
5.4: Requirements for Ventilation
- Page ID
- 83998
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)The major features necessary for proper ventilation include (1) open airways for easy air movement, (2) defense mechanisms that assure that only clean, moist, warm air reaches the lungs, (3) proper pressure changes in the thoracic cavity and lungs to make the air move, (4) compliance in thoracic and lung components so that pressure changes cause them to expand easily to accept incoming air, and (5) control systems that ensure that the process occurs successfully and at the correct rate.
Contributions by Airways
The contributions made by muscles and skeletal components to the first four of these requirements were described previously. We will now consider the ways by which the airways contribute to these requirements.
Nasal Cavities
Inspired air entering the nostrils passes through the nasal cavities above the hard palate. These cavities are held open by the bones of the skull. As air passes through the nasal cavities, it is cleaned, moistened, warmed, and monitored so that it does not harm the delicate structures deep within the lungs (Figure 5.5).

The air is cleaned because dust and other particles are trapped by hairs inside the nostrils and by the sticky mucus that coats the inside of the cavities. Microscopic hairlike cilia on the cells lining the cavities wave back and forth, causing the mucus to glide back toward the throat. Then the mucus and its trapped debris can be harmlessly swallowed.
The air is moistened by the mucus to prevent drying of the lungs. Heat from the blood in the walls of airways warms the air so that the lungs are not chilled. Finally, sensory nerve cells monitor the chemical contents of the air and send impulses to the brain. The presence of such chemicals is perceived as aromas. The nervous system may cause inspiration to slow or stop if harmful chemicals or particles are detected. Forced expiration (e.g., sneezing) may be initiated in an attempt to blow the noxious materials out of the respiratory system.
A person may inspire some or all of the air he or she breathes through the mouth rather than through the nasal passages. This can increase the rate of airflow, but it reduces the amount of cleaning, moistening, and warming of inspired air. Injury to the airways below the pharynx may result. Inspiring through the mouth can also lead to excessive dryness of the oral cavity, which may cause oral discomfort and sores.
Nasopharynx
Air in the nasal cavities moves backward into the nasopharynx, which is above the soft palate. Bones and other firm tissues keep this passage open except when one is swallowing, during which the tongue pushes upward on the soft palate. The mucus, cilia, and blood in the nasopharynx further clean, moisten, and warm the air.
Pharynx
After passing through the nasopharynx, the air moves through the throat, or pharynx, into the opening in the voice box, or larynx. This opening is called the glottis. The pharynx is held open by the firmness of the muscles and other tissues that make up its walls.
Since food and beverages in the oral cavity that are being swallowed also pass through the pharynx, these materials can lodge in the pharynx or enter the glottis, blocking or injuring the airways. Two reflexes controlled by the nervous system prevent these problems.
The swallowing reflex occurs whenever solids or liquids are present in the pharynx behind the tongue (Figure 5.6). This reflex clears the pharynx by pushing materials down into the esophagus. At the same time, a flap called the epiglottis is moved over the glottis to prevent materials from entering the larynx. The epiglottis is moved off the glottis after swallowing has been completed so that ventilation can begin again.
