1.15: Laryngofissure Technique
- Page ID
- 17626

OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
LARYNGOFISSURE / MEDIAN THYROTOMY
Johan Fagan
Laryngofissure, also known as median thyrotomy, refers to vertically splitting the thyroid cartilage in the midline to gain access to the endolarynx. It provides good exposure to both anterior and posterior laryngeal structures with very minor morbidity (Figure 1).
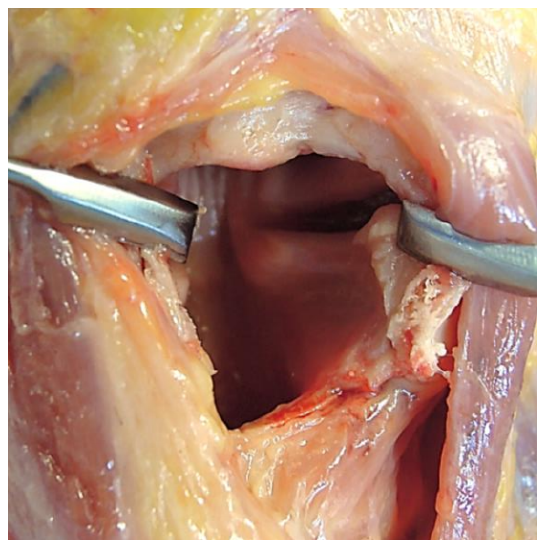
Figure 1: Good exposure to both anterior and posterior laryngeal structures
Indications for laryngofissure
Laryngofissure has largely been supplanted by transoral microsurgery. Yet it remains relevant in settings where endolaryngeal approaches are not possible due to lack of suitable microlaryngeal instrumentation and/or CO2 laser capabilities. Other indications include the following:
- Transoral approach not possible due to anatomical constraints
- Laryngeal trauma (evacuate hematoma, repair lacerated or avulsed vocal cords, or insert a laryngeal stent)
- Cordectomy for T1/T2 glottic cancer
- Excising benign laryngeal tumors and masses
- Arytenoidectomy and lateralization of vocal cord for vocal cord paralysis
- Laryngeal stenosis and webs including insertion of a laryngeal keel for an anterior web (Figure 2)
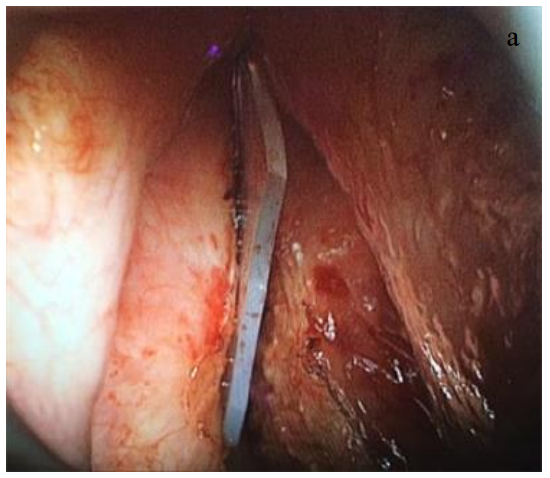

Figures 2a, b: Laryngeal keel for anterior web
Relative contraindications
- Tumor involving thyroid cartilage and anterior commissure
- Laryngeal papillomatosis as laryngofissure may disseminate papillomata into the tissues of the neck
Surgical technique
- Because the airway is entered (clean contaminated wound), the patient must have perioperative (24 hours) broad spectrum antibiotics
- Tracheostomy is done to permit surgical access to the endolaryngeal structures and to secure the airway until postoperative swelling has abated
- Perform direct laryngoscopy to assess the laryngeal pathology
- Position the patient with neck extended
- Make a transverse skin crease incision midway between the thyroid prominence and the cricoid (Figure 3)
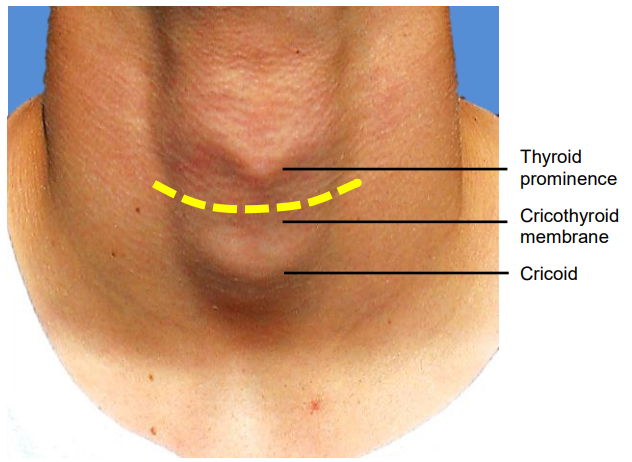
Figure 3: Surface anatomy and incision (yellow line)
- Raise skin flaps superiorly and inferiorly (platysma is generally absent in the midline)
- Incise the midline raphe between the sternohyoid muscles to expose thyroid cartilage (Figure 4)
- Clear all the soft tissue off the thyroid cartilage, cricothyroid membrane and cricoid in the midline (Figure 5)
- Expose the cricoid cartilage and cricothyroid membrane
- Incise thyroid perichondrium vertically in the midline and strip it off the cartilage to expose a midline strip of cartilage
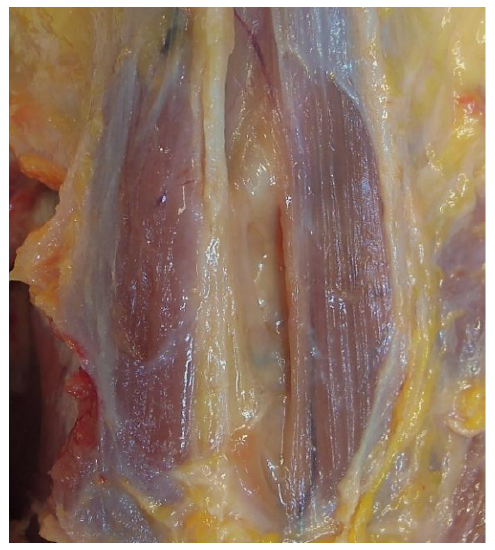
Figure 4: Raphe between sternohyoid muscles has been divided to expose the thyroid cartilage

