5 | 8 |
| 3-6 yrs | 5 | 10 |
| 6-9 yrs | 5.5 | 10 |
| 9-12 yrs | 6 | 12 |
| 12-14 yrs | 6.5 | 14 |
Table 2: NPA size as determined by patient’s age

Figure 1: Commercially available NPAs come in different sizes
Commercially available NPAs come in different sizes and materials (Figure 1). The size is determined by the patient’s age. (Table 2). They can also be fashioned from endotracheal tubes (ETT) which are readily available, also in resource constrained settings.

Figure 2: Materials needed to create an NPA from an ETT. a) Portex® tube holder (half-size smaller than the ETT); b) Portex® Blue Line® ETT (ID 0.5 to 1 mm smaller than age-appropriate size, or similar to the diameter of the patient’s little finger)
This chapter describes how to manufacture an NPA using an ETT, how to insert and fix it to a patient (Figure 2), and its aftercare.
Making an NPA from an Endotracheal Tube (ETT)
- Figure 2 illustrates materials needed to create an NPA from an ETT

Figure 3: Murphy eye /additional air vent (arrow)
- A soft, uncuffed ETT (Portex® Blue Line®)) is preferred, ideally without Murphy eye (Figure 3)
- The inner diameter (ID) should be 0.5 to 1 mm smaller than the age appropriate ETT size
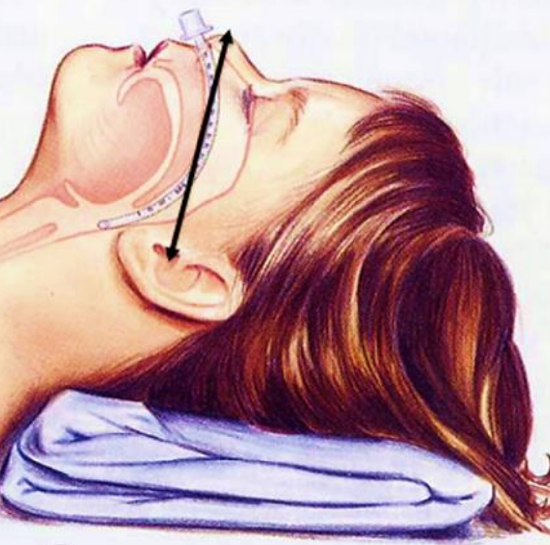
Figure 4: Determine the starting length of the NPA by measuring the distance from the nasal tip to the tragus
- Determine the starting length of the NPA by measuring the distance from the nasal tip to the tragus, adding a few centimeters to allow for adjustments should it be required (Figure 4)
- For custom-made NPAs the length is dictated by the level of obstruction that needs to be bypassed
- Cut the ETT to the desired length at its proximal (unbevelled) end
- The bevel of the NPA should face medially, away from the lateral pharyngeal wall to avoid soft tissue of the pharynx blocking the end of the tube. The bevel faces medially by default when the right nasal passage is used
- If the NPA needs to be passed on the left side, a new bevel must first be created by cutting the distal end of the tube obliquely, taking care not to leave any sharp edges
- Once the correct length has been determined, mark the proximal end flush with the nasal rim, and cut the ETT at this point
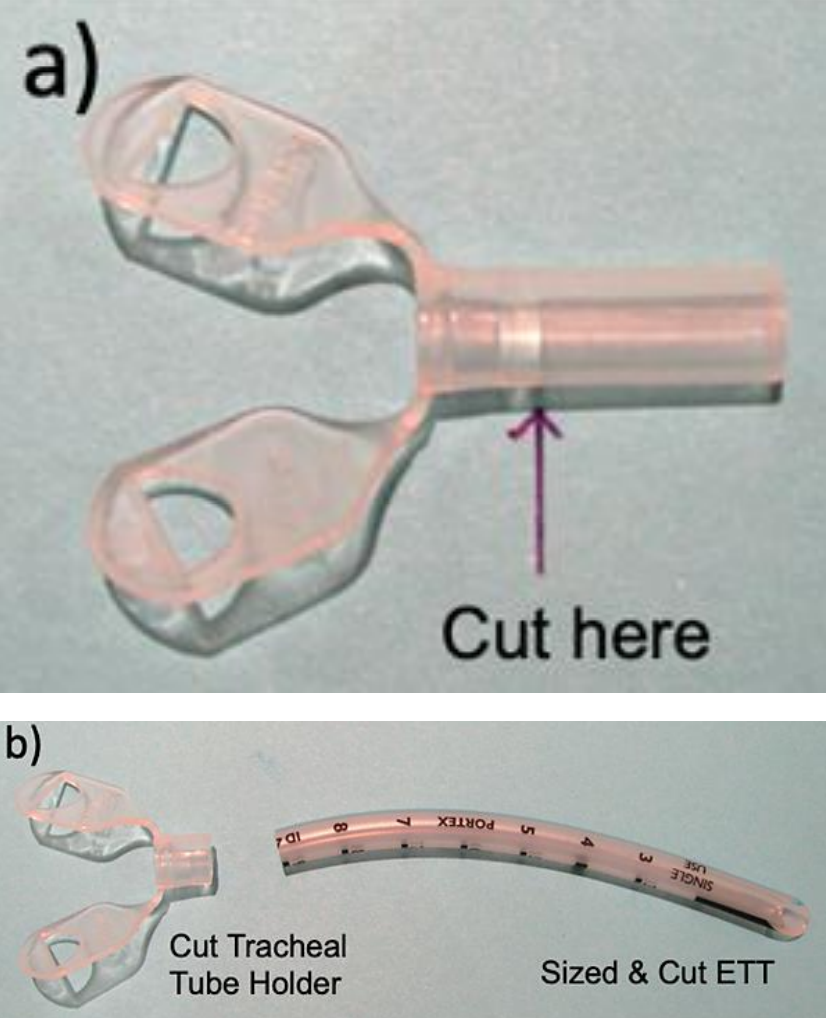
Figures 5a, b: Cutting tube holder and ETT
- A half-size smaller Portex® tube holder is cut distal to its flanges (Figures 5a,b)

