
1.6: Early Development
- Page ID
- 41542

- Overview of early development
- Patterning
- First trimester:
- Pre-implantation
- Gastrulation
- Differentiation of the ectoderm
- Neurulation
- Neural crest migration
- Differentiation of the mesoderm
- Somite formation
- Heart formation
- Differentiation of the endoderm
- Pharynx formation
- Development of other oral cavity structures
- Salivary gland development
- Lingual papillae development
- Clinical applications of early development
Overview of early development
Human development is the process where a single cell, a visually unremarkable cell except for perhaps its size, slowly changes into trillions (37) of different-looking cells. Embryology is the study of the phases of development, especially the early phases where most of the interesting stuff happens. A round cell, just a ball with no sides and no special parts, grows into an organism with different organs in different places. Fig. 6.1 is the Sun. You see it every day, can you tell whether the photo right-side up? Is there even a right-side up? We are not astronomers, but the Sun looks a bit like a fertilized egg, and in Fig. 6.1 there are no obvious landmarks to orient our view. An egg has a similar amorphous (without shape) appearance, but it morphs (smoothly changes shape) into the embryo shown in Fig. 6.2, which has a head-end and tail-end, and clear beginnings of arms and legs. The first part of this chapter focuses on concepts common to many developmental events seen in chapters 7 through 11. The second half of the chapter covers the details of early development.

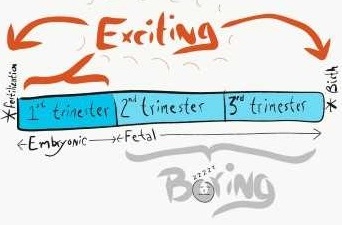
Pregnancy is divided into three equal time periods named trimesters. During the first trimester, a single cell multiplies into a multicellular organism with no discernible shape (other than it is a round blob, not an icosohedron). Starting at week 2, the blob of cells develops into an embryo, which has different shapes. The embryo keeps developing new shapes until it has all of the basic human shapes, such as a head and arms and heart. At this time (week 8) it is a fetus, and the first trimester has ended. The next two trimesters are relatively boring, the fetus grows bigger and the shapes mature, but nothing terribly exciting happens until birth. That’s why this is a Histology and Embryology book, not Histology and Fetology.
As human cells divide during the first trimester, they make decisions as to their cell fate, which ultimately determines the number and location of our arms and legs, our head and heart. These decisions involve signals being sent between cells. Errors in these signals or decisions lead to congenital disorders (or congenital malformation, or birth defects (but see below)). These can happen without known cause. Or, chemicals may interfere with developmental signals, and we call these chemicals teratogens. The most famous teratogen in my country is the drug thalidomide, which– if taken by pregnant women at the wrong time– interferes with the decision-making processes an embryo uses to decide where to grow limbs. This causes phocomelia, or malformation of the limbs. Not every country shares this bias, the teratogenic effects of agent orange (dioxin, which is also found in cigarette smoke) and atomic radiation (pdf download) are notably absent in most American school classes (agent orange and atomic radiation also have adverse effects on adults, and the rate this information reaches the American public is subject to similar biases). We will cover a small number of signals involved in some important decisions that are made during face and tooth development. 37 trillion decisions are made between the single-cell stage and birth, errors are inevitable. Some errors are minor, changing the appearance but not the function of an organ; we might refer to this as a birth mark or human variation. Other mistakes are more severe, interfering with a person’s health, and we refer to those as congenital disorders (or perhaps inborn errors of development, but preferably not birth defects, because our choice of words may influence the amount of health care people seek, it depends on the patient). If you at any time feel like you need more information on embryology, these links are helpful:
- The Embryology Education page
- by Dr. Mark Hill at the University of New South Wales, Sydney, Australia
- Embryo Images Normal and Abnormal Mammalian Development
- by Dr. Kathleen K. Sulik and Dr. Peter R. Bream Jr. at the University of North Carolina School of Medicine.
- The 3D Atlas of Human Embryology
- an open-source collection of 3D pdf files (readable using adobe acrobat reader) by over 70 different students at the Academic Medical Center, Netherlands.
Patterns
This section covers the basic processes that occur during development. Often, more than one process is occurring in the same place at the same time. However, it is useful to think about the following processes separately, the way you might focus on just the vocals– or cello, or guitar, or accordion– in a song.
Cloning
Mitosis produces clones, or identical cells with identical DNA. However, cells differentiate and express different genes to become different tissues and organs. In the first 2 weeks of development, cells divide and produce more identical (albeit smaller) cells. Very soon, cells make decisions as to what they are going to become, and these decisions are coordinated with other cells. Without coordination, an embryo could wind up with two butts and no head.
Differentiation
Differentiation is the process where stem cells begin to express different genes, causing them to appear and function differently from other cells. All cells in the human body have the same DNA, because all cells copied their DNA from the DNA in the zygote (a few exceptional cells change their DNA a bit). The zygote is a toti-potent stem cell, transcription factors could potentially bind to and activate any gene. As cells differentiate, however, they limit their cell fate by putting some genes into deep storage (not actually changing the genetic code, but changing what may or may not be accessible to RNA polymerase).
Differentiation is triggered upon receiving chemical signals. These signals cause target cells to methylate the DNA of certain un-necessary genes, pack those DNA regions around histones, and permanently shut those genes off. For instance, cells fated to become ovaries never synthesize insulin, the gene for insulin is packaged away long before ovaries secrete estrogen or ovulate. DNA methylation and histone packaging limits the fate of these cells. After that, the signals can disappear because the methylation pattern is copied during mitosis and passed to both daughter cells (and their daughter cells). In Fig. 6.7, imagine a signal instructs one cell to methylate green genes, leaving the red genes open to potentially be transcribed. A different signal does the opposite to the other cell. As the red cell duplicates its DNA, it copies the methylation pattern, so that all of its daughter cells cannot express green genes. Meanwhile, the green cell produces a number of daughter cells who have the red gene methylated, none of its daughter cells can express the red gene. We now have 4 red cells, who belong to one lineage, and 4 green cells who belong to a different lineage. Further patterning arises as cells transcribe un-methylated genes. In the cartoon, as red cells transcribe the red gene, this creates a short-range signal which induces nearby green cells to transcribe the dark-green gene. We would say those target cells have differentiated further, and this organism has become even more complicated (3 different cell types). This must continue until we have 200 or so different cell types. Generally speaking, as a cell becomes more specialized, its fate becomes more limited (more DNA methylation and histone packaging), possibly to the point of being limited to just one cell fate.
