
3.7: Pharmacological treatment
- Page ID
- 42739

\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
\( \newcommand{\dsum}{\displaystyle\sum\limits} \)
\( \newcommand{\dint}{\displaystyle\int\limits} \)
\( \newcommand{\dlim}{\displaystyle\lim\limits} \)
\( \newcommand{\id}{\mathrm{id}}\) \( \newcommand{\Span}{\mathrm{span}}\)
( \newcommand{\kernel}{\mathrm{null}\,}\) \( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\) \( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\) \( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\id}{\mathrm{id}}\)
\( \newcommand{\Span}{\mathrm{span}}\)
\( \newcommand{\kernel}{\mathrm{null}\,}\)
\( \newcommand{\range}{\mathrm{range}\,}\)
\( \newcommand{\RealPart}{\mathrm{Re}}\)
\( \newcommand{\ImaginaryPart}{\mathrm{Im}}\)
\( \newcommand{\Argument}{\mathrm{Arg}}\)
\( \newcommand{\norm}[1]{\| #1 \|}\)
\( \newcommand{\inner}[2]{\langle #1, #2 \rangle}\)
\( \newcommand{\Span}{\mathrm{span}}\) \( \newcommand{\AA}{\unicode[.8,0]{x212B}}\)
\( \newcommand{\vectorA}[1]{\vec{#1}} % arrow\)
\( \newcommand{\vectorAt}[1]{\vec{\text{#1}}} % arrow\)
\( \newcommand{\vectorB}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\( \newcommand{\vectorC}[1]{\textbf{#1}} \)
\( \newcommand{\vectorD}[1]{\overrightarrow{#1}} \)
\( \newcommand{\vectorDt}[1]{\overrightarrow{\text{#1}}} \)
\( \newcommand{\vectE}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash{\mathbf {#1}}}} \)
\( \newcommand{\vecs}[1]{\overset { \scriptstyle \rightharpoonup} {\mathbf{#1}} } \)
\(\newcommand{\longvect}{\overrightarrow}\)
\( \newcommand{\vecd}[1]{\overset{-\!-\!\rightharpoonup}{\vphantom{a}\smash {#1}}} \)
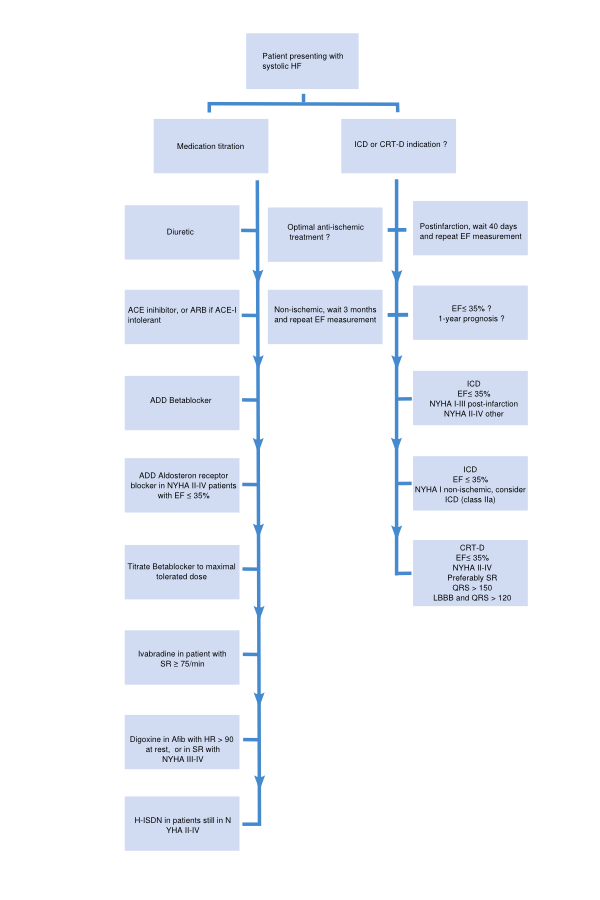
\(\newcommand{\avec}{\mathbf a}\) \(\newcommand{\bvec}{\mathbf b}\) \(\newcommand{\cvec}{\mathbf c}\) \(\newcommand{\dvec}{\mathbf d}\) \(\newcommand{\dtil}{\widetilde{\mathbf d}}\) \(\newcommand{\evec}{\mathbf e}\) \(\newcommand{\fvec}{\mathbf f}\) \(\newcommand{\nvec}{\mathbf n}\) \(\newcommand{\pvec}{\mathbf p}\) \(\newcommand{\qvec}{\mathbf q}\) \(\newcommand{\svec}{\mathbf s}\) \(\newcommand{\tvec}{\mathbf t}\) \(\newcommand{\uvec}{\mathbf u}\) \(\newcommand{\vvec}{\mathbf v}\) \(\newcommand{\wvec}{\mathbf w}\) \(\newcommand{\xvec}{\mathbf x}\) \(\newcommand{\yvec}{\mathbf y}\) \(\newcommand{\zvec}{\mathbf z}\) \(\newcommand{\rvec}{\mathbf r}\) \(\newcommand{\mvec}{\mathbf m}\) \(\newcommand{\zerovec}{\mathbf 0}\) \(\newcommand{\onevec}{\mathbf 1}\) \(\newcommand{\real}{\mathbb R}\) \(\newcommand{\twovec}[2]{\left[\begin{array}{r}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\ctwovec}[2]{\left[\begin{array}{c}#1 \\ #2 \end{array}\right]}\) \(\newcommand{\threevec}[3]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\cthreevec}[3]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \end{array}\right]}\) \(\newcommand{\fourvec}[4]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\cfourvec}[4]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \end{array}\right]}\) \(\newcommand{\fivevec}[5]{\left[\begin{array}{r}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\cfivevec}[5]{\left[\begin{array}{c}#1 \\ #2 \\ #3 \\ #4 \\ #5 \\ \end{array}\right]}\) \(\newcommand{\mattwo}[4]{\left[\begin{array}{rr}#1 \amp #2 \\ #3 \amp #4 \\ \end{array}\right]}\) \(\newcommand{\laspan}[1]{\text{Span}\{#1\}}\) \(\newcommand{\bcal}{\cal B}\) \(\newcommand{\ccal}{\cal C}\) \(\newcommand{\scal}{\cal S}\) \(\newcommand{\wcal}{\cal W}\) \(\newcommand{\ecal}{\cal E}\) \(\newcommand{\coords}[2]{\left\{#1\right\}_{#2}}\) \(\newcommand{\gray}[1]{\color{gray}{#1}}\) \(\newcommand{\lgray}[1]{\color{lightgray}{#1}}\) \(\newcommand{\rank}{\operatorname{rank}}\) \(\newcommand{\row}{\text{Row}}\) \(\newcommand{\col}{\text{Col}}\) \(\renewcommand{\row}{\text{Row}}\) \(\newcommand{\nul}{\text{Nul}}\) \(\newcommand{\var}{\text{Var}}\) \(\newcommand{\corr}{\text{corr}}\) \(\newcommand{\len}[1]{\left|#1\right|}\) \(\newcommand{\bbar}{\overline{\bvec}}\) \(\newcommand{\bhat}{\widehat{\bvec}}\) \(\newcommand{\bperp}{\bvec^\perp}\) \(\newcommand{\xhat}{\widehat{\xvec}}\) \(\newcommand{\vhat}{\widehat{\vvec}}\) \(\newcommand{\uhat}{\widehat{\uvec}}\) \(\newcommand{\what}{\widehat{\wvec}}\) \(\newcommand{\Sighat}{\widehat{\Sigma}}\) \(\newcommand{\lt}{<}\) \(\newcommand{\gt}{>}\) \(\newcommand{\amp}{&}\) \(\definecolor{fillinmathshade}{gray}{0.9}\)A flowchart for the treatment of patients presenting with systolic HF is depicted in Figure 3.7.1. Medications with a class I indication in patients with systolic heart failure are summarized in Table 3.7.1. Indications, mode of action, contraindications of the medication, and possible side effects of drugs included in this algorithm are discussed below.
| NYHA I & EF <40% | NYHA II | NYHA III | NYHA IV | |
|---|---|---|---|---|
| Diuretic | ||||
| ACE-inhib | ||||
| AT-II antagonist | Alternative | Alternative | Alternative | |
| Betablocker | Post infarction | |||
| Aldosteron antagonist | EF < 35% | EF < 35% | EF < 35% | |
| Nitrate / Hydralazine | Afro-American | Afro-American | Afro-American | |
| Ivabradine | SR>75/min & EF<35% | SR>75/min & EF<35% | SR>75/min & EF<35% | |
| Digoxin |
Angiotensin-converting enzyme (ACE) inhibitors
An ACE inhibitor is indicated for every patient with symptomatic systolic HF and an EF ≤40 % (NYHA class II-IV). (Class I recommendation, level of evidence A) Contraindications for the use of ACE inhibitors are:
- History of angioedema
- Bilateral renal artery stenosis
- Serum potassium concentration >5.0 mmol/L
- Serum creatinine >220 µmol/L
- Severe aortic stenosis
ACE inhibitors relieve the heart by decreasing the preload and afterload. This is achieved through two mechanisms. Firstly, conversion of angiotensin-I to angiotensin– II is inhibited, which reduces vasoconstriction and lowers BP. Secondly, production of aldosterone is decreased, as angiotensin II induces this production. Aldosterone stimulates sodium- and water retention. Possible side effects are symptomatic hypotension (dizziness), hyperkalemia, worsening renal function and cough.