Figure 6: Suturing the tube holder to the ETT; Prolene® 4-0 suture is being used and the knot is tucked inside the lumen
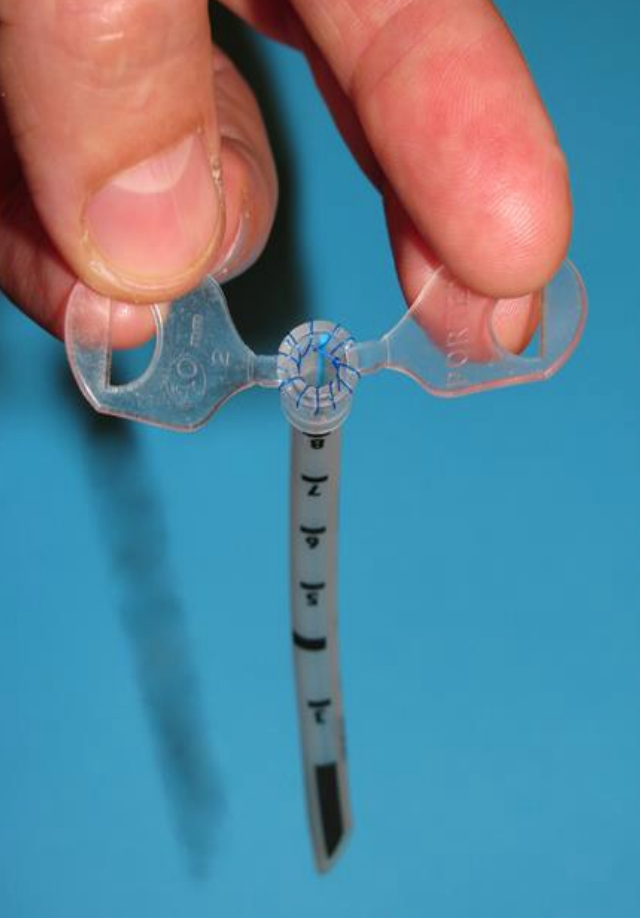
Figure 7: Completed NPA
- Suture the tube holder to the ETT using a Prolene® or nylon 4-0 suture (Figures 6, 7)
- Recheck and note the length and reinsert the NPA