Figure 5: Thyroid cartilage, cricothyroid membrane and cricoid exposed in midline and cricothyrotomy incision visible
- Make a transverse cricothyrotomy incision through the cricothyroid membrane (Figure 5). Anticipate some bleeding from the cricothyroid artery, a small branch of the superior thyroid artery which courses across the upper part of the cricothyroid membrane and communicates with the artery of the opposite side (Figure 6)
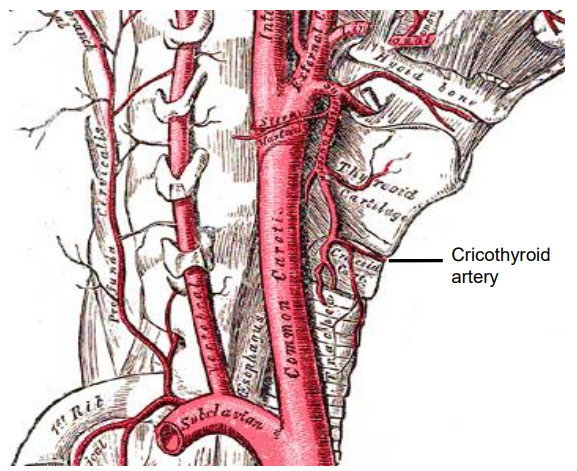
Figure 6: Cricothyroid artery branching from the superior thyroid artery
- Precisely determine the position of the anterior commissure, so that the thyrotomy is made through the anterior commissure. If this is not achieved, then either vocal cord will be damaged. The position of the anterior commissure can be determined by passing the tips of a small curved artery forceps through the cricothyrotomy, and cephalad between the vocal cords. By elevating the thyroid cartilage anteriorly with closed tips of the artery forceps, the artery will lodge in the anterior commissure, indicating precisely the line in which the thyrotomy should be made
- Vertically divide the thyroid cartilage in the midline aiming for the upturned tips of the artery forceps. This can be achieved with a scalpel; in older people with ossified cartilage it can be done with an oscillating saw or a heavy pair of scissors (Figure 7)
- Part the cut ends of the thyroid cartilage and inspect the endolarynx using an operating microscope or loupes if necessary (Figures 8, 9)