In patients with congestive HF, total mortality and hospitalization are significantly reduced by ACE inhibitors.[8]
Beta Blockers
Beta blockade (in addition to an ACE inhibitor or ARB when ACE inhibitor is not tolerated) is indicated for every patient with symptomatic systolic HF and an EF ≤40 % (NYHA class II-IV) and in asymptomatic patients with a LVEF ≤40% after a MI. (Class I recommendation, level of evidence A).[9] Contraindications are:
- Bronchial asthma
- Second - or third degree heart block, sick sinus syndrome, sinus bradycardia
Beta blockers mainly exert their effect by reducing the toxic effects of the sympathetic nervous stimulation on the heart and by deactivating the renin-angiotensin system.
Possible side effects include (symptomatic) hypotension, worsening of HF and bradycardia. The recommendation is ‘start low, go slow’, i.e. start with a low dose, and titrate every two weeks.
In patients with persistent symptoms after treatment with a combination of beta blocker and ACE inhibitor or ARB, a mineralocorticoid/aldosterone receptor antagonist (MRA) is recommended. (Class I recommendation, level of evidence A)
Diuretics (Loop of Henle diuretics, Thiazides, Aldosterone antagonists)
Diuretics reduce preload by venous vasodilatation and by increasing diuresis. As a result, filling pressures of the heart and the lung vasculature decrease. Although the effects of diuretics on mortality and morbidity have not been studied in patients with HF (irrespective of EF), it is recommended in patients with signs and symptoms of congestion as diuretics relieve dyspnea and edema. Figure 3.7.2 depicts the nephron and the sites where different diuretics work.
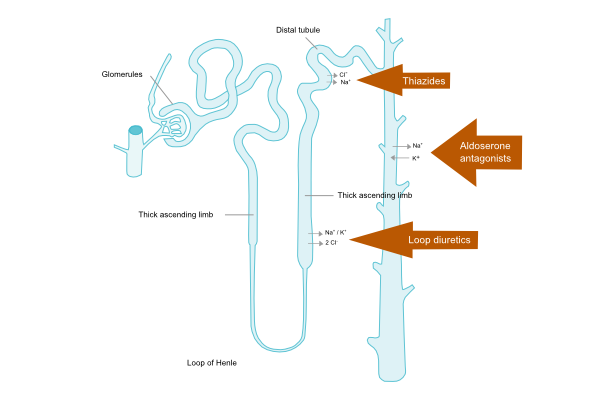
Loop of Henle diuretics
Loop of Henle diuretics act on the ascending loop of Henle in the kidney tubules to inhibit sodium and chloride (and indirectly calcium and magnesium) reabsorption. This will ultimately result in increased urine production of sodium and water. Compared to thiazides, loop diuretics produce a more intense and shorter diuresis.
Thiazides
Thiazide increases urine production by decreasing reabsorption of sodium in the distal tubule. This type of diuretic is often used in combination with loop diuretics to enhance their effects, but may be less effective in patients with a severely reduced kidney function.
Aldosterone antagonists
Adding this drug is suggested for patients with moderate to severe symptomatic HF (NYHA class II to IV, refer to Table 3.7.2) and an LVEF < 35%. (Class I recommendation, level of evidence A) Contraindications:
- Serum potassium concentration > 5.0 mmol/L
- Serum creatinine > 220 µmol/L
- Concomitant potassium sparing diuretic or potassium supplements
- Combination of an ACEI and ARB
Aldosterone antagonists reduce sodium retention by the kidney, and inhibit fibrosis formation in the heart.