Figure 8: NPA in situ and taped to the face
- Secure the flanges to the sides of the child’s face with tape (Figure 8)

Figure 9: If tube holders are unavailable, one can leave the proximal end of the ETT longer and split it down its length to create two flaps that are taped to the face
- If tube holders are unavailable, the proximal end of the ETT longer can be split lengthwise to create two flanges that can be secured to the face (Figure 9)

Figure 10: Commercial pre-made NPAs can be secured by passing sutures through the proximal “button” which are then taped to the face
- Note: If commercial NPAs are used, the length is standard for every ID size (but can be trimmed if necessary). The proximal “button” end can be secured by passing sutures which are then taped to the face (Figure 10)
Inserting an NPA
- Topical nasal decongestant drops may be applied
- Bend the NPA into a downward curve with the bevel facing medially
- Lubricate the NPA with saline or a lubricant
- Insert it into the nose and direct it along the floor of the nose
- Avoid excessive force, though gentle twisting can assist its passage into the nasopharynx
- If inserted in the operating room, direct inspection of the pharynx should show the tube projecting 1 cm below the free edge of the soft palate
- Alternatively, a flexible nasendoscope can be passed through the tube to measure exactly where the tip of the NPA should be located
- In some cases, such as with retrolingual collapse, the tip of the NPA can be positioned more distally above the epiglottis, if tolerated by the patient
Additional modifications
A standard 15 mm adapter can be used with an NPA customized from an ETT, for connection to mechanical ventilation. Some have adapted commercial NPAs for this purpose.
Caring of NPAs
Maintaining patency: NPAs should be suctioned as required to prevent blockage. The suction catheter should not be inserted more than 0.5 cm beyond the distal end of the NPA. Instillation of saline drops helps to soften secretions and facilitates toilet. Patency can be grossly checked by a mirror fogging / misting test. If an NPA becomes obstructed and cannot be unblocked with suction, the tube is removed and replaced, especially if the patient becomes distressed. Parents should always keep spare NPAs of the same and smaller sizes.
Fixing NPA: Tapes should be checked regularly to avoid accidental displacement of the NPA. The skin around the nostrils and cheeks must be regularly checked and cleaned to avoid infection and pressure ulcers.
Changing NPA: Routine changes of the NPA depends on the amount of secretions, but usually ranges between every 1-4 weeks. Initial insertion and the 1st NPA change should be performed by a member of the otolaryngology team. If insertion is easy, subsequent changes can be performed by trained staff or family members. Family should be advised that if NPA reinsertion becomes difficult, but the patient is stable, no further attempts should be made until an experienced health professional has been consulted.
Cleaning: NPAs can be washed with soap and water, or discarded and replaced, depending on available resources.
Mucosal granulations can develop at the distal end of the NPA. This should be suspected if partial distal blockage is encountered, especially if bleeding is observed. A flexible nasendoscope can be passed through larger NPAs for visual inspection. Management may include vasoconstrictor and steroid drops, shortening the tube or switching it to the contralateral side.
Homecare: When NPAs are used long term, parents and caregivers must be properly trained and have access to the necessary equipment such as a portable suction unit, and materials including suction catheters, spare NPAs, saline, lubricants, gauze, and tapes prior to discharge from hospital.
Acknowledgements
Dr Nikki Mills, RN Debby Sandow and SLT Melissa Keesing for providing supporting material
Authors
Andrés Alvo
Otorhinolaryngologist
Hospital Roberto del Río
Hospital Clínico Universidad de Chile
Clínica Alemana de Santiago
Santiago, Chile
andresalvo@gmail.com
Cecilia Sedano
Otorhinolaryngologist
Hospital Roberto del Río
Hospital San José
Santiago, Chile
cecisedano@gmail.com
Graeme van der Meer MBChB, MMed
Otorhinolaryngologist
Starship Children's Hospital
Auckland, New Zealand
GraemeV@adhb.govt.nz
Pediatric Section Editor
Nico Jonas MBChB, FCORL, MMed
Pediatric Otolaryngologist
Addenbrooke’s Hospital
Cambridge, United Kingdom
nico.jonas@gmail.com
Editor
Johan Fagan MBChB, FCS (ORL), MMed
Professor and Chairman
Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za