Induction
One cell may signal to another cell and induce (instructs) that cell to differentiate. Chemicals that can induce another cell to change its shape (to morph) and change cell fate are called morphogens (or sometimes called Growth Factors). Morphogens are similar to neurotransmitters or hormones, they often bind to cell-surface receptor proteins. Activation of morphogen receptors leads to activation of intracellular signals, which in turn can either activate or inhibit specific transcription factors to alter the expression of different genes. Changes in gene expression cause the target cell to look and function differently. Morphogens also change the methylation of genes and their packaging around histones, which is a more permanent change to gene expression. This pattern of gene regulation is passed down to daughter cells, which we learned in Chapter 1 is an example of epigenetic inheritance. By regulating gene expression through both transcription factor activity and methylation, morphogens change not only the morphology the target cell, but their cell fate as well. There are often several closely-related molecules that belong to a family of morphogens, each chemical having a name like morphogen-1, morphogen-2a, morphogen-2b, and morphogen-3. There are a very large number of different morphogens, in this textbook we discuss only a few by name, mostly ones directly related to tooth development, including the Bone Morphogen Protein (BMP) family, the Wnt family, and the Fibroblast Growth Factor (FGF) family. Morphogens can act over different distances listed in Table 6.1. The names of specific morphogens are very important on embryology exams, much less so on dental hygiene exams.
| Distance | Type | Examples |
|---|---|---|
| Direct | Cell-to-Cell | Epithelial-to-neuro-mesenchymal stem cell (Odontoblast differentiation) |
| Cell-to-ECM | Integrin-to-collagen (Ameloblast differentiation) | |
| Short-range | Diffusion through ground substance | Bone Morphogen Protein (BMP), Wnt, Fibroblast Growth Factor (FGF). (Tooth bud induction) |
| Body-wide signals | Hormones | Growth Hormone, Calcitonin. |
Table 6.1: Examples of different type of signals seen during embryogenesis.

Morphogens are secreted into ground substance, creating a concentration gradient of morphogen levels as they diffuse slowly away from the source. The amount of morphogen molecules produced, the relative stickiness of the ground substance, the distance away from the source and the number of receptor proteins on the target cell determine level of a signal cells receives. Sometimes, a morphogen produces visible effects that fall along a gradient (or spectrum), which conceptually matches the gradients we just listed, such as skin color (lighter to darker) or body size (shorter to taller). However, sometimes the effects of a morphogen are more discrete (tooth bud or no tooth bud, there are no half tooth buds). To help explain these observations requires a little knowledge of how transcription factors work. For example, in the French flag model (Fig 141), imagine receiving high levels of the morphogen signal triggers the transcription of a blue gene and inhibits a red gene, causing those cells to differentiate into blue cells. Moderate amounts of the morphogen signal may not be enough to recruit RNA polymerase to the blue gene, but enough to inhibit the red gene, causing cells in regions of moderate morphogen levels to differentiate into white cells. Lastly, cells that receive little or no morphogen signal do not inhibit the red gene, causing them to differentiate into red cells. There are other models that help explain the link between induction and morphogenesis– between a chemical and an organism—for instance a morphogenetic field is less Francophile in nature but harder to visualize. These models all share an important concept: chemical signals can communicate positional information in a developing embryo.
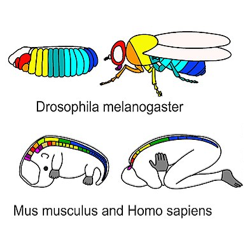
During very early development, regional expression of homeobox genes controls cell fate, not morphology.Homeobox genes are transcription factors that specify which part of the body a particular cell is now a part of, such as part of an arm or face, even if that area has no specific shape yet. They do not encode proteins cause cells to become part of a specific organ. Instead, homeobox genes activate or inhibit a collection of other genes (a program), setting the stage for future changes. In contrast, morphogens like FGF and BMP activate genes that alter a cell or tissues shape (morphology). Homeobox gene expression represents a very specific plan in embryology. It is highly conserved across animal species, and the pattern is very predictable in embryos. The pattern is also relatively simple and linear (Fig. 6.10). Think of homeobox genes like surveyors who determine the locations where houses will be built in a subdivision, while morphogens are the contractors who follow the DNA blueprints for each house, which are built by cells. We can extend this metaphor one step further: in a subdivision, houses are similar, derived from one basic blueprint, but given slight modifications with each re-use.
![[animate output image]](https://med.libretexts.org/@api/deki/files/22913/animate-output-image.gif?revision=1)
The ability of a tissue to create its own patterns is called self-organization (in contrast, maternal effect genes from mom’s cells guide patterns in the embryo’s cells). This involves multiple morphogens, initially expressed randomly. Interactions between these morphogens leads to a stable pattern of expression, and a complex pattern of differentiation. For instance, some morphogens block other cells from producing the same morphogen. In Fig. 6.11, imagine a blue morphogen induces one cell to differentiate into a blue cell, but blocks neighboring cells from becoming blue cells. These neighbors would be free to differentiate into red cells. At the same time, a distant cell produces red morphogen, which induces it to differentiate into a red cell, but blocks its neighbors from doing the same. Its neighbors would be free to produce blue morphogen and differentiate into blue cells. The initial pattern that arises is alternating rings of red and blue cells. However, rings produce regions of red-next-to-red and blue-next-to-blue, which violates our make-believe rules, and this starts a battle. To minimize the number of red-next-to-red and blue-next-to-blue, cells change their cell fate until a stable pattern arises, in this case stripes. It would be hard to predict from the start which cells would be red versus blue, but you could predict the development of red and blue stripes. If these were pigment-producing cells in a zebra, we’d have a zebra with stripes (the best type of zebra). But this pattern could also be alternating regions of oral mucosa that grow a tooth bud or don’t grow a tooth bud, ensuring each tooth bud has enough space to grow (if you want to go down a rabbit-hole, these interactions can be modeled mathematically). When a morphogen blocks another signal, we call that antagonism, and antagonist signals are just as common as induction signals. They must, after all, it is fundamentally just as important to grow one head as it is to not grow two heads.
Proliferation
Growth of a tissue is called proliferation. Proliferation occurs either by mitosis (adding cells) or by adding extra-cellular matrix (synthesizing proteins or other molecules). When new growth happens next to a region of older growth, this is appositional growth, whereas if growth happens from within and pushes older tissue outwards, that is interstitial growth. Dense tissues, such as bone, enamel and dentin, undergo appositional growth. Softer tissues like mesenchyme grow interstitially.