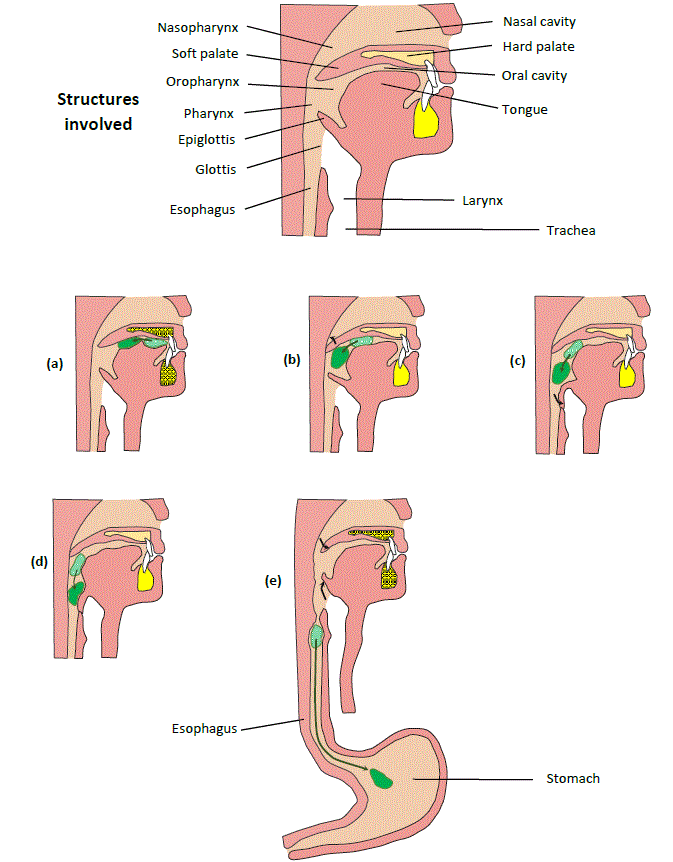
(a) the tongue pushes food back in oral cavity (voluntary); (b) as food moves under the soft palate, throat muscles cause the soft palate to elevate, closing the nasal air passageway (reflex); (c) as muscle contractions push food through the pharynx, muscle contractions of the pharynx and larynx cause the epiglottis to fold down over the glottis, closing glottis (reflex); (d) throat muscle contractions push food over the epiglottis and into the esophagus; (e) wave of contraction down the esophagus pushes food down and into the stomach. Soft palate and epiglottis return to original positions to allow breathing again. (Copyright 2020: Augustine G. DiGiovanna, Ph.D., Salisbury University, Maryland. Used with permission.)
The gag reflex is caused when irritating materials enter the pharynx. This reflex causes muscles near the pharynx to close the openings into the larynx and esophagus. At the same time, muscle contractions in the abdomen raise the pressure in the esophagus and trachea to prevent materials from entering those passageways. A very strong gag reflex can result in vomiting.
Larynx, Trachea, and Primary Bronchi
Air passing through the glottis moves through the larynx, down the windpipe (trachea), and through the two primary bronchi into the lower airways in the lungs. Plates and rings of springy cartilage within the walls of these airways provide support so that the airways stay open during ventilation.
Materials other than air that enter these air passages initiate the cough reflex. During coughing, bursts of air that are expired rapidly force foreign materials up and out of these airways.
The mucus, the cilia, and blood flow in these structures carry out further cleaning, moistening, and warming of the air. The cilia beat in an upward direction so that the mucus glides into the pharynx. Since the mucus carrying materials slides upward in a smooth continuous stream, this mechanism is called the mucociliary escalator. Phagocytic macrophages and immune system cells in the trachea and primary bronchi provide additional defense against foreign materials.
Smaller Bronchi, Bronchioles, and Alveolar Ducts
As each primary bronchus enters a lung, it branches repeatedly, forming ever more numerous smaller bronchi and bronchioles and finally microscopic alveolar ducts.
The walls of these airways become thinner as they branch and narrow. Cartilage in the smaller bronchi keeps them open during inspiration. There is no cartilage in the bronchioles or smaller airways. A peculiar helical structure of the collagen that coils around the airways and elastin fibers also support these smaller airways. The cartilage and fibers provide the lungs with compliance. Like the trachea and bronchi, these smaller airways are protected by the cough reflex and defense cells, and they condition the entering air.
Smooth muscle cells in the airway walls allow for appropriate adjustments in their diameter as the amount of ventilation needed fluctuates. The smaller airways provide most of this adaptability. The activity of the muscle is controlled by the nervous system, the endocrine system, and nearby chemicals.
As air is expired and the lungs decrease in size, the open passages in the airways become narrower. The walls of the smallest airways are so thin and weak that these airways close completely before all the air has escaped from the alveoli below them. This air remaining in the alveoli makes up part of the residual volume.