Figure 7: Completed thyrotomy
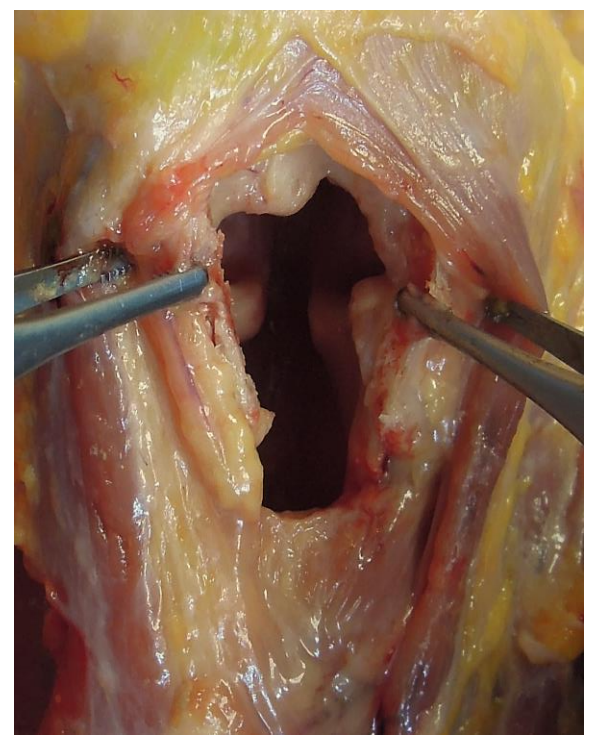
Figure 8: Note excellent view of the false vocal cords, ventricles, true cords and posterior larynx
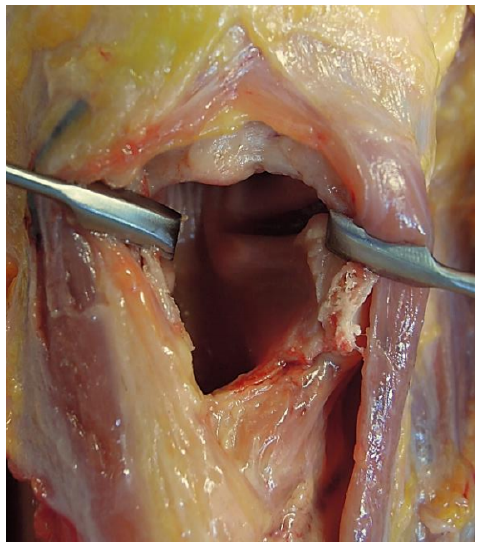
Figure 9: Note excellent view of false vocal cord, ventricle, true cord and subglottis
- A lesion of the glottis may then be excised under direct vision (Figures 10, 11)
- Reattach the anterior ends of the vocal cords to the cut edges of the thyroid cartilage with permanent monofilament material e.g. nylon to prevent retraction and shortening of the cords
- If there is a concern about webbing across the anterior commissure due to denuding of both vocal cords, a silastic keel can now be placed and secured (Figure 2)
- Reapproximate the cut edges of the cartilage accurately by using sutures or miniplates
- Suture the thyroid perichondrium
- Reapproximate the strap muscles in the midline
- Insert a pencil or corrugated drain to avoid surgical emphysema
- Suture the skin
- Remove the tracheostomy tube once the airway is adequate
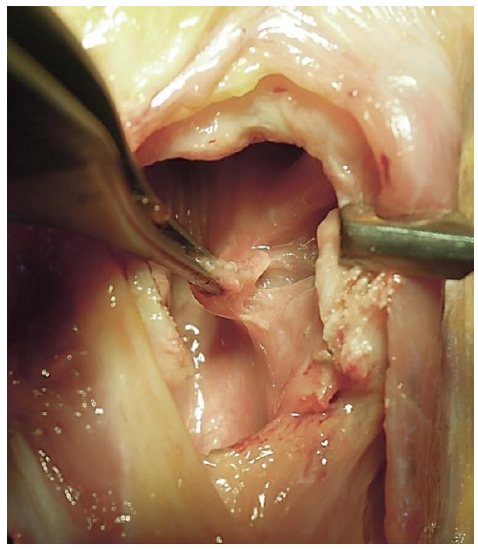
Figure 10: Lesion of glottis being excised
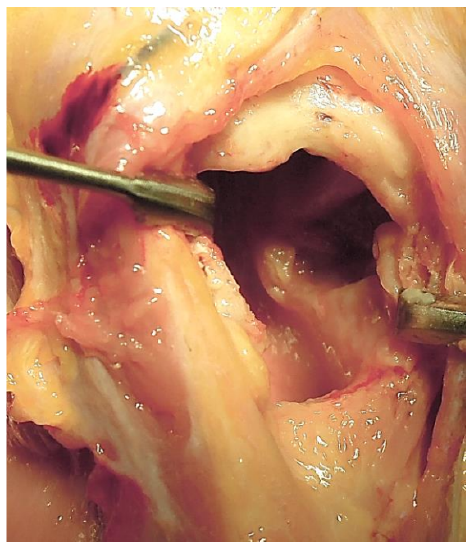
Figure 11: Cordectomy defect
Complications
- Webbing of anterior commissure; this is due to failure to reapproximate the vocal cords to the anterior edges of the laryngofissure, or not inserting a silastic keel when the opposing mucosae of the vocal cords have been traumatized
- Non-healing thyrotomy e.g. following previous radiation therapy
- Laryngocutaneous fistula: this generally closes spontaneously
- Malunion of the thyrotomy may cause a poor voice
Useful reference
Author and Editor
Johan Fagan MBChB, FCS(ORL), MMed
Professor and Chairman Division of Otolaryngology
University of Cape Town
Cape Town, South Africa
johannes.fagan@uct.ac.za

The Open Access Atlas of Otolaryngology, Head & Neck Operative Surgery by Johan Fagan (Editor) johannes.fagan@uct.ac.za is licensed under a Creative Commons Attribution - Non-Commercial 3.0 Unported License