The growth of a tissue is regulated by hormones, such as Growth Hormone, which coordinates the rate of growth of tissues body-wide. On the other hand, local-acting morphogens cause small regions to grow faster than neighboring regions. To make room for new cells while still maintaining a single-layer of cells connected to their neighbors by desmosomes and tight junctions, an epithelium bulges inwards or outwards if it can’t grow wider. An outward growth is known as a bud, and an inwards growth is an invagination. Arms and legs grow from buds, while teeth, hairs and the brain grow from invaginations. These are both forms of interstitial growth.
Morphogenesis
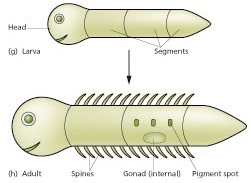
Morphogenesis is the appearance of new shapes in an organism. It means to go from no shape to some shape. The word morphology can mean the study of these shapes, or be used as an adjective to mean the shape of something (For example, a cleft palate is a chance to the healthy morphology of the palate.) From the zygote to the blastula stage (sometimes referred to as the germinal stages) the ball of cells is amorphous, it has no shape (other than being a sphere). At the start of gastrulation, however, the embryo undergoes numerous morphological changes. New shapes arise in the developing embryo. It develops an inside and an outside, a tail end and a head end, soon it develops a left and right, and a front and back. After that, a nervous system and a circulatory system become visible. How long do you think it takes before teeth develop? The answer may surprise you.
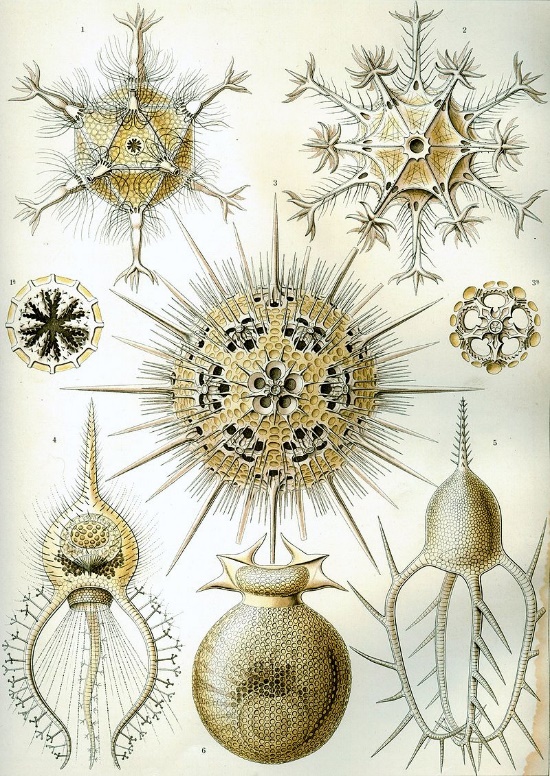
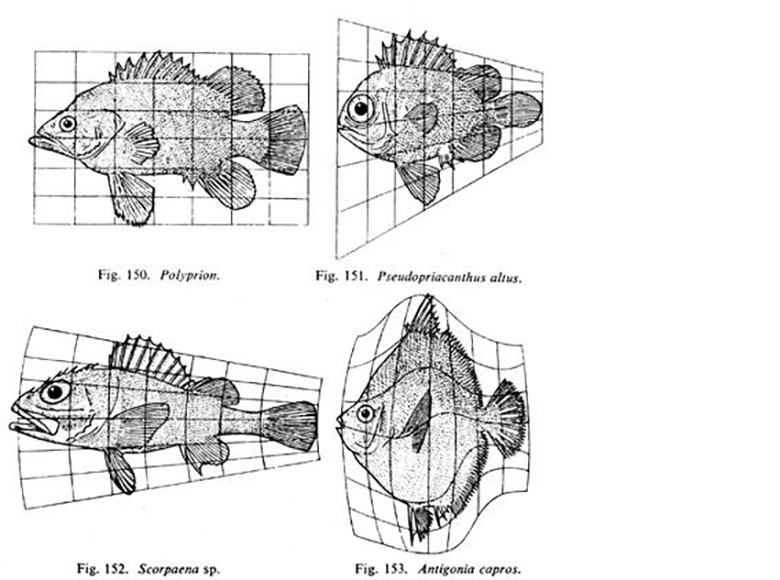 Figure 6.15: D’Arcy Wentworth Thompson proposed that what may look like different shapes in related species may be transformations of one basic pattern. Image credit: “Fig 150-153” by D’Arcy Wentworth Thompson, On Growth and Form is in the Public Domain, CC0
Figure 6.15: D’Arcy Wentworth Thompson proposed that what may look like different shapes in related species may be transformations of one basic pattern. Image credit: “Fig 150-153” by D’Arcy Wentworth Thompson, On Growth and Form is in the Public Domain, CC0Fig. 6.14 is a famous drawing of tiny sea creatures with mineralized exo-skeletons. This image was later analyzed by a mathematical biologist named D’Arcy Wentworth Thompson, who noticed different biological shapes can be different transformations of the same shape. Transformations, he proposed, occurred by different localized rates of growth– something our current knowledge of morphogen signaling supports– as he illustrated in Fig 6.15. He is regarded as the first person to describe morphogenesis. When Thompson looked at the tiny sea creatures, he didn’t see different shapes, he saw changes to one shape. These changes happened over evolutionary time, and led to different-looking sea creatures (who shared a single lineage). In this book, we look at different body parts that share the same lineage but change over developmental time, such as hair follicles and tooth buds. Thompson’s ideas were expanded upon by the mathematician Alan Turing, who coined the term morphogenesis. His other achievements include inventing computer science and breaking the Nazi code during WWII (with the help of many female mathematicians at Bletchley park). Sadly, he committed suicide after his arrest, conviction and imprisonment for homosexuality by the British government he helped save. Their government’s view on homosexuality has developed since then, we can understand the current view better by following its lineage.
Morphogenesis and genetics
To have a well-rounded understanding of how morphogen signaling works, it helps to understand some concepts of genetics. When we say understand, we don’t mean meorize the specific details, focus on the concepts. First, pay attention to when we discuss a morphogen, we likely mean the signaling molecule itself. We at times discuss the morphogen signal, and that extra word signal makes a big difference. Mutations that alter morphogen signals include mutations to the gene for the extra-cellular morphogen molecule itself (if it is a protein such as FGF and BMP) or enzymes that synthesize the morphogen (as is the case with Retinoic Acid), cell-surface receptors for the morphogens, cytoplasmic second messengers and nuclear transcription factors. Discussing morphogen signaling levels saves us from the complexity of including all possible targets. Next, some mutations might be gain-of-function, such as a mutation to a receptor that prevents it from shutting off, and these are often inherited in an autosomal dominant fashion (it only takes 1 faulty allele to create a signal where it shouldn’t be). Alternatively, loss-of-function mutations prevent proteins from functioning properly, and are often inherited in an autosomal recessive pattern (it takes both copies to be faulty to lead to a loss of a signal where it should be, one good allele would be enough). Some mutations fully stop, or fully start, morphogen signals. and in such cases we would say theses mutation have complete penetrance. Other mutations might partially block or partially start morphogen signals, and have partial or incomplete penetrance, the severity of the symptoms fall on a spectrum.
Maturation
Maturation is the process by which new shapes created by morphogenesis continue to develop and take on a more mature form. By the end of week 9, all of the basic organ shapes have formed, and we say the embryonic period is over and the fetal stages begin. The fetus undergoes maturation, and maturation involves bits of the previous processes (another way of saying that is maturation recapitulates other developmental processes).
Fusion
Sometimes, two separate bits of the same type of tissue come into contact with one another and fuse into a single tissue. For an epithelium, this requires the cells share the same type of trans-membrane protein known as a cell adhesion molecule. For a connective tissue, this requires the correct integrin binding to fibronectin. In Fig 147, the basic pattern of green being on the outside and red in the middle is initially disrupted by the fusion of two structures. There are three ways to remove green cells from the middle area. The first way is for cells to receive guidance cues and cause cells to move. Some guidance cues are repulsive, such as the lack of correct cell-to-cell contacts, or high concentrations of a repulsive morphogen. Other guidance cues are attractive, such as the correct cell-to-cell contact or a positive guidance morphogen. Whether a cell-to-cell connection or morphogen is attractive or repulsive depends on how the target cell has been programmed (what receptor genes it is expressing). Cells in the incorrect location can also be induced to undergo apoptosis (see below). Lastly, another way to re-organize cells is to induce them to de-differentiate (revert to a stem cell) and differentiate into the correct cell type. This is called a transition; both early development and tooth development involve examples of epithelial-to-mesenchymal transitions and mesenchymal-to-epithelial transitions.
Apoptosis
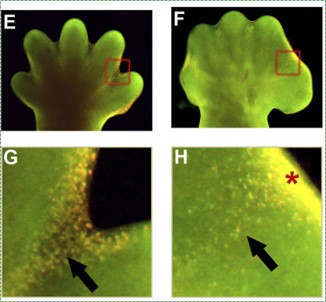
In the construction of tall buildings or large ships, scaffolding is built first to allow the construction workers to get where they need, then removed after construction is complete. Similarly, during development, apoptosis is an integral part of the construction of body parts. Many tissues grow more cells than are needed in the mature form. To undergo maturation, un-needed cells undergo apoptosis. For instance, during the growth of bone tissue, extra cartilage tissue is made to act as a scaffold for osteoblasts. Shown in Fig. 6.18, the hands and feet start off as paddles, and only with apoptosis in alternating regions does morphogenesis of fingers and toes occur. Without enough apoptosis, people are born with webbed fingers or toes, or suffer ankyloglossia (their tongue is rigidly anchored to the floor of the mouth by a pronounced lingual frenulum).
Early development
Pre-implantation period
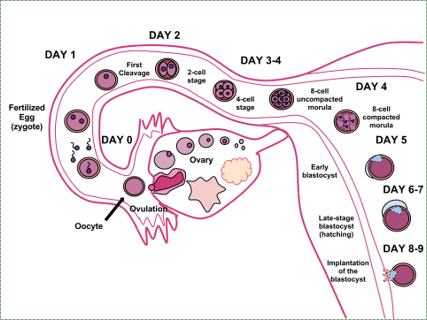
The pre-implantationperiod begins with fertilization, spans a week or so of development, and ends with an embryo implanting into the uterus. Fertilization is the union of one sperm cell and one egg– thousands of sperm are needed, but only one is allowed into the egg. This union joins 23 maternal chromosomes with 23 matching paternal chromosomes, forming a zygote. Fertilization most often occurs towards the distal end of a fallopian tube. Over the next week the zygote undergoes mitosis and increases in cell number, but it does not grow in size. All of the amino acids and nucleotides for making new cells during this first week come from the cytoplasm of the zygote, which is why the egg is a very large cell. After implantation, the uterus provides the raw materials for an embryo to grow larger.
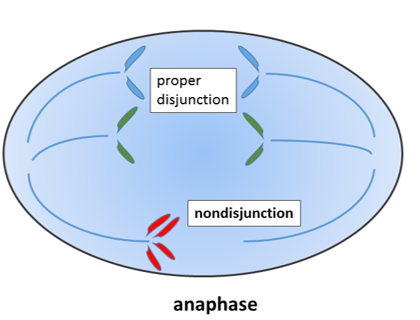
During mitosis, the 23 pairs of chromosomes are duplicated and divided between 2 daughter cells evenly. If mistakes are made and an odd number of chromosomes wind up in a daughter cell, this fails a cell cycle checkpoint and triggers apoptosis. If a chromosome breaks, it can lead to the same result.

There are exceptions, however. A cell with an odd number of chromosome 21 or 23 can survive. If that cell is the egg, then the zygote and all subsequent cells will have an odd number of chromosomes. This leads to congenital disorders such as Trisomy 21. If the chromosomal segregation error happens at the 2-cell stage of development, then only half of the cells in the adult would have an extra chromosome, and the condition would be less severe. Extra chromosomes interfere with decision-making processes in development. People with Trisomy 21 frequently develop microdontia, and may suffer from hypo-salivation and bruxism. They therefore need extra care maintaining healthy oral hygiene.

Early divisions
During the first week of development, the zygote undergoes 3 cleavage divisions, where mitosis occurs in a synchronized fashion (see a cool video here). The cells duplicate along a single plane, 3 times, producing an 8-cell embryo. Synchronizing mitosis requires cell-to-cell communication between gap junctions to coordinate cell cycle checkpoints. Synchronized mitosis leads to the embryo developing evenly. The fact that multiple cells are dividing in the same direction means these cells have some polarity, even if the embryo as a whole has no visible top or bottom yet. As mitosis continues, the number of cells continues to double, but the cells do not divide along the same plane. This solid ball of cells is called a morula. As mitosis continues, the cell count doubles and the cells continue to get smaller, until the solid ball of cells becomes a hollow ball of cells named a blastula. From the zygote to the blastula stage, none of the cells appear any different except in size. A fancier way to say this is that there are no changes to morphology. During the blastula stage, a group of cells named the embryonic disc move away from the others. The fate of the embryonic disc is to become the embryo, while the outer cells, known as the trophoblast, are fated to become extra-embryonic structures such as the placenta. The blastula implants in the endometrium about a week after fertilization and continue developing.
Gastrulation
It is not birth, marriage, or death, but gastrulation, which is truly the most important time in your life.–Lewis Wolpert.
Gastrulation overview
During gastrulation, some cells invaginate, forming a layer of cells on the inside and a layer of cells on the outside of the embryo. The significance of this is that this is the first instance where embryonic cells are different from one another. But, wait, if all the blastula cells are identical, why did only some of them migrate? Mitosis does indeed generate 2 cells with identical DNA, but not necessarily identical cytoplasm. If an egg has mRNA for a transcription factor clustered into one spot in the cytoplasm, the first cleavage division produces two non-identical cells, one with the transcription factor mRNA and one without. Later, when the mRNA is translated, it could induce that cell to migrate inwards, while other cells stay on the outside. This is s a maternal effect, because the mRNA for the transcription factor is not transcribed from the zygotes’ DNA, but is made by mom’s ovary cells and deposited into the egg. Lets return to gastrulatiojn: the end result of gastrulation is an embryo with two layers (outside and inside). Imagine holding a tennis ball and pushing your thumbs inwards, forcing some of the outer rubber to fold inwards. The tube that forms becomes the gastrointestinal tract, and the opening (can you guess?) becomes the anus. The embryo therefore now has a distinct tail direction and head direction. Fig. 6.23 represents the way a sea urchin gastrulates. Human embryos look different because it is only the embryonic disc that undergoes gastrulation, not the entire blastula. But the 2 layers are the same, human gastrulas simply look more squashed. Oh, and sea urchins don’t form anus-first. The reason sea urchin gastrulation looks simpler than human gastrulation is that human blastulas reserve some cells (the trophoblast) to form a placenta and amnion, while sea urchins dump their eggs into the sea. We are sacrificing a little accuracy here to focus on important concepts shared across species. If you are curious, watching movies of these processes in humans is not possible, but it is for organisms like xenpous laevis (frogs).
Next, cells from the outer layer migrate between the two layers. This gives the embryo 3 layers, which are the 3 embryonic germ layers (Fig. 6.23). The outer layer of ectoderm and the inner layer of endoderm remain epithelial in appearance, while the middle layer of cells (mesoderm) undergoes a morphological change, and becomes mesenchyme. This migration begins at a single location called Hensen’s node, which moves down the embryo forming the primitive streak behind it (Fig 6.24). The side of the embryo with the node is fated to become the dorsal side, and the streak divides the embryo into a left-half and a right-half. You have now witnessed, albeit in cartoon form, how something (all the basic body directions) arose from nothing. Don’t let the significance of this sneak past un-noticed. Scientists have a hard time explaining what there was before the universe formed, or how the Earth went from having no life to having life. Embryologists, by contrast, explain how embryos change from having no shape to having shape in great detail (we’ve had the benefit of directly watching and manipulating this process).
| 3 embryonic layers | Cell fate |
|---|---|
| Ectoderm | Epithelium of skin and oral mucosa, neural tissue |
| Mesoderm | Connective & muscle tissue |
| Endoderm | Epithelial lining of hollow organs |
Table 6.2: The three germ layers develop during gastrulation
Epithelial-to-mesenchymal transition
The process by which ectodermal cells quit being ectoderm and migrate to the middle and form mesoderm is called an epithelial-to-mesenchymal transition (EMT). The epithelial cells of the ectoderm must first lose their cell-to-cell contacts with neighboring cells, which makes them less-epithelial. They lose their polarity, de-differentiate into a stem cell, then differentiate into mesenchymal stem cells. This process is not only required to form mesoderm during gastrulation, it occurs during neural crest migration, wound healing, and cancer metastasis. Cells in the mesoderm (the name for the middle layer) form mesenchyme (a type of tissue), while the other two layers remain epithelial. There is a reverse process, called a mesenchymal-to-epithelial transition (MET), which also occurs during wound healing. EMT allows epithelial stem cells from a healthy region of oral mucosa to turn into mesenchymal stem cells, migrate away from the healthy region into a damaged region. MET then allows the mesenchymal stem cells to turn back into epithelial stem cells, which divide and differentiate into new keratinocytes. Because this mimics what happens during gastrulation, we say “wound healing recapitulates (states again) development”.
Differentiation of ectoderm
Neurulation
Gastrulation gave the embryo its first polarity, as well as the beginning of the GI tract. One of the next organ systems to develop is the central nervous system. The basic processes used in neurulation are re-used when other hollow organs form. First, underlying mesoderm known as the notochord sends morphogens to nearby ectodermal cells. This induces the nearby region of ectoderm to differentiate into neuro-ectoderm, followed by local proliferation. Because these epithelial cells cannot easily spread side-to-side, they invaginate. Ultimately, invaginating neuro-ectodermal cells lose their contacts with the ectoderm and fuse to other neuro-ectodermal cells, creating a new structure called the neural tube. This tube develops into the brain and spine. If you are wondering about the notochord, its cell fate is to mostly undergo apoptosis, although some remains as the nucleus pulposis of the vertebral discs. In tiny fish-like chordates with no backbone called amphioxis, the notochord persists. This wont be the last time you see a human embryo make a structure that goes away or changes entirely.
The neural tube begins folding from the anterior portion of the embryo, and zips up in an anterior-to-posterior direction. The zippering is not perfect, the anterior end is also growing wider as it is folding to form the primitive brain. For all of the developmental processes we do and don’t cover, the anterior end is usually the region that develops first, followed by more posterior regions. Zipping the neural tube requires adequate levels of folic acid, so it is important that mother’s melanin has protected this vitamin, otherwise incomplete closure of the neural tube may result (spina bifida).
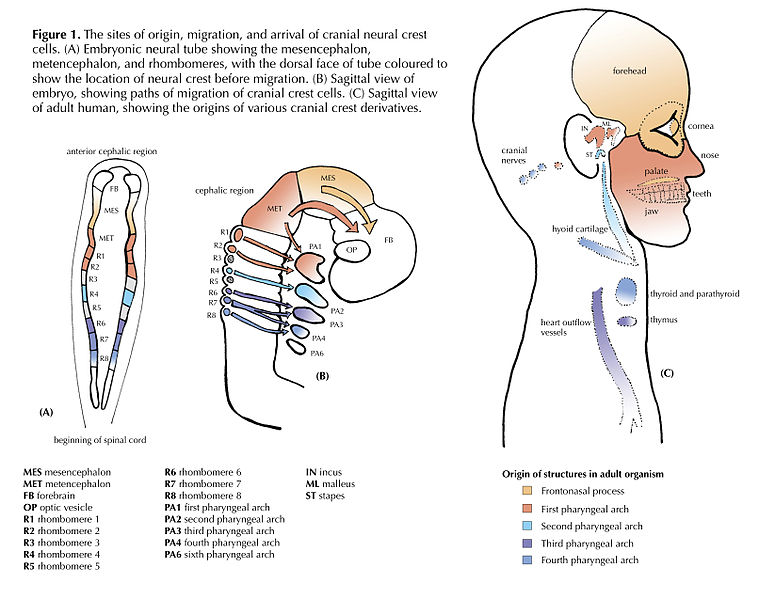
Some of the neuro-ectoderm cells do not fuse. Instead, these cells undergo an epithelial-to-mesenchymal transition and migrate away from the neural tube. These cells are neural crest cells, they are fated to become a number of important cells and tissues throughout the body including melanocytes, odontoblasts, dental pulp, cementoblasts, and the neuro-mesenchyme of the pharyngeal arches. These cells are sometimes referred to as the fourth embryonic tissue (in addition to the three that arise during gastrulation), which suggests some people think neural crest are important. Even after neural crest cells migrate to new and distant tissues, they often retain visible signs of their neural lineage, such as the dendrites on melanocytes or the odontoblastic process of odontoblasts. To make migration easier, neural crest cells express an enzyme called a matrix metalloproteinase (MMP). This enzyme digests proteins found in the extra-cellular matrix. By now we hope remember the phrase wound healing recapitulates development, matrix metalloproteinase enzymes are re-used to heal certain type of tooth wounds. When neural crest cells reach the pharyngeal arches, they secrete the morphogens FGF and BMP, which antagonize each other, producing a striped pattern along the ectoderm. Some regions are induced to form tooth buds, the in between regions produce oral mucosa.
Differentiation of mesoderm
Somite formation
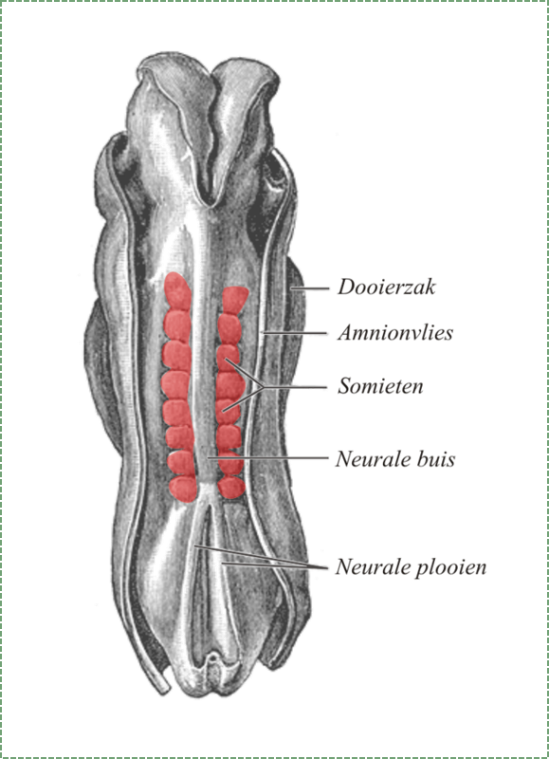
During the same time as neurulation, mesoderm undergoes differentiation. Mesoderm starts off as an amorphous layer of mesenchyme. Then, regions of mesenchyme pinch off in repeating spherical structures called somites, forming segments along the anterior-to-posterior axis of the embryo. The fate of the somites is to become solid organs, either repeating units of connective tissue such as the ribs and vertebrae, or repeating units of muscle tissue such as the rectus abdominus and intercostal muscles. The formation of each somite involves a mesenchymal-to-epithelial transition, some mesenchymal stem cells differentiate into an epithelium that separates one somite from the next.
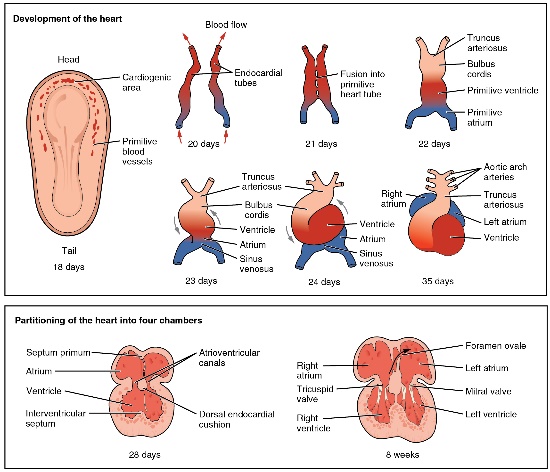
Formation of the heart
In the third week, mesoderm also begins to develop into blood, the heart and the circulatory system. Mesenchymal stem cells first differentiate into blood islands. Next, angiogenesis begins. Two large blood vessels fuse– with some help from neural crest cells– to form the primitive heart, which begins beating.
Differentiation of endoderm

Formation of the pharynx
The endoderm that migrates interiorly during gastrulation extends its way towards the anterior end of the embryo. This forms the primitive foregut, which later becomes the pharynx, oral cavity and nasal cavity. At this time, however, there are no openings for the mouth and nostrils.

4th week
We are now only up to the 4th week of development. A lot has happened! At this time, the embryo continues to undergo local regions of proliferation, patterning, fusion and the other processes covered at the beginning of the chapter. This leads to the formation of rudimentary (basic) structures. When a structure first becomes visible from the surface of an embryo, it is often called a placode (an ectodermal thickening). The cells in a placode are fated to become an organ, but their overall shape is no more than a raised bump or shallow pit. By the 4th week, head-related organs listed in Table 6.3 begin to develop.
| Structure | Fate |
|---|---|
| Eye placodes | primitive eyes |
| Otic placodes | primitive ears |
| Nasal placodes | primitive nose |
| Pharyngeal arches | so many things they get their own chapter |
| Oro-pharyngeal membrane | primitive mouth (not open yet) |
Table 6.3: primitive structures formed during the 4th week of development
Clinical applications of early development
Disturbances in these early stages of development are usually so severe the embryo does not survive. However, clinical conditions exist related to these early stages and to oral health.

Homeobox gene mutations
Mutations to homeobox gene can cause entire structures to be missing, or to develop in the wrong location. Early experiments on flies led to observations of legs where antennae should be located, or antennae where wings should be located. There are a few homeobox-related genetic disorders in humans. Homeobox-related disorders are rare because the mutations are usually lethal, but when they aren’t the conditions are often severe. A small list is found in Table 6.4
| Syndrome | Homeobox gene involved | Symptoms include |
|---|---|---|
| Axenfeld-Rieger Syndome | FOXC1, PITX2 | Mostly eye-related, sometimes hypodontia and microdontia |
| Autosomal dominant syndactyly | HOXD13 | Syndactyly (fused fingers or toes) |
| Guttmacher syndrome | HOXA13 | Polydactyly (extra fingers or toes) |
| Ectodermal dysplasia | HOXC13 | See below |
Table 6.4: A few examples of homeobox mutations in humans.

Apert syndrome
Apert syndrome is caused by a mutation in the receptor for the morphogen FGF. It is categorized by a wide range of symptoms, including cranial deformations and syndactyly. FGF is involved in the formation of the pharyngeal arch apparatus (covered in the next chapter), which explains the craniofacial abnormalities. Relevant to this chapter is the ability of FGF (like many growth factors) to inhibit apoptosis. Having a mutation that causes an FGF receptor to be on all the time inhibits apoptosis in the hand and foot paddles. Regions of apoptosis are required to produce fingers and toes, hence this mutation leads to syndactyly. Partial disturbances to FGF and BMP signals can lead to partial syndactyly, or webbing of the fingers or toes.
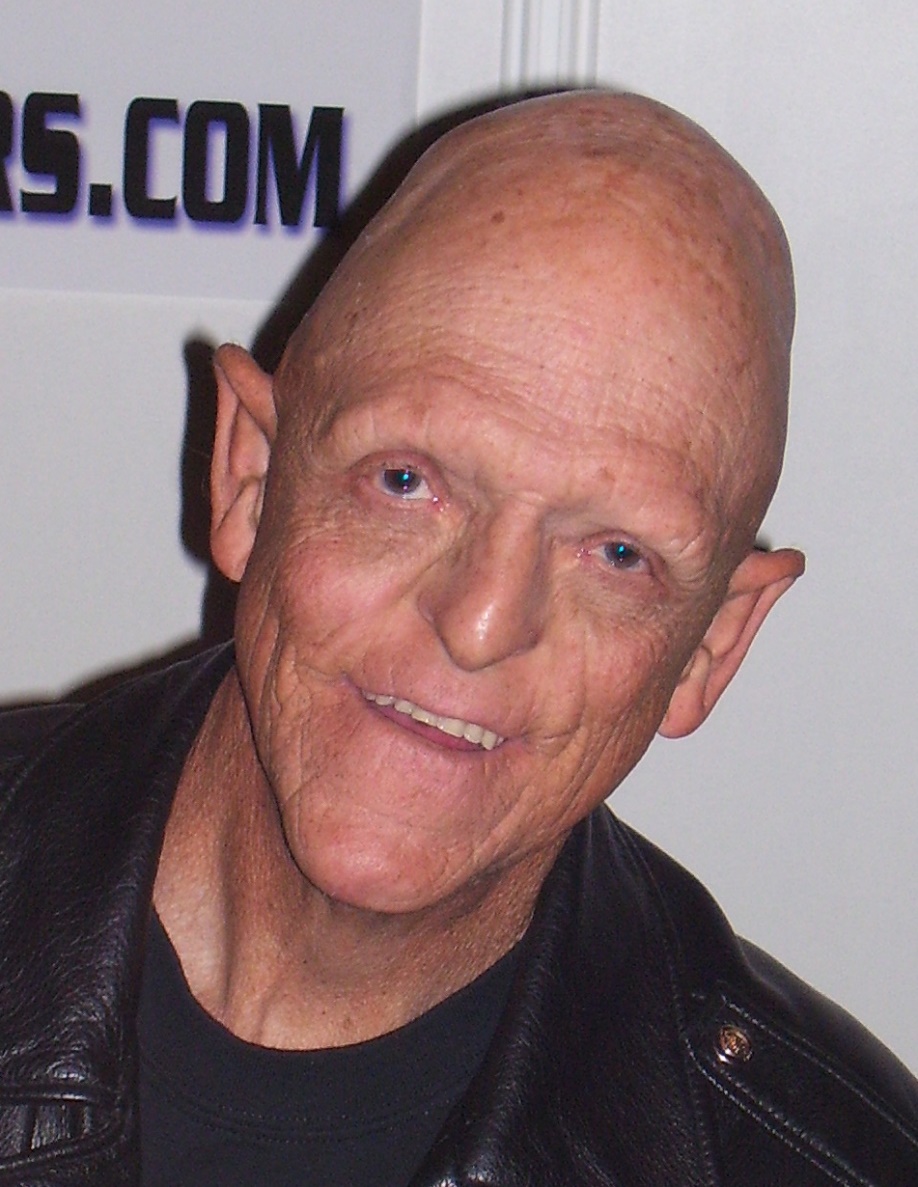 Figure 6.35: Figure 185: “Michael Berryman, actor” by Stefan Borggraefe is licensed under CC BY 4.0
Figure 6.35: Figure 185: “Michael Berryman, actor” by Stefan Borggraefe is licensed under CC BY 4.0Ectodermal Dysplasia (part 1 of 2)
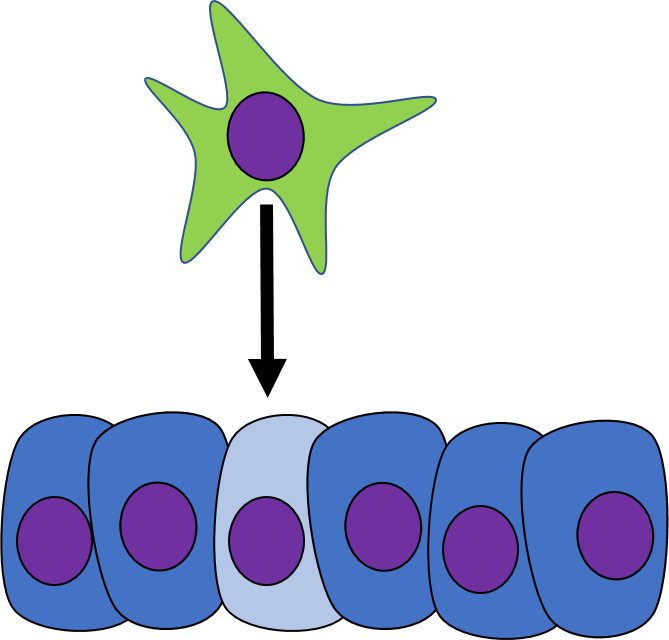
Problems with the induction of neural crest cells during neurulation leads to disturbances in the formation of teeth, hair follicles, salivary glands and other structures. What these have in common is they are all specialized structures of the ectoderm, induced by neural crest cells to differentiate. In a healthy embryo, ectodermal cells receive morphogens which activate or inactivate the correct transcription factors to trigger differentiation into neural crest cells. Neural crest cells migrate to distant regions of the body, determine their location by interacting with morphogens in the ground substance, and release other morphogens to induce regions of ectoderm to differentiate into sweat glands, salivary glands, tooth buds or hair follicles. Mutations in any of the genes for these morphogens, their receptor proteins, or down-stream transcription factors may lead to a condition named Ectodermal Dysplasia. This group of syndromes is rare, with only 7,000 cases worldwide, but there are at least 40 different genes have been implicated in these syndromes. Compare that to Sickle Cell Disease, which currently affects over 100,000 Americans (predominantly African Americans, Hispanic Americans, Greek Americans, Turkish Americans and Italian Americans), all due to mutations in a single gene, Hemoglobin-Beta. The point of this comparison is to highlight when these genes are expressed. The induction of ectodermal stem cells to proliferate and differentiate into different appendages is complex and occurs during embryogenesis. Mutation in the morphogens, the morphogen receptors, the second messengers or transcription factors and downstream genes that are activated to induce differentiation are all possible targets that cause ectodermal dysplasia. Mutations in these genes in a neural crest cell leads to a disruption in any of the subsequent cells induced by this new cell type, similar to the way tackling the ball carrier in socer (football) disrups the gameplay of any of his or her potential passing targets. By comparison, only red blood cells express hemoglobin-beta, and they are terminally differentiated cells, they do not become any other cell type. Obviously red blood cells are an important cell type, one that can be found early in embryogenesis, but the symptoms of Sickle Cell Disease present less of a spectrum than the types of diseases we have been discussing, such as Ectodermal Dysplasia.
 Figure 6.36: Gaten John Matarazzo III, actor and CCD activist. Image credit: Gaten John Matarazzo III, by Gage Skidmore, is licensed CC BY SA 3.0
Figure 6.36: Gaten John Matarazzo III, actor and CCD activist. Image credit: Gaten John Matarazzo III, by Gage Skidmore, is licensed CC BY SA 3.0
Cleido-cranial Dysostosis
Cleido-cranial dysostosis (CCD) is a congenital disorder caused by a mutation to a transcription factor required for the differentiation of bone and teeth. It is required to trigger osteo-chondro-progenitor cells to exit the cell cycle and differentiate into osteoblasts. It is also re-used to induce the differentiation of odontoblasts. Furthermore, after teeth have formed, this transcription factor is re-used to activate the expression of a Matrix metalloproteinase enzyme, which is necessary for remodeling of the alveolar sockets. Without this enzyme, retention of deciduous teeth occurs. Dental implants or dentures (such as the ones the actor and CCD-philanthropist Gaten John Matarazzo III received in Fig. 6.36) are the preferred treatment. In addition, a person with CCD may have small clavicles and changes to shape of the skull– bones that form by intra-membranous ossification. This illustrates two major concepts in development. First, many structures form one way, but are remodeled later to serve a different function (teeth form by folding inwards, they later move outwards). Secondly, many different patterns in embryology are re-sued (recapitulated), such as the removal of tissue during neural crest migration and the removal of tissue during tooth eruption.
Stem cell therapies
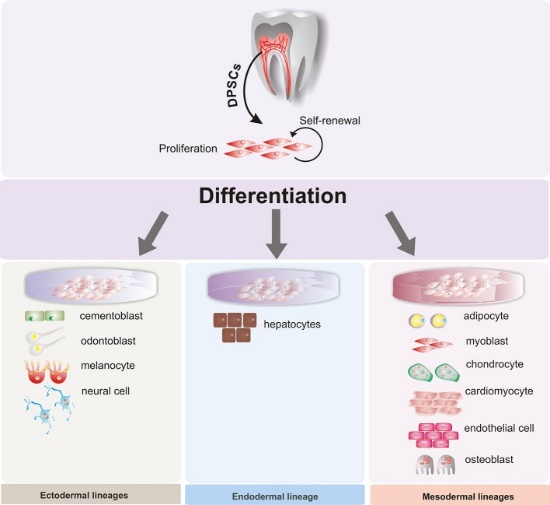
When cells terminally differentiate, they permanently inactivate un-needed genes by methylation and storage around histones. Researchers are learning ways to reverse this process, and guide differentiated cells to revert to a stem-cell state. This raises the possibility of promoting regeneration of tissues that do not otherwise regenerate, removing the need for tissue grafting or transplantation. Because some dental tissues do not regenerate well, there is potential for these technologies to be applied to the oral cavity, such as growing biological dental implants instead of using metals and ceramics. However, more interest has been placed on acquiring mesenchymal stem cells from dental tissues. For instance, stem cells isolated from maxillary third molars have been used in clinical trials to improve healing and reduce the need for transplanted tissue in maxillofacial surgery. Because of their potential to differentiate into a wide array of cells, great interest has been placed on collecting dental stem cells to treat diseases unrelated to the oral cavity. With the correct morphogen and plenty of dental stem cells, it may be possible to reverse the damage caused by neurodegenerative disease such as Alzheimer’s Disease (AD) and Parkinson’s Disease (PD), spinal trauma, myocardial infarct (heart attack), and Muscular Dystrophy (MD). The lineage of the cells that produce dentin, pulp, cementum and the periodontium will help explain the link to neurodegenerative disoders. What else will you do with extracted third molars? Unfortunately, there is no legal definition in the U.S. for what constitutes safe, effective stem cell therapy. Even if good rules are put in place, medical-tourism does not abide. In addition to honest and good research in stem cell therapies (the Institute for Stem Cell and Regenerative Medicine at the University of Washington is a good example), there are a large number of dubious-to-downright-quack stem cell clinics operating in the grey market, using risky, untested methods and making absurd claims to take as much money as possible from vulnerable people. So, who’s who? Therapies that use or boost a patient’s own stem cells have the best possible chance of providing positive outcomes with minimal risk of side-effects– especially if that therapy is targeted, such as by adding a specific morphogen to boost a specific result. On the other hand, throwing exogenous stem cells at a problem– cells from other people, other animals, or from non-animal sources– carries the biggest risk of serious adverse effects with minimal potential for benefit. Keep in mind that 19 out of 20 (or so) potential drugs that are shown scientifically to work in animal models fail in human trials. That means there is scientific evidence in publication for treatments that we know don’t work, but other people can cherry-pick the positive information and use it to sell a product.
Chapter 5 * Chapter 7