Alveolar Sacs and Alveoli
The inspired air in the alveolar ducts passes into blind cup‑shaped outpocketings called alveoli. Most alveoli occur in clusters extending outward from slightly enlarged spaces at the ends of the alveolar ducts, called alveolar sacs. Each cluster may look like a tightly packed bunch of plump grapes (Figure 5.7a and Figure 5.7b).

There are about 300 million alveoli in the lungs. Because alveoli are hollow, filled with air, and very small, and because they make up most of the lungs, dried lungs have the consistency of Styrofoam. The alveoli provide an amount of surface area equivalent to that of an area 30 feet long and 25 feet wide. The walls of the alveoli are very thin, allowing diffusion of O2 and CO2 between the air and the blood to occur easily.
Special cells in the alveoli secrete a material called surfactant. As surfactant spreads out, it coats the inner surface of the alveoli and parts of the smaller airways. The surfactant greatly increases the compliance of the lungs by reducing the attraction between the water molecules on the inner surfaces of the lungs. Without surfactant, the attraction (surface tension) would be so great that the alveoli and small airways would collapse. The inner surfaces would stick together tightly, making it nearly impossible for them to separate and fill with air during inspiration. These characteristics can be compared to the difference between the effort needed to inflate a new balloon or to put a hand into a new rubber glove that contains a powdery surfactant, and the effort needed to inflate an old balloon or to put a hand into an old rubber glove that dried after becoming damp.
Surface tension is important because as it makes the lungs collapse, it helps increase the pressure in the lungs, and therefore assists in expiration. The combination of a moderate amount of surface tension in the alveoli and the large surface area they provide makes expiration much easier.
Control Systems
Nervous System
Ventilation begins with inspiration, which requires the contraction of muscles. The nervous system signals activating these muscles originate in a region of the brain called the medulla oblongata and travel to the muscles through nerves. The medulla oblongata is inside the region of the skull just above the neck (Figure 6.8). The part of it concerned with respiration is called the respiratory control center.
The respiratory control center starts inspiration when it detects an increase in CO2 levels or a decrease in O2 levels in the blood flowing through it. When sensory nerve cells from the aorta and arteries in the neck detect very high levels of CO2 or very low levels of O2, these nerve cells also stimulate the respiratory control center. Other sensory neurons in the lungs send impulses to the respiratory control center, telling it that the lungs are in a partially collapsed condition and are ready for inspiration. Sensory nerves from muscles and joints inform the respiratory center when a person begins physical activity and will need more gas exchange.
Nerves from the lungs inform the respiratory center and a nearby part of the brain called the pons when inspiration is complete. The brain then stops the impulses for inspiration. As the muscles relax, expiration begins because of elastic recoil of the thorax and lungs. The respiratory center can also send impulses to the muscles indicating that a forceful expiration is needed.
The respiratory center and the pons monitor their own impulses and are also informed by nerves from the lungs when expiration is complete. This triggers the beginning of the next inspiration. Therefore, the linking and repeating of two negative feedback systems result in rhythmic breathing.
The depth of breathing, the speed of airflow, and the respiratory rate are adjusted when the respiratory center detects that CO2 concentrations, O2 concentrations, or the acid/base balance in the blood are beginning to wander from proper levels. The adjustments restore appropriate gas levels and acid/base balance so that homeostasis is maintained.
Ventilation is also modified by the swallowing, gag, and cough reflexes. In addition, upper regions of the brain such as the areas controlling emotions and those controlling conscious actions can influence the respiratory center. The conscious control areas allow voluntary modifications of ventilation including inspiration, expiration, stopping ventilation, and modifying ventilation for actions such as talking.
The nervous system also controls ventilation by adjusting the size of the lower airways. Impulses from the sympathetic nervous system cause relaxation of smooth muscles in the airways, permitting them to dilate and increasing minute volume. Parasympathetic nerves cause the smooth muscles to contract, constricting the airways and reducing minute volume. These changes allow the rate of gas exchange to maintain homeostasis for O2 and CO2.