Possible side effects include hyperkalemia, hyponatremia, worsening renal function, and breast tenderness and/or enlargement. Eplerenon has less mastopathy side effects and is an alternative to spironolacton. In patients with severe heart failure, spironolactone in addition to standard therapy, reduces morbidity and mortality. [10]
Choice and combination of diuretics
Patients with heart failure may be treated with a thiazide diuretic, which should be switched to a loop diuretic if a suboptimal response occurs. In patients with a decreased renal function, a loop diuretic is the mainstay of treatment. Addition of a thiazide diuretic to a loop diuretic can be considered in case of a suboptimal response of loop diuretic alone, when given in sufficient doses (furosemide 250 mg twice daily), suggesting that diuretic resistance is due to distal tubular increased activity of retaining sodium. In all patients with NYHA II or more, except in those with a creatinine clearance < 20 ml/min (creatinine > 220 micromol/L), addition of an aldosterone antagonist should be considered. In special cases in which hypercapnia plays a role, metabolic alkalosis can result from diuretics, and acetazolamide, a reversible carbonic anhydrase inhibitor, is then prescribed as an alternative diuretic.
Angiotensin receptor blockers (ARBs)
ARBs are recommended in patients who do not tolerate an ACE inhibitor. Until recently, the addition of ARBs was the first choice recommendation in patients with HF and EF ≤40% who remained symptomatic despite optimal treatment with ACE inhibitor and beta blocker. As aldosterone antagonists have also proven their effects in NYHA class II patients, aldosterone antagonists have become first choice additional therapy after an ACE inhibitor and beta blocker. Whether ARBs may still be recommended in this patient group as added therapy after the addition of aldosterone antagonist is not known.
Contraindications are:
- Bilateral renal artery stenosis
- Serum potassium concentration > 5.0 mmol/L
- Serum creatine > 220 µmol/L
- Severe aortic stenosis
Possible side effects include symptomatic hypotension (dizziness), hyperkalemia, and a worsening renal function.
Digoxin
In the past, digoxin was the standard treatment in HF. Digoxin inhibits sodium-potassium ATPase in the cell membrane of the myocytes, and, by decreasing the sodium extrusion, also inhibits the exchange of calcium out of the cell for sodium into the cell. More calcium remains in the myocyte and increases the contractility of the heart. In contrast to other inotropics, digoxin does not increase mortality.
In patients with symptomatic HF and atrial fibrillation (AF) with a ventricular rate at rest of >80 beats per minute, use of digoxin may be considered to slow the ventricular rate. (Class I recommendation, level of evidence C)
Digoxin may be considered to reduce HF hospitalization in patients with symptomatic (NYHA class II-IV) systolic HF in sinus rhythm with an EF ≤45%. These patients should also use an ACE inhibitor (or ARB) and an MRA (or ARB) and preferably a beta blocker. (Class IIb recommendation, level of evidence B) This may also be considered in patients with an EF ≤45% and persisting symptoms despite treatment with an ACE inhibitor (or ARB) and an MRA (or ARB). (Class IIb recommendation, level of evidence B)
Contraindications for the use of digoxin are:
- Second- or third degree heart block without a permanent pacemaker, sick sinus syndrome
- Pre-excitation syndromes
Possible side effects include sinoatrial or atrioventricular block, arrhythmias or signs of toxicity (nausea and visual effects as halos).
Ivabradine
Ivabradine lowers the heart rate through inhibition of the If channel in the sinus node. This drug can be used in patients who are still in NYHA class II-IV after treatment with ACE inhibitor (or ARB), beta blocker and an MRA (or ARB), who have a LVEF ≤35%, are in sinus rhythm and have a heart rate ≥75 beats/min. Ivabradine may also be used in patients who do not tolerate, or have contraindications for the use of beta blockers.
Hydralazine and isosorbide dinitrate (H-ISDN)
H-ISDN can be used as an alternative treatment when both ACEI and ARBs are not tolerated by symptomatic HF patients with a LVEF ≤45% and dilated LV (or EF ≤35%). These patients should also receive a beta blocker and MRA. (Class IIb recommendation, level of evidence B). H-ISDN can be used in addition to the standard HF treatments (ACEI, beta blocker and MRA) in patients of Afro-American descent (Class IIb recommendation). H-ISDN may reduce risk of HF hospitalization and risk of premature death in patients with a LVEF ≤45% and dilated LV (or EF ≤35%) with persistent symptoms despite treatment with beta blocker, ACEI (or ARB), and an MRA (or ARB). (Class IIb recommendation, level of evidence B)
Contraindications for the use of H-ISDN are:
- Symptomatic hypotension
- Lupus syndrome
- Severe renal failure
The H-ISDN combination acts by decreasing peripheral vascular resistance.
Possible side effects include symptomatic hypotension or drug-induced lupus-like syndrome.
Other
- Anticoagulants
- Anti platelet agents
- Statins
- Anti arrhythmic medication
- Calcium